
Abstract
Objective:
Prisoners with intellectual disability who have a coexisting mental health issue often have unmet health needs and are more likely to reoffend than those with intellectual disability alone. The aims of this study were to estimate the prevalence of co-occurring mental disorder among prisoners with intellectual disability and to explore the association between intellectual disability and mental disorder.
Methods:
Cross-sectional study of adult prisoners within 6 weeks of release from custody in seven prisons in Queensland, Australia between August 2008 and July 2010. Intellectual disability was assessed using a practical composite screening tool. Prisoners who scored <85 on the Hayes Ability Screening Index and reported either having attended a special school or having been diagnosed with intellectual disability were identified as having an intellectual disability. Mental health was assessed using self-reported psychiatric diagnoses, the Kessler Psychological Distress Scale (K-10), and the Mental Component Summary score of the Short-Form-36 health survey version 2. The association between intellectual disability and mental health was assessed using univariate and multivariate logistic regression.
Results:
Overall, 1279 prisoners completed the HASI: 316 (24%) scored below the recommended cut off for further diagnostic assessment of intellectual disability, 181 (14%) reported attending a special school, and 56 (4%) reported that they had been diagnosed with an intellectual disability. On our composite measure, 115 (9%) participants were identified as having an intellectual disability. Among prisoners with intellectual disability, the estimated lifetime and current prevalence of co-occurring mental disorders was 52.5% (95% CI 43.3–61.5) and 37.2% (95% CI 28.8–46.5), respectively. Of those with intellectual disability, 13.5% (95% CI 8.3–21.1) reported very high psychological distress, as measured by the K10. Prisoners with intellectual disability were significantly more likely than their non-disabled peers to report a current diagnosis of depression [adjusted odds ratio (AOR) 1.8, 95% CI 1.1–3.2] or substance dependence (AOR 3.7, 95% CI 1.6–8.4], after adjusting for potentially confounding variables. Prisoners with intellectual disability were also significantly more likely than their non-disabled peers to use antipsychotic medication (AOR 1.7, 95% CI 1.0–2.8).
Conclusions:
Prisoners with an intellectual disability were more likely than their non-disabled peers to have elevated rates of psychiatric comorbidity and unmet treatment needs. There is a need for enhanced collaboration between specialist intellectual disability psychiatric services and mainstream prison mental health services, to ensure coordinated service delivery for this dually disadvantaged group.
Introduction
Adults with an intellectual disability are significantly over-represented among prisoners in many Western jurisdictions including the USA, UK, Ireland, Norway, and Australia (Hayes and McIlwain, 1988; Veneziano and Veneziano, 1996; Petersilia, 1997; Murphy et al., 2000; Hayes et al., 2007; Søndenaa et al., 2008). Adults with intellectual disability in the general population are substantially more at risk of developing a range of mental disorders than are their non-disabled peers (Holland and Koot, 1998; Lunsky and Palucka, 2004). Many of the important risk factors for mental disorder, such as genetic anomalies, brain damage, adverse drug effects, institutionalized background, disadvantaged lifestyles, social marginalization, low self-worth, and limited coping skills, are prevalent among people with an intellectual disability (Moss et al., 1998).
There is increasing international concern about the particularly vulnerable subset of prisoners with intellectual disability who have a coexisting mental health issue [so-called “dual diagnosis” (White et al., 2005) or “dual disability”]. These individuals are more likely than those with intellectual disability alone to reoffend (Klimecki et al., 1994) and pose a complex challenge to forensic mental health services. Service delivery for this group of offenders has long been fragmented (Simpson et al., 2001). As poor mental health is an important predictor of both preventable mortality and recidivism in ex-prisoners (Bonta et al., 1998; Kariminia et al., 2007; Fazel et al., 2009; Pratt et al., 2010), improving mental health outcomes among prisoners and ex-prisoners is important from both a health and a criminal justice perspective.
Few studies have examined the association between intellectual disability and mental illness in prisoners, or examined the health needs of prisoners with co-occurring disorders. Most of these studies have relied on administrative data (e.g. prisoners registered with disability services) or convenience samples (e.g. segregated prison units specifically for offenders with intellectual disability). In one retrospective study of offenders judged unfit to stand trial due to intellectual disability, at a secure forensic hospital in Florida, USA, the prevalence of mental illness was 52.3% (Ho, 1996). However, these findings were based on a review of offender files and it is not clear what criteria were used to assess psychiatric disorders. Two older Australian studies identified a high prevalence of prior psychiatric contact (75%) (Klimecki et al., 1994) and major psychiatric diagnosis (29%) (Glaser and Deane, 1999) among offenders with intellectual disability in segregated prison populations and specialist prison units respectively.
There is little research concerning prisoners with intellectual disability and co-occurring mental illness in the mainstream prison population. One recent cross-sectional study of a large, representative sample of prisoners in England and Wales found elevated rates of psychosis in prisoners with intellectual disability, although this relationship was fully mediated by self-reported general health status (Hassiotis et al., 2011). A recent Australian study investigating physical health outcomes among the same cohort of prisoners examined in the current study demonstrated that those with intellectual disability are characterized by increased somatic morbidity and lower preventive health service utilization (Dias et al., 2012). Given the increasing recognition of the nexus between mental health and physical health among prisoner populations (Butler et al., 2007), psychiatric comorbidity is of particular concern in this invisible subgroup of offenders. The aims of this study were to estimate the prevalence of co-occurring mental disorders separately in prisoners with and without intellectual disability and to explore the association between intellectual disability and mental disorder.
