
Abstract
Objective:
Children of parents with bipolar disorder (BD) are at heightened risk for developing mood and other psychiatric disorders. We proposed to evaluate the environment of families with at least one parent with BD type I (BDF) with affected offspring (aBDF) and unaffected offspring (uBDF) compared with control families without a history of DSM-IV Axis I disorder (CF).
Method:
We used the Family Environment Scale (FES) to evaluate 47 BDF (aBDF + uBDF) and 30 CF. Parents were assessed through the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I). Diagnosis of the offspring was determined through the Schedule for Affective Disorders and Schizophrenia for School-Age Children/Present and Lifetime Version (K-SADS-PL) interview.
Results:
There were statistically significant differences between aBDF, uBDF and CF in cohesion (p = 0.003), intellectual-cultural orientation (p = 0.01), active-recreational orientation (p = 0.007), conflict (p = 0.001), control (p = 0.01), moral-religious emphasis (p = 0.01) and organization (p = 0.001). The aBDF showed higher levels of control (p = 0.02) when compared to the uBDF.
Conclusions:
Families with a BD parent presented more dysfunctional interactions among members. Moreover, the presence of BD or other psychiatric disorders in the offspring of parents with BD is associated with higher levels of control. These results highlight the relevance of psychosocial interventions to improve resilience and family interactions.
Introduction
Children of parents with bipolar disorder (BD) are at heightened risk for developing mood disorders, adjustment problems and other psychiatric disorders, including social and academic difficulties and poor overall functioning (Birmaher et al., 2009; Singh et al., 2007). Offspring of parents with BD presented a 14-fold increase in rates of BD spectrum disorders and approximately a two- to threefold increase in any mood and anxiety disorders, when compared to offspring of parents without BD (Birmaher et al., 2009).
Bipolar disorder (BD) is considered a multifactorial illness with multiple gene and environmental factors implicated in its pathogenesis. Genetic load is the largest vulnerability factor reported in twin and adoption studies (Brietzke et al., 2012; Craddock and Sklar, 2013). In addition to genetic predisposition, some environmental high-risk factors have been postulated to be relevant in BD development. A positive family history of BD and other psychiatric conditions (psychosis, major depression, suicide and substance abuse disorder) are considered robust risk factors (Brietzke et al., 2012). Family stressors, such as marital difficulties, parenting problems, chronicity and severity of parental illness, are particularly relevant among children of affectively disordered parents (Jones and Bentall, 2008; Schenkel et al., 2008).
Investigating the family environment is important in order to understand the development and maintenance of severe psychopathologies (Repetti et al., 2002) and mood disorders in particular (Hooley and Parker, 2006; Miklowitz et al., 2004). Therefore, owing to the family environments’ pervasive influences on child development, poor family functioning may be an important environmental risk factor for developing BD (Schudlich et al., 1997). Previous studies used the Family Environment Scale (FES) to evaluate the family environment in parents (Chang et al., 2001; Romero et al., 2005), children and adolescents with BD (Belardinelli et al., 2008; Nader et al., 2013). Chang et al. (2001) reported lower cohesion and organization and higher levels of conflict in families with BD parents compared to normative (United States population) FES data. Similarly, Romero et al. (2005) reported lower cohesion and expressiveness scores in families with a parent with BD compared to families without any Axis I psychiatric disorders. Comparing the environment of families with BD children and adolescents to families with children without any Axis I psychiatric diagnoses, Belardinelli et al. (2008) and Nader et al. (2013) found lower levels of family cohesion and higher levels of conflict in BD families.
In this study, we used the FES to test the hypothesis that families with at least one parent with BD would present a more dysfunctional environment, specifically higher conflict and lower cohesion compared with families without any psychiatric diagnoses amongst members. In order to identify family environment characteristics that could be targeted for useful interventions, we compared the environment of families with BD parents with affected and unaffected offspring. Our secondary hypothesis was that families with BD parents whose offspring also had psychiatric disorders would have a profile suggestive of worse functioning. Lastly, we explored the clinical characteristics of affected offspring to identify any relationship between specific diagnoses and family environment characteristics.
