
Abstract
Objective:
The study investigated the impact of potentially traumatic events on mental health outcomes among males who had ever served in the Australian Defence Force.
Method:
Data from a nationally representative household survey of Australian residents, the 2007 National Survey of Mental Health and Wellbeing, were used for this study.
Results:
Compared with community members, Australian Defence Force males were significantly more likely to have experienced not only deployment and other war-like events but also accidents or other unexpected events, and trauma to someone close. For non-deployed males, Australian Defence Force members were at increased risk of accidents or other unexpected events compared to community members. After controlling for the effect of potentially traumatic events that were more prevalent among all Australian Defence Force members, the increased risk of mental disorders among Australian Defence Force members was no longer evident. For non-deployed males, Australian Defence Force and community members were at comparable risk of poor mental health outcomes. A significant minority of Australian Defence Force members had onset of a mental disorder prior to their first deployment.
Conclusions:
Deployment and other potentially traumatic events among Australian Defence Force members can help to explain their increased vulnerability to mental disorders compared with community members. Providers should routinely enquire about a range of potentially traumatic events among serving and ex-serving military personnel.
Introduction
Military personnel are exposed to potentially traumatic events (PTEs) in their service. Exposure to combat and other deployment PTEs can have a significant impact on the mental health of serving and ex-serving military personnel (Hoge et al., 2004; Kulka et al., 1990). The experience of non-deployment PTEs among military personnel, such as childhood adversity, has also been shown to be an important predictor of mental health problems among active duty and treatment-seeking military populations (Cabrera et al., 2007; Forbes et al., 2013; Fritch et al., 2010; Sareen et al., 2013). These findings highlight the importance of deployment and non-deployment PTEs among military personnel and their impact on mental health.
Epidemiological studies have assessed the prevalence of mental disorders in serving and ex-serving military personnel (Iversen et al., 2009; Riddle et al., 2007; Sareen et al., 2007), with some studies making comparisons with the general population (McFarlane et al., 2011; O’Toole et al., 2009). For example, the 2010 Australian Defence Force (ADF) Mental Health Prevalence and Wellbeing Study (McFarlane et al., 2011) reported that the prevalence of affective disorders was significantly higher, and the prevalence of alcohol disorders was significantly lower, among current ADF personnel compared with Australian community members. The most frequently reported PTEs among ADF members were seeing serious injury or death (44.4%), sudden death of someone close (36.3%), peacekeeper or relief worker experience in a war zone (31.5%), combat experience (29.0%), life-threatening car accident (26.8%), mugged or threatened with a weapon (26.0%) and toxic chemical or harmful substance exposure (22.8%). Some studies have examined the prevalence and impact of certain types of trauma exposure among military personnel compared with the general community. For example, Afifi et al. (2016) found that almost half of all serving military personnel in Canada had a history of child abuse which was a higher rate than in the general community (Afifi et al., 2016). Woodhead et al. (2011) found that male ex-serving military personnel were more likely than community members to report childhood abuse and adversity and to have experienced a major trauma since the age of 16 years, with 34% reporting that the latter was related to an experiencein the military (Woodhead et al., 2011). However, to date, no known published studies have comprehensively examined trauma exposure among current or ex-serving military personnel compared with members of the general community.
Using data from the 2007 National Survey of Mental Health and Wellbeing (NSMHWB) in Australia, the aims of this study were, first, to compare exposure to PTEs among males who had ever served in the ADF with male members of the Australian general community; second, to assess whether the increased rate of mental health problems previously found among ADF members can be explained by their greater exposure to PTEs; and third, to investigate the onset of any mental disorder among ADF members relative to their first experience of combat or peacekeeping deployment.
Method
Sample
The 2007 NSMHWB (ABS, 2007) was based on a stratified, multistage area probability sample of residents aged 16–85 years in rural and urban private dwellings across all states and territories in Australia. Data were initially weighted according to the inverse of the probability of being selected in the survey. Person weights (used in this study) were then calibrated to independent estimates of population benchmarks in an attempt to reduce the sampling error of estimates and the level of non-response bias. The population benchmarks used in the NSMHWB included state by part of state by age by sex which was obtained from the 2006 Australian Census, as well as state by household composition, state by educational attainment and state by labour force status which were all obtained from the 2007 Australian Survey of Education and Work. The estimates calculated in this study are based on person weights calibrated to these benchmarks. Estimates of counts of persons were therefore obtained by summing person weights of persons with the characteristics of interest. Further details of the methods of the NSMHWB have been reported previously (Slade et al., 2009).