Materials and methods
A total of 47 adult patients with BD type I, admitted to the Bipolar Disorder Program at the Institute of Psychiatry of the University of São Paulo, were interviewed by trained psychiatrists using the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Axis I Disorders (SCID-I) (First et al., 1995). Inclusion criteria for adult patients were: the presence of BD type I diagnosis according to DSM-IV, aged between 18 and 65 years old, and at least one offspring. Patients with schizophrenia, schizoaffective and schizophreniform disorders, and organic mental illnesses were excluded.
Offspring of BD parents had their diagnoses determined by trained researchers using the Schedule for Affective Disorders and Schizophrenia for School-Age Children/Present and Lifetime Version (K-SADS-PL) (Kaufman et al., 1997). Final diagnoses were assigned via consensus of child and parent interview and reviewed by child psychiatrists. BD offspring were included if they were aged between 6 and 17 years old.
Thirty parents, between 18 and 65 years old, and their offspring, aged 6 to 17 years old without any DSM-IV Axis I psychiatric disorders, were recruited. The children and adolescents were interviewed by means of the K-SADS-PL. All children and adolescents were excluded if they presented mental retardation or organic illnesses.
Parents were asked to complete the FES, a 90-item, true/false questionnaire, validated to Portuguese (Vianna et al., 2007). This family environment scale is composed of 10 different categories: cohesion (C), expressiveness (EX), conflict (CON), independence (IND), achievement orientation (AO), intellectual cultural orientation (ICO), active-recreational orientation (ARO), moral-religious emphasis (MRE), organization (ORG), and control (CTL). Parents were asked to answer the questions considering the overall environment and functioning of the family, and not based on a specific day or week. This scale has been recommended as a useful instrument for studying family environments (Moos and Moos, 2002). Moreover, the low cost and short time spent in its application makes it a feasible scale for clinical use (Ebesutani et al., 2012).
The sociodemographic characteristics are displayed in Table 1. There were no statistically significant differences in sociodemographic variables when we compared families with BD parents (BDF) and control families with no history of Axis I major psychiatric disorders (CF). When we compared families with BD parents with affected offspring (aBDF), families with BD parents with unaffected offspring (uBDF) and CF, there were no significant differences in sociodemographic variables except for the offspring’s ethnicity. The CF group had a higher number of African ethnicity offspring (36.7%; p = 0.04). However, when we divided our sample into families with Caucasian offspring and families with African offspring, we found no statistically significant difference in FES scores between the two groups.
Sociodemographic characteristics of families with BD parents (BDF) and control families with no history of psychiatric disorders (CF).
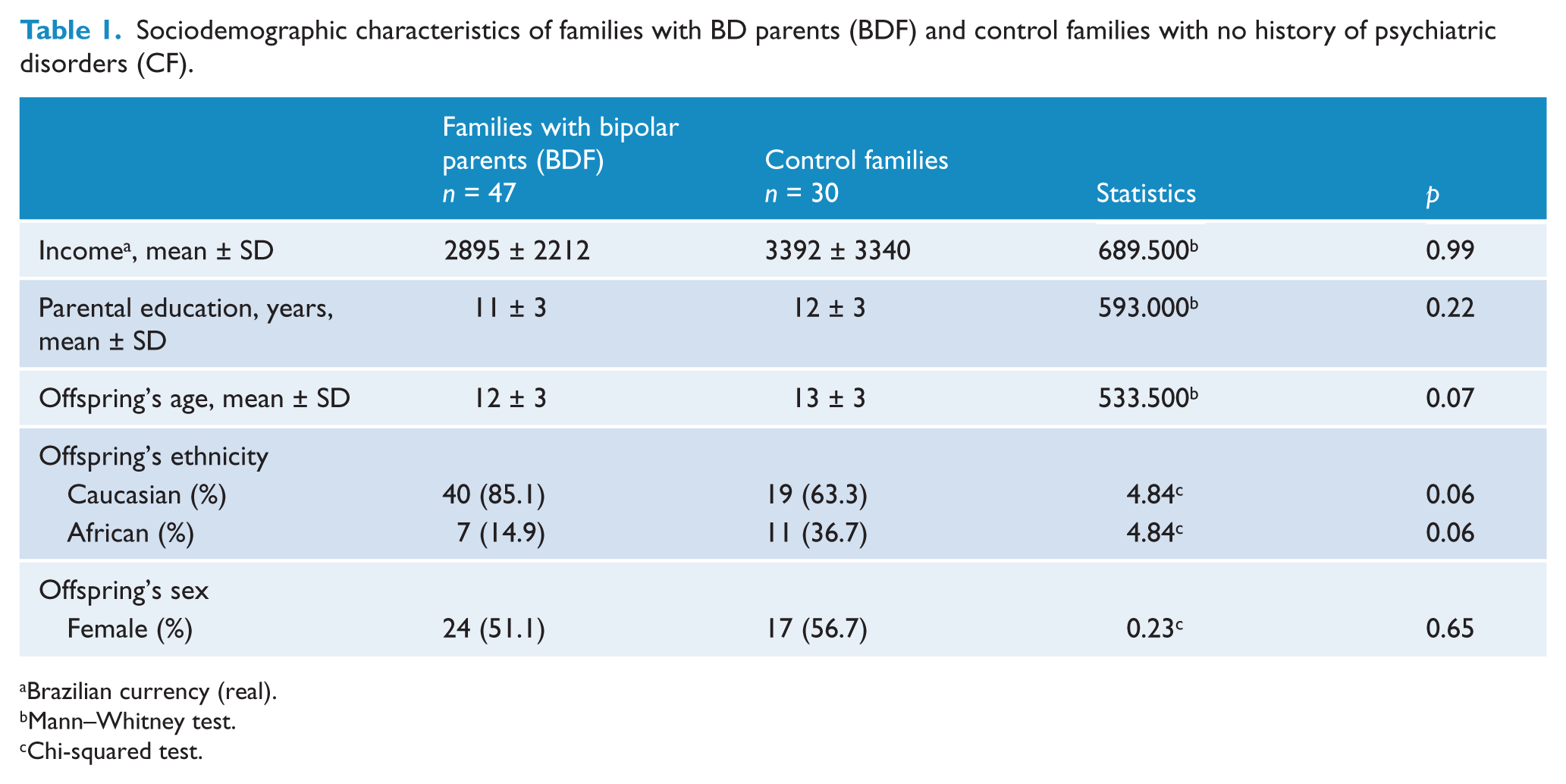
Brazilian currency (real).
Mann–Whitney test.
Chi-squared test.
Parents or legal guardians gave written informed consent and children and adolescents agreed to participate after the study was fully explained. This study had the University of São Paulo Ethics Committee approval.
Statistical analysis
Statistical analyses were conducted using the SPSS software version 14.0 for Windows (SPSS, Inc., Chicago, IL, USA), the level of significance was set at 5% and tests were two-tailed. The data assumption of normality was verified by the Kolmogorov–Smirnov test. Groups (BDF and CF) were compared using chi-squared tests for categorical variables. For variables with non-normal distribution, the Mann–Whitney U-test was used and a Bonferroni correction for multiple comparisons involving the 10 FES subscales was applied (p > 0.005). For the three-group comparison (aBDF, uBDF and CF) and subsequent pairwise comparisons, the Kruskal–Wallis test was used without correction for multiple comparisons.
Results
Family environment of BDF and CF
The family environment profile of BDF was significantly different from that of the comparison families and the scores are presented in Table 2. We found statistically significant differences on six of the 10 FES subscales. The BDF group presented lower cohesion (p = 0.001), intellectual-cultural orientation (p = 0.005), active-recreational orientation (p = 0.002), moral-religious emphasis (p = 0.004) and organization (p < 0.001), and higher conflict (p < 0.001).
Mean FES scores of families with BD parents (BDF) and control families without history of psychiatric disorders (CF) and statistics.