As part of the NSMHWB interview, respondents were asked whether they had ever served in the ADF and whether they had ever received a Department of Veterans’ Affairs (DVA) benefit. This study was based on the sub-sample of males who had served in the ADF (n = 447) compared with other males who had never served in the ADF or received a DVA benefit (n = 3544).
Measures
Socio-demographics
Prior to the formal mental health diagnostic interview, socio-demographic information was collected, including gender, age, marital status and current employment status.
PTEs
A modified version of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI) (Kessler and Ustun, 2004) was used to assess the presence of PTEs. Respondents were asked whether they had ever experienced 27 specific PTEs (Mills et al., 2011). For example, respondents were asked, ‘Did you ever participate in combat, either as a member of a military or as a member of an organised non-military group?’ to assess for combat exposure and ‘Did you ever serve as a peacekeeper or relief worker in a war zone or in a place where there was ongoing terror of people because of political, ethnic, religious or other conflicts?’ to assess for experience as a peacekeeper or relief worker in a war zone. In addition to questions about the 27 events, respondents were asked whether they had ever experienced any ‘other extremely traumatic or life-threatening event’ or a ‘private event’ they did not wish to talk about. To determine age at onset of each PTE, respondents were asked how old they were when it first happened to them. For example, if respondents indicated that they had experienced combat, they were asked, ‘How old were you when you had your first combat experience?’ Data on age at onset of PTEs were subsequently categorised in the ABS’ survey data files as follows: 1–20, 21–25, 26–30, 31–34 and 35 years or older.
For this study, the PTEs were grouped into seven categories based on similar categories used elsewhere (Searle et al., 2013). For example, the individual PTEs ‘Combat experience’ and ‘Peacekeeper or relief worker in a war zone’ were both included in the ‘Deployment’ category, and a respondent who answered in the affirmative to a question about one or both of these events was considered positive for ‘Deployment’. The age at onset of each PTE category was calculated as the earliest age at onset of individual PTEs within that category. The resultant PTE categories (and individual PTEs) were as follows: Deployment (combat experience, peacekeeper or relief worker in a war zone); Other war-like (saw atrocities or carnage [e.g. mutilated bodies], on purpose seriously injured, tortured or killed another); Accident or other unexpected trauma (life-threatening car accident, other life-threatening accident, life-threatening illness, toxic chemical or harmful substance exposure, natural disaster, man-made disaster, saw serious injury or death, accidentally caused serious injury or death); Sexual (raped, other sexual assault); Other interpersonal (kidnapped, badly beaten up by parents or caregiver, badly beaten up by spouse or partner, badly beaten up by someone else, as a child witnessed serious physical fights at home, mugged or threatened with a weapon, stalked); Civilian in war zone or refugee (unarmed civilian in war zone, civilian in region of terror, refugee); and Trauma to someone close (extremely traumatic event to someone close [e.g. rape], sudden death of someone close [e.g. accident, murder], had a child with life-threatening illness).
Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition mental disorders
The modified WMH-CIDI (Kessler and Ustun, 2004) was also used to assess the presence of Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) mental disorders. Diagnoses were based on standard WMH-CIDI algorithms with all DSM-IV hierarchical rules applied. Any affective disorder refers to the presence of depression, dysthymia and/or bipolar disorder; any anxiety disorder refers to the presence of agoraphobia, social phobia, panic disorder, generalised anxiety disorder, obsessive–compulsive disorder and/or posttraumatic stress disorder (PTSD); any substance use disorder refers to the presence of alcohol, cannabis, amphetamine, sedative and/or opioid abuse or dependence. Only lifetime disorders were considered in this study.
Psychological distress
The survey included the Kessler Psychological Distress Scale (K10). The K10 is a 10-item measure of non-specific psychological distress experienced in the past month that was developed specifically for use in epidemiological research (Kessler et al., 2002). Responses to each item are provided on a 5-point scale from 1 ‘none of the time’ to 5 ‘all of the time’, with higher scores indicative of higher distress. For use in logistic regression analyses, K10 scores were dichotomised as low (15 or less) or medium/high (greater than 15).
Self-assessed rating of physical health
Respondents were asked to rate their overall physical health on a 5-point scale of ‘excellent’, ‘very good’, ‘good’, ‘fair’ or ‘poor’. For use in logistic regression analyses, self-assessed physical health was dichotomised as excellent/very good or good/fair/poor.
Analyses
The estimated prevalence of individual PTEs was calculated for ADF males versus those males who had never served in the ADF.
Separate multiple logistic regression analyses were undertaken to calculate the weighted and adjusted odds ratios (ORs) and associated 95% confidence intervals (CIs) for the strength of association between military status and PTEs. Further multiple logistic regression analyses assessed the strength of the association between military status and mental disorders and psychological distress after controlling for each trauma category found to be more prevalent among ADF members. Similar to our previous report (McGuire et al., 2015), all multivariable analyses controlled for age, as well as marital, employment and physical health status variables.
All univariate and multivariable analyses were performed with weighted data and implemented using SURVEY procedures in SAS 9.2.
Results
Socio-demographics and physical health status
We have previously reported comparisons between male ADF (n = 447) and community members (n = 3544) on socio-demographic and physical health variables (McGuire et al., 2015). Briefly, ADF males were significantly more likely to be older; more likely to be widowed and less likely to be separated, divorced or never married; and less likely to be employed. Compared with males in the general community, they were also more likely to assess their physical health as good, fair or poor rather than excellent or very good.
PTEs