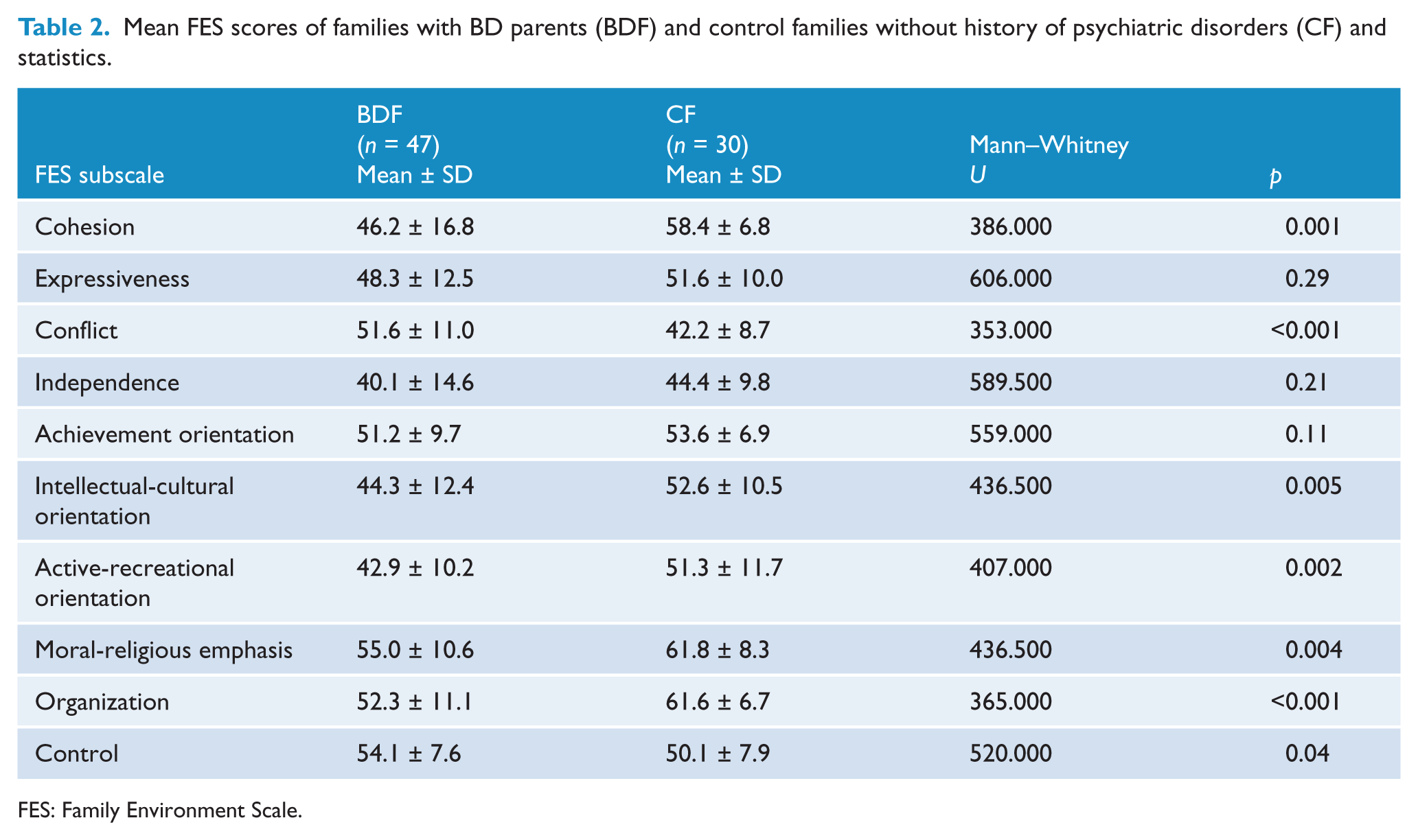
FES: Family Environment Scale.
Clinical characteristics of the affected offspring of BD parent
There was a higher frequency of psychiatric disorders (47%) among the offspring of BD parents, with a mean onset age of 13 years old. The affected offspring of BD parents presented a lifetime history of anxiety disorders (34%), attention deficit hyperactivity disorder (ADHD) (14.9%), BD (12.8%), major depressive disorder (MDD) (10.6%) and conduct or oppositional defiant disorders (8.5%).
Family environment of affected BD offspring (aBDF), unaffected BD offspring (uBDF) and control offspring with no history of DSM-IV Axis I psychiatric disorders (CF)
The aBDF group (n = 22) had average scores that were significantly different from uBDF (n = 25) and CF (n = 30) on five of the 10 FES subscales (Table 3). The aBDF group presented lower cohesion (p = 0.003), intellectual-cultural orientation (p = 0.01) and active-recreational orientation (p = 0.007) and higher conflict (p = 0.001) and control (p = 0.01) than CF and uBDF. The CF showed higher moral-religious emphasis (p = 0.01) and organization (p = 0.001) compared to the offspring groups. When we conducted a pairwise comparison between aBDF and uBDF, we found higher levels of control in the aBDF group (mean score ± SD = 56.9 ± 8.2 and 51.6 ± 6.1, respectively; Mann–Whitney U =170.000; p = 0.02).