Table 1 shows comparisons between male ADF and community members on PTE categories (e.g. Deployment) and individual PTEs within each category (e.g. combat experience and peacekeeper or relief worker in war zone in the Deployment category). An individual could report experiencing more than one PTE within each PTE category which meant that the number of respondents who were positive for a PTE category (e.g. Deployment) could be less than the sum of respondents who reported individual PTEs within that category (e.g. combat experience and peacekeeper or relief worker in war zone). Compared to community members, ADF members were at increased risk of certain PTE categories (and individual PTEs within each category): Deployment events (combat experience and peacekeeper or relief worker in a war zone or region of terror); Other war-like events (seeing atrocities or carnage, on purpose seriously injured, tortured or killed another); Accident or unexpected event (life-threatening car accident, other life-threatening accident, toxic chemical or harmful substance exposure, natural disaster, man-made disaster and saw serious injury or death); and Trauma to someone close (sudden death of someone close). There were no differences between ADF and community members on the PTE categories of Sexual, Other interpersonal and Civilian in war zone or refugee. With regard to individual PTEs, ADF members were less likely to have been a civilian in a region of terror.
Comparison of potentially traumatic events (PTEs) among males who had ever served in the Australian Defence Force (ADF) and male community members.
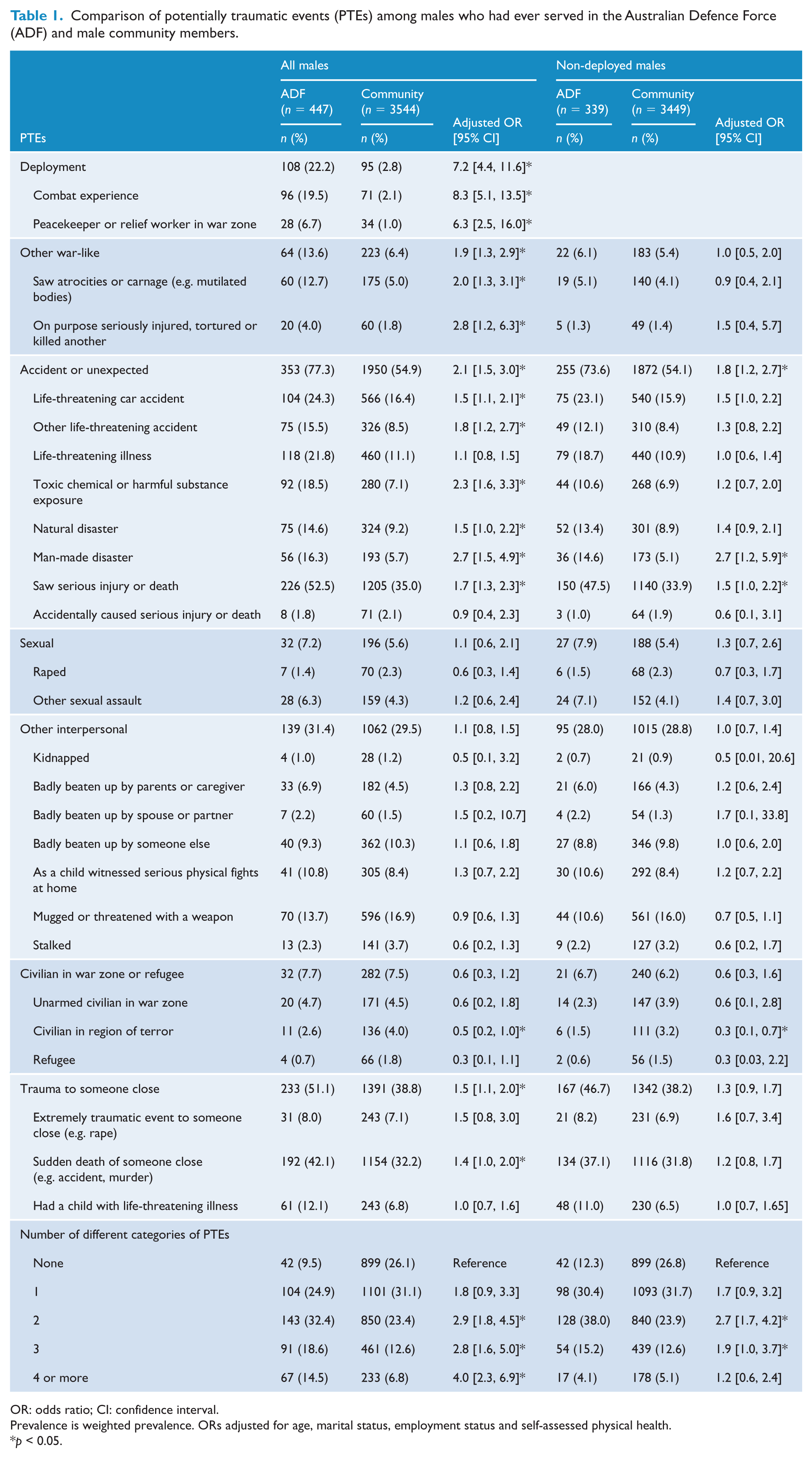
OR: odds ratio; CI: confidence interval.
Prevalence is weighted prevalence. ORs adjusted for age, marital status, employment status and self-assessed physical health.
p < 0.05.
When analyses were restricted to ADF (n = 339) and community members (n = 3449) without deployment experience, ADF members were at increased risk of the Accident or unexpected event PTE category, as well as man-made disaster and seeing serious injury or death; they were less likely to have been a civilian in a region of terror (see Table 1).
PTEs and mental disorders
As we have previously reported (McGuire et al., 2015), Model 1 in Table 2 shows that ADF members were significantly more likely to be diagnosed with any lifetime mental disorder, any affective disorder, depression, PTSD, any substance use disorder and alcohol use disorder, compared with community members. ADF members were also more likely to report higher psychological distress.
Comparison of lifetime mental disorder and recent psychological distress among males who had ever served in the Australian Defence Force (ADF) and male community members.
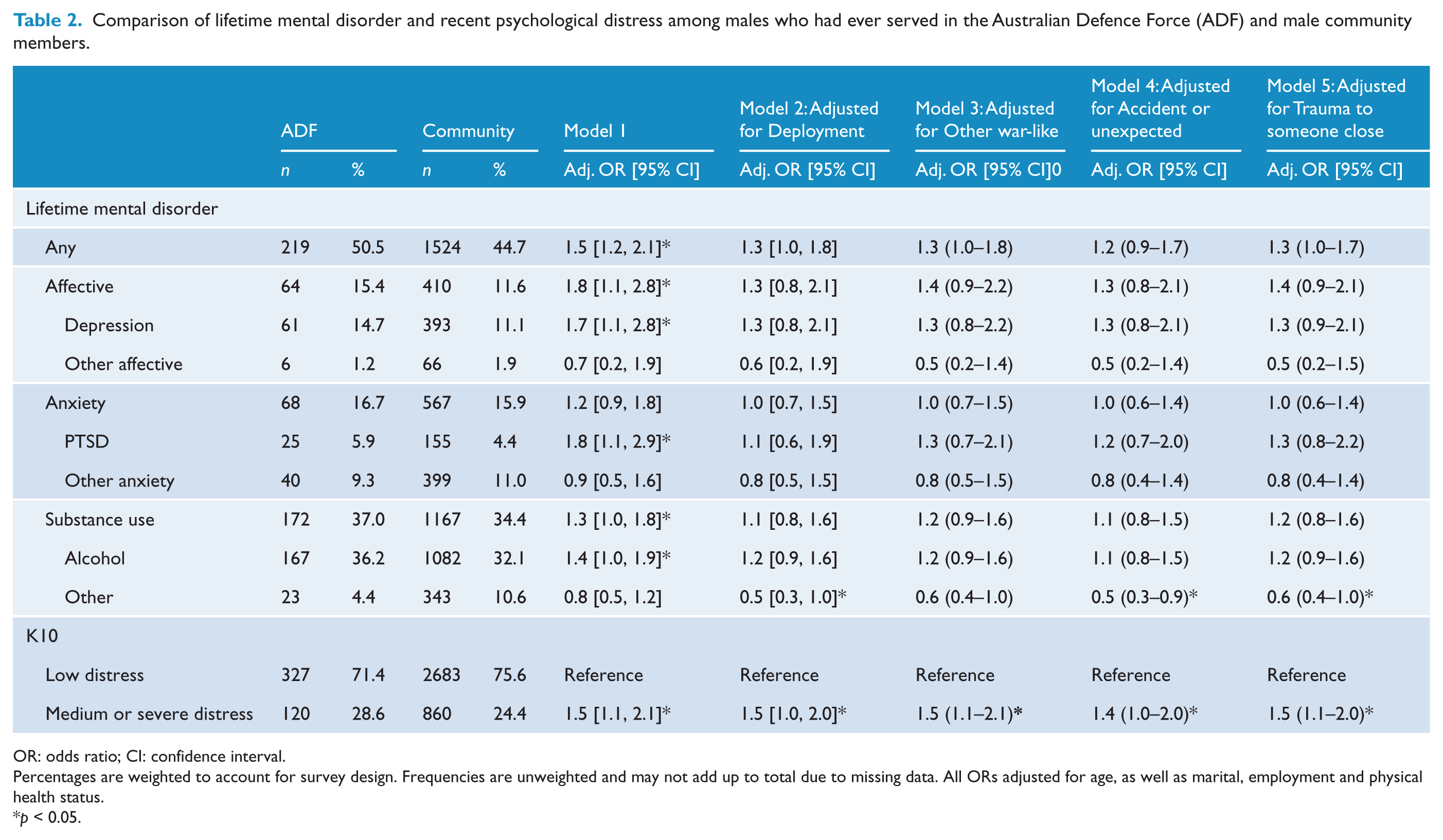
OR: odds ratio; CI: confidence interval.
Percentages are weighted to account for survey design. Frequencies are unweighted and may not add up to total due to missing data. All ORs adjusted for age, as well as marital, employment and physical health status.
p < 0.05.
Models 2–5 adjusted for the effects of each PTE category that was more prevalent among ADF members, that is, Deployment, Other war-like, Accident or unexpected and Trauma to someone close, respectively. After controlling for these effects, ADF members were no longer at increased risk of any mental disorder or individual mental disorders. Also, ADF members were at reduced risk of non-alcohol substance use disorder (except for Model 3), but remained at increased risk of higher psychological distress.
When the analyses were restricted to males without deployment experience, ADF members were not at increased risk of diagnosis of any or individual mental disorders, or psychological distress, compared with community members (results not shown but available upon request).