Mean FES scores of families with BD parents with affected offspring (aBDF), families with BD parents with unaffected offspring (uBDF) and control families without history of psychiatric disorders (CF) and statistics.
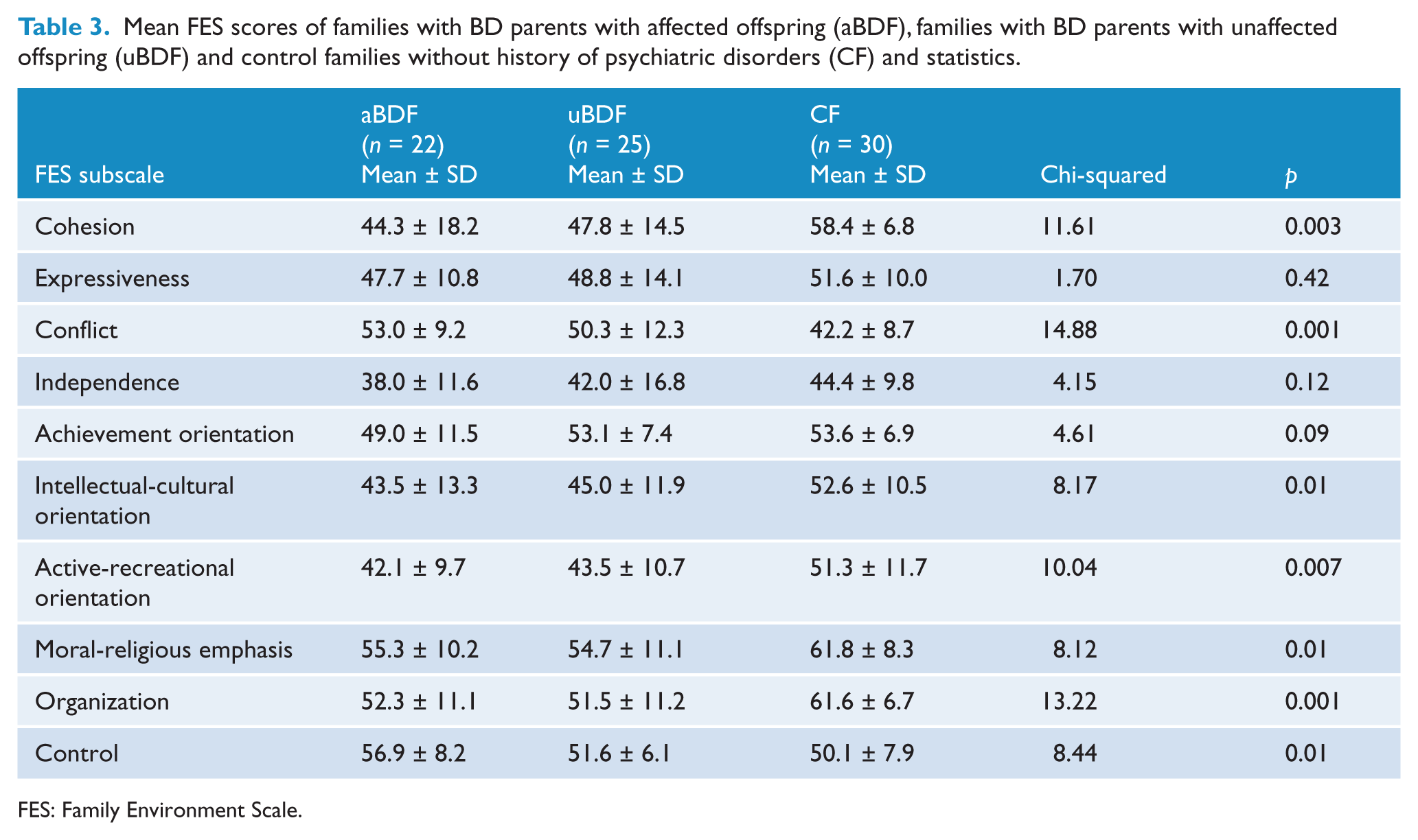
FES: Family Environment Scale.