Onset of mental disorder and first experience of combat or peacekeeping
Table 3 shows the number of ADF members with onset of a mental disorder before, during the same period or after their first experience of combat or peacekeeping deployment. The data for age at first experience of deployment were only available on an interval scale. This meant that it was not possible to calculate the number of ADF members with onset of a mental disorder before their first experience of deployment if they were 20 years old or younger at the time or the number of ADF members with onset of a mental disorder after their first experience of deployment if they were 35 years or older at the time. With this in mind, the data show that a significant proportion of ADF members had onset of a mental disorder prior to their first experience of deployment. For all ADF members with available data (n = 108), onset of any mental disorder preceded first experience of deployment in 31.1% of cases. For those with complete data for temporality of events, that is, those whose first experience of deployment was between the ages of 21 and 34 years (n = 53), the onset of any mental disorder preceded first experience of deployment in 48.6% of cases.
Number and percentage of males who had ever served in the Australian Defence Force (ADF) with onset of mental disorders before, during the same period or after their first experience of deployment.
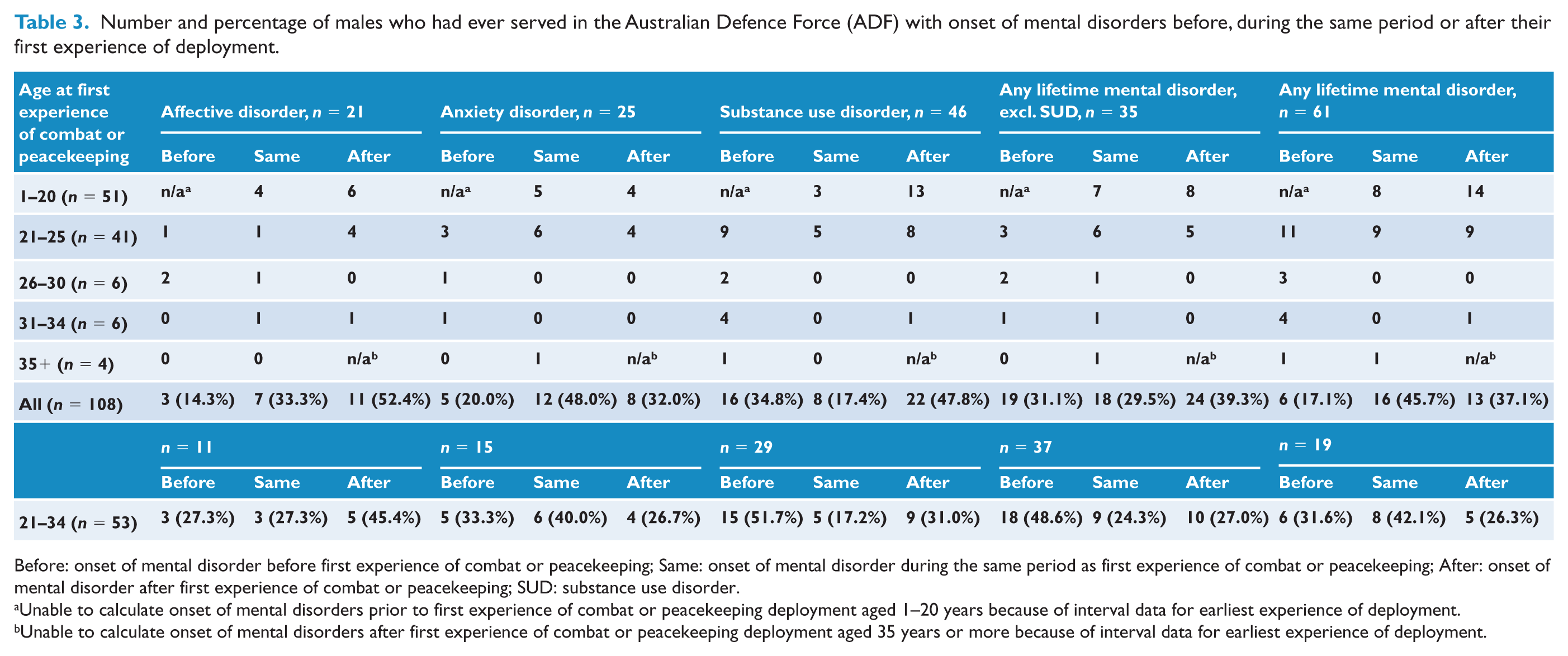
Before: onset of mental disorder before first experience of combat or peacekeeping; Same: onset of mental disorder during the same period as first experience of combat or peacekeeping; After: onset of mental disorder after first experience of combat or peacekeeping; SUD: substance use disorder.