Clinical characteristics of BD families and their relation with family environment features
The BDF were divided according to the presence or absence of different psychiatric diagnoses of their offspring: anxiety disorders, ADHD, BD, MDD and conduct or oppositional defiant disorders. In order to test the hypothesis that the presence of a specific psychiatric disorder in the offspring group would be related to different patterns of family functioning, we used the FES to compare the BDF with offspring that possessed each one of the above diagnoses, to BDF without that specific psychiatric disorder. However, we did not find statistically significant differences in FES domains in any of the comparisons.
Regarding history of psychotic symptoms, the BDF whose parents presented a history of psychotic symptoms had lower organization scores when compared to BDF with non-psychotic parents (mean score ± SD = 58.85 ± 7.71 and 49.91 ± 11.28, respectively; Mann–Whitney U = 118.500; p = 0.01).
Lastly, we compared the FES subscale scores between BDF with one BD parent and one parent without a mood disorder – unilineal (n = 41, 87.2%) to BDF with both parents with any mood disorder – bilineal (n = 6, 12.8%). We found higher moral-religious emphasis scores in bilineal BDF compared to unilineal BDF (mean score ± SD = 62.67 ± 6.06 and 53.88 ± 10.75, respectively; Mann–Whitney U = 60.500; p = 0.04).
Discussion
The comparison of family environment between BDF and CF revealed significant differences on six of the FES domains. Consistent with previous results, our families with BD parents presented lower cohesion (Chang et al., 2001; Romero et al., 2005), intellectual-cultural orientation (Chang et al., 2001; Romero et al., 2005), moral-religious emphasis (Romero et al., 2005) and organization. Neither Chang et al., 2001 nor Romero et al., 2005 found significant differences in active-recreational orientation domain when comparing BDF to CF or to the FES normative data. (Chang et al., 2001), as well as higher levels of conflict (Chang et al., 2001; Romero et al., 2005). The reiteration of previous findings in the literature, although in a different cultural context (shown here by the Brazilian family environment), provides a clear indicator that the dysfunctional family characteristics related to BD parents are independent of socio-cultural environments found in western societies.
In agreement with previous studies, we found a higher frequency of different psychiatric disorders in our BD offspring sample (Birmaher et al., 2009; Mesman et al., 2013; Vandeleur et al., 2012; Zappitelli et al., 2011). Similarly to our study, Birmaher et al. (2009) found that 52.1% of BD offspring (n = 388, mean age = 11.9 years) presented a DSM-IV Axis I psychiatric diagnosis, 25.8% an anxiety disorder and 10.6% a BD diagnosis. BD offspring are at a heightened risk to develop not only BD, but also psychopathologies in general and the psychiatric disorders rates seem to increase with age. In the 12-year follow-up of the Dutch bipolar offspring cohort (n = 108; age range at baseline = 12–21 years), 72% of the BD offspring developed a DSM-IV Axis I disorder and 13% were diagnosed with BD (Mesman et al., 2013).
Our results indicate that families whose affected offspring of BD parents with any DSM-IV Axis I psychiatric disorder (aBDF) are characterized by higher levels of control compared to families of unaffected offspring of BD parents (uBDF). Since control scores are indicators of how much rules and procedures are used to run family life (Moos and Moos, 2002), one may assume that the higher control scores found in aBDF could be an attempt to deal with the possibly altered functioning pattern of BD families (Chang et al., 2001).
Romero et al. (2005) did not find any difference in FES scores when comparing the environment of families of BD parents with and without BD children. Likewise, when we divided the BDF group in offspring with and without BD, we did not find statistically significant differences in any FES subscales scores. Moreover, when we divided the BDF into subgroups with and without a specific offspring diagnosis and compared them against each other, there were no statistically significant differences found in the FES scores. The higher levels of control in aBDF compared to uBDF were not associated with a specific psychiatric disorder in the offspring. This may be a family characteristic that is non-specifically associated with overall child psychopathology.
To verify whether the presence of mood disorders in both parents would be related to a worse family functioning, we compared the familial environment of bilineal versus unilineal BDF. There were no significant differences, except for higher scores of moral-religious emphasis in bilineal BDF. This could be related to a strong religious and spiritual belief held by most of the BD patients (Cruz et al., 2010; Mitchell and Romans, 2003), and indicates that families with both parents affected could be more prone to emphasize religiosity.
We also found lower organization scores in BDF with psychotic BD parents compared to BDF with BD parents without any history of psychotic symptoms. This is in line with the context of a broader psychosis definition that would also include a disorganized thought process and grossly disorganized behavior.
Recent psychosocial interventions have been developed in order to prevent the incidence of psychopathology among children of parents with a mental illness (COPMI) (Reupert and Maybery, 2009). In general, these programs aim to enhance coping, self-esteem, resilience and understanding of mental illnesses. For example, Fraser and Pakenham (2008) evaluated the effectiveness of a group-based intervention (n = 27) in comparison with a waiting list control condition (n = 17) for psychiatric patients’ offspring aged 12–18 years old. After an 8-week follow-up, the intervention group showed clinically significant improvements in mental health literacy, depression, and life satisfaction. According to our results of less cohesion in BD families, it is recommended that interventions for BD offspring also address how these children could find support on other social networks. As a matter of fact, low social support predicts higher levels of depression over time in BD patients (Johnson et al., 2003) and may be related to resilience and psychopathology onset.
To the best of our knowledge, the BD literature lacks psychosocial studies directed at unaffected offspring. Miklowitz and colleagues (2011) adapted the family-focused therapy in an open trial that included 13 children ranging from 9 to 17 years old. This cohort had at least one BD parent and a lifetime diagnosis of BD-NOS (not otherwise specified), MDD or cyclothymic disorder. After a year, 11 subjects showed a moderate improvement in the depression severity scale (p = 0.013) and a significant improvement on the mania rating scale (p < 0.001), whilst nine (82%) subjects experienced a reduction in the Adolescent Longitudinal Interval Follow-up Evaluation (A-LIFE).
These promising interventions were focused on clinical outcomes and did not assess family characteristics. The family function includes factors such as cohesion, harmony and the ability to deal with conflicting issues. These characteristics can have a profound impact on the experiences of children and their life trajectories, playing an important role in emotional development during childhood (Cuffe et al., 2005), as well as adding to the risk of mood disorders (Althoff et al., 2005; Yap et al., 2007). In families with BD adolescents, family interventions have already demonstrated their efficacy in reducing expressed emotion (Miklowitz et al., 2009). High levels of expressed emotion are related to higher levels of criticism and this association could be explained by an increase in conflict levels. Further family intervention studies on unaffected children are needed to address the impact on conflict levels.
An important limitation of our study regards the relatively small sample size when we divided the aBDF into the different psychiatric diagnoses. This may have hindered us from detecting differences in FES subscales that are associated with specific offspring psychiatric disorders. Another limitation is that our study was based on a self-report questionnaire, which may render our findings more dependent on the individual and on the parents’ subjective perception, rather than an observation-based evaluation rating. One may argue that the presence or absence of a mood disorder in the respondent parent could have an impact on his or her perception of the family. However, previous studies demonstrated high concordance rates between affectively disordered parents and their non-affected spouses in their ability to report family environmental characteristics (Billings and Moos, 1983; Romero et al., 2005). Recruiting subjects through an advertisement could be associated with a possible selection bias, facilitating the inclusion of better informed and treatment-seeking families that are not representative of the general population. Finally, the information was collected from the parents only and thus the offspring’s impressions of family functioning were not included.
In summary, our results suggest that altered family environments are related not only to BD in parents but also to the presence of offspring psychopathology. However, owing to its cross-sectional design, our study could not determine causality between both factors. Thus, larger and longitudinal studies are necessary to clarify such points and further determine family environment abnormalities that may be future targets for specific family-focused interventions.
Footnotes
Funding
This research was supported in part by Fundação de Amparo a Pesquisa de São Paulo, Brazil (FAPESP); Conselho Nacional de Desenvolvimento Cientifico e Tecnológico, Brazil (CNPq); the National Alliance for Research on Schizophrenia and Depression (NARSAD), Young Investigator; the American Psychiatric Association/AstraZeneca Young Minds in Psychiatry International Awards; and the L’Oréal-ABC-Unesco – Para Mulheres na Ciência, Brazil.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.