Unable to calculate onset of mental disorders prior to first experience of combat or peacekeeping deployment aged 1–20 years because of interval data for earliest experience of deployment.
Unable to calculate onset of mental disorders after first experience of combat or peacekeeping deployment aged 35 years or more because of interval data for earliest experience of deployment.
Discussion
This study investigated exposure to PTEs and lifetime mental health outcomes among Australian males who had ever served in the ADF and male community members using a population-based survey. The main findings were as follows. First, ADF members were at increased risk of exposure to a range of PTE categories, not only deployment and other war-like events but also accidents or other unexpected events, and trauma experienced by someone close. They were not at increased risk of exposure to sexual, other interpersonal or being a civilian in a war zone or a refugee. For non-deployed males, ADF members were at increased risk of accidents or other unexpected events only. Second, after adjusting for the effects of those PTEs that were more prevalent among all ADF members, the increased risk of lifetime mental disorders among ADF members was no longer evident, although ADF members remained at increased risk of higher psychological distress. For non-deployed males, ADF and community members were at comparable risk of poor mental health outcomes. Third, a significant minority of ADF members reported that the onset of any mental disorder occurred before their first experience of combat or peacekeeping deployment.
This study extends our knowledge of the relative prevalence of PTEs among ex-serving military personnel compared with community members. ADF members were found to be more prone not only to deployment and other war-like PTEs but also accidents and disasters as well as trauma to someone close. Of course, it is quite feasible that at least some of these traumatic experiences, such as accidents, disasters and trauma to others, occurred while on deployment. This is supported by the finding that non-deployed ADF members compared with community members were only at increased risk of accidents or other unexpected events, notably man-made disaster and seeing serious injury and death. This pattern of findings indicates that deployment to combat or peacekeeping duties is frequently but not always implicated in exposure to PTEs among ADF members. It is possible that these experiences of trauma unrelated to combat or peacekeeping deployment took place in the course of other military duties, for example, training exercises or disaster relief operations. As other researchers have speculated, it is also possible that certain factors, such as providing assistance at accidents or working as volunteer emergency service workers, may make ex-serving personnel more likely to experience trauma not directly related to military service (O’Toole et al., 2009). It is also possible that at least some of these experiences of trauma unrelated to deployment took place prior to ADF service.
Compared with current serving ADF members in the 2010 ADF Mental Health Prevalence and Wellbeing Study (McFarlane et al., 2011), males who had served in the ADF in this study reported lower rates of combat experience (19.5% vs 29.0%) and peacekeeper or relief worker experience (6.7% vs 31.5%). No doubt these findings reflect a higher rate of deployment among recent cohorts of ADF members to combat operations in Iraq and Afghanistan, and peacekeeping missions in places such as Bougainville and East Timor. The lower rate of deployment among ADF males in this study may also help to explain their comparatively lower rate of being mugged or threatened with a weapon (13.7% vs 26.0%). The higher rates of life-threatening illness (21.8% vs 12.3%) and having a child with a life-threatening illness (12.1% vs 6.3%) among ADF males in this study are likely owing to their comparatively older age compared with current serving ADF members. Other than these findings, the rates of PTE exposure across both populations were quite similar.
The findings that ADF and community members were at comparable risk of sexual or other interpersonal PTEs, including being badly beaten up by parents or a caregiver, or as a child having witnessed serious physical fights at home, appear somewhat at odds with previous studies that found serving and ex-serving military personnel were more likely than community members to report childhood abuse (Afifi et al., 2016; Woodhead et al., 2011). Methodological differences may be an explanation for this apparent discrepancy. For example, Afifi et al. (2016) and Woodhead et al. (2011) both used a composite measure of childhood abuse compared with the indicators of individual PTEs used in this study.
The current finding that the increased vulnerability for lifetime mental disorders among ADF compared with community members disappeared after controlling for the effects of deployment is consistent with previous reports that the experience of combat and other deployment can have a lasting impact on the mental health of ADF members (O’Toole et al., 2009). It seems likely that the similar pattern of findings related to other PTEs, including other war-like experiences, accidents or other unexpected events and trauma experienced by someone close, was confounded by deployment experience. For example, an individual may witness the sudden death of someone close as well as other traumatic experiences while on deployment. This confounding explanation is supported by the fact that the sub-sample of non-deployed ADF members showed a reduced risk of PTEs relative to all ADF members and had a comparable risk of mental disorders and recent psychological distress as non-deployed community members. An interesting finding is that after controlling for the effects of deployment as well as other PTEs, ADF members continued to demonstrate an increased vulnerability for recent psychological distress compared with community members. We should not expect recent psychological distress to be concordant with a diagnosis of a lifetime mental disorder. Indeed, the NSMHWB data show that many individuals with medium to high distress on the K10 did notmeet criteria for a lifetime mental disorder. Taken together, these findings suggest that the increased risk of psychological distress among ADF members is not to trauma exposure. Other factors such as current psychosocial stressors may be contributing to this higher distress among ADF members.
It is perhaps not too surprising that a significant proportion of ADF members had onset of a mental disorder prior to their first deployment experience, given that age at first experience of deployment was most often during their mid-20s and that most individuals who develop a mental disorder will have done so by this age period (Kessler et al., 2005). Previous studies have also reported the presence of mental disorders among some military personnel prior to their first or subsequent deployment (Farmer et al., 2014; McFarlane et al., 2011).
This study has a number of limitations. First, there is no generally accepted method for categorising PTEs in a reliable and valid manner (Stein et al., 2012), and our results may have been influenced by the categorisation scheme we used. Second, it is not possible to know the extent to which the higher prevalence of deployment and other PTEs among ADF members can be directly attributed to military service. Despite this, more than one in five ADF members and relatively few community members reported deployment such as combat or peacekeeping in a war zone. Given these findings, it seems reasonable to assume that a high proportion of ADF males would have deployed on combat or peacekeeping duties while engaged in ADF military operations. The fact that the sub-sample of non-deployed ADF members showed a reduced risk of PTEs (relative to all ADF members) suggests that at least some reported traumatic experiences, such as witnessing atrocities, injuring or killing others, accidents and the sudden death of someone close, occurred while on deployment. It is also possible that the experience of deployment indirectly contributed to the experience of other traumatic experiences. For example, combat may result in an increased risk of car or other accidents due to a range of factors such as increased risk-taking, mental health problems, traumatic brain injury and post-service adjustment problems (Johnson, 2012). Third, the NSMHWB was designed to provide reliable estimates at the national level and there are risks of sampling errors when evaluating data relevant to smaller groups such as ADF members. In particular, only a relatively small number of ADF members were included in analyses examining the temporal relationship between onset of mental disorder and first experience of combat or peacekeeping. In addition, the interval-based data for first experience of combat or peacekeeping among ADF members meant that there were limited data to examine the temporal relationship between deployment and the onset of a mental disorder. As a result, these findings should be treated with some degree of caution. Finally, the utility of the data on ADF members would have been greater if they had been asked additional questions about the nature of their service, such as timing and duration of service, full-time or reserve service, and current or past serving ADF member.
Notwithstanding these limitations, this study was based on a population-based survey and found that males who had ever served in the ADF were at increased risk of a range of PTEs compared with community members and that this increased exposure to PTEs helped to explain their increased vulnerability to mental disorders. This study highlights the need for providers undertaking assessments for clinical, rehabilitation and compensation reasons to expand the scope of enquiry about PTEs among serving and ex-serving military personnel beyond ‘signature’ combat or other deployment events and to carefully assess the temporal onset of mental health problems relative to deployment and other traumatic experiences in order to better understand and treat mental health problems. The study findings also support routine, in addition to deployment-linked, mental health screening and intervention programmes for military personnel.
Footnotes
Additional information
Declaration of Conflicting Interests
Drs Wade, Varker, Phelps and Forbes are employees of Phoenix Australia and The University of Melbourne. Phoenix Australia is partially funded by the Australian Government Department of Veterans’ Affairs (DVA).
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.