Methods
Study design and setting
This cross-sectional study was conducted among adult prisoners in seven correctional centres in Queensland, Australia, between August 2008 and July 2010. The data for this study served as baseline data for a randomized controlled trial designed to evaluate the impact of personalized service brokerage on health service utilization and health outcomes within the first 6 months of release from custody (Kinner et al., 2008, 2010). Randomization occurred after baseline interview.
Participants and procedures
Eligible participants were sentenced prisoners (full-time or parole) who were scheduled to be released from custody within 6 weeks, who provided informed, written consent for participation. Remand prisoners were excluded due to uncertainty regarding release dates. Women were oversampled to increase statistical power for gender-specific analyses. Ethics approval for the study was granted by the University of Queensland’s Behavioural and Social Sciences Ethical Review Committee.
Baseline data were collected via face-to-face administration of a structured questionnaire in confidential interviews conducted by trained interviewers. The questionnaire covered demographic information, social, and criminological characteristics, general health, mental health, and health risk behaviours. Interviews took approximately 60 minutes to complete.
Mental health measures
Information was collected on self-reported lifetime and current psychiatric diagnoses (as told by a doctor, psychologist, or psychiatrist). Measures of mental health included the Kessler Psychological Distress Scale (K-10) (Kessler et al., 2002) and the Mental Health Component Summary (MCS) score of the Short-Form-36 health survey version 2 (SF-36v2; Ware et al., 2000; Ware, 2002). The K10 is a 10-item screening tool for symptoms of anxiety and depression in the previous 4weeks. Scores can range from 10 to 50 and high scores (≥30) are indicative of moderate-to-severe mental illness (Andrews and Slade, 2001). The MCS is a widely used measure of functional health status, derived using a weighted combination of scores on the eight sub-scales of the SF-36v2, and provides a measure of overall mental health-related functioning. It has been shown to be useful in screening for psychiatric disorders (Ware et al., 1994). MCS scores were computed using Australian weights (Hawthorne et al., 2007) to give the MCS a population mean of 50 and standard deviation (SD) of 10.
Information on current use of prescribed psychiatric medication was abstracted from prison medication charts and was categorized according to the Monthly Index of Medical Specialities (MIMS), a comprehensive medicine database (www.mimsonline.com). Additionally, information was collected on lifetime history of self-harm and suicide attempts, involuntary psychiatric treatment, and engagement with prison mental health transitional services.
Presence of intellectual disability
Participants with intellectual disability were identified using a pragmatic screening method involving the Hayes Ability Screening Index (HASI) (Hayes, 2000). The HASI correlates significantly with standardized tests of intelligence and adaptive behaviour and is widely used to screen for intellectual disability among prisoners and similar population groups (Hayes, 2000). Due to its intentionally over-inclusive design as a screening tool, it is likely to identify prisoners with other types of cognitive impairment and mental illness and those with poor English language skills. To account for this over-inclusiveness, we included the HASI as part of a constructed composite measure to identify participants with intellectual disability (Dias et al., 2012). We increased its specificity (predictive accuracy) by combining HASI scores with two reliable markers of intellectual disability: lifetime diagnosis of intellectual disability and special school attendance. We defined an individual as having intellectual disability if their HASI score was below the standard cut off of 85 and they reported that they had either attended a special school or received a life-time diagnosis of intellectual disability from a doctor or other health professional.
Other measures
Demographic and general health variables included age (<25 or ≥25 years), gender, Indigenous status, and self-evaluated general health status (excellent, very good, good, fair, or poor). Participants who identified as Aboriginal, Torres Strait Islander, and/or South Sea Islander were defined as Indigenous; all other participants were defined as non-Indigenous. Socioeconomic variables included highest level of education (<10 or ≥10 years of school), employment status (employed or unemployed) in the 6 months before imprisonment and accommodation status (unstable or stable housing) in the month prior to imprisonment. Criminogenic variables included number of juvenile imprisonments (0 or ≥1 imprisonments), prior adult incarceration (0 or ≥1 prior imprisonments), sentence length (<1 or ≥1 years) and parole status on release (yes or no).
Statistical analysis
Continuous variables were summarized as mean±SD, categorical variables as n (%) and prevalence as % (95% confidence interval). The associations between intellectual disability and markers of mental disorder were examined using univariate and multivariate logistic regression analyses. Variables adjusted for in the multivariate analyses were either identified a priori based on previous research (age, sex, Indigenous status, and general health) or were included via screening as they were significantly associated with intellectual disability at the p<0.05 level in a univariate logistic regression model. The association between intellectual disability and MCS score was investigated using linear regression. All analyses accounted for the oversampling of females in the parent trial and were conducted using Stata version 10.3 (Stata Corp, College Station, TX, USA).
Results
The sample included 1325 participants. No potential participant was excluded due to inability to provide informed consent to participate. Participants were similar to the 10,931 prisoners released from adult prisons in Queensland during the study period in terms of age (mean of 33 vs. 33 years) and Indigenous status (24 vs. 30% Indigenous). A total of 1279 (97%) participants completed the HASI; the mean scores were 88.4±9.2, with 316 (24%) scoring below 85. There were 181 (14%) participants who reported attending a special school and 56 (4%) reported that they had been diagnosed with an intellectual disability. Overall, 115 (9.0%) participants were identified as having an intellectual disability. Participants with an intellectual disability were more likely than those without an identified intellectual disability to be male (p<0.001), Indigenous (p=0.04), to have <10 years of formal education (p<0.001), to report unstable accommodation in the month before they came to prison (p=0.003), to have a history of juvenile imprisonment (p=0.043), and to report poorer self-evaluated general health (p=0.013) (Table 1). Consequently potentially confounding variables included in all subsequent multivariate models were age, sex, Indigenous status, education level, general health status, accommodation status, and juvenile imprisonment history.
Demographic, socio-economic, and criminological characteristics according to intellectual disability status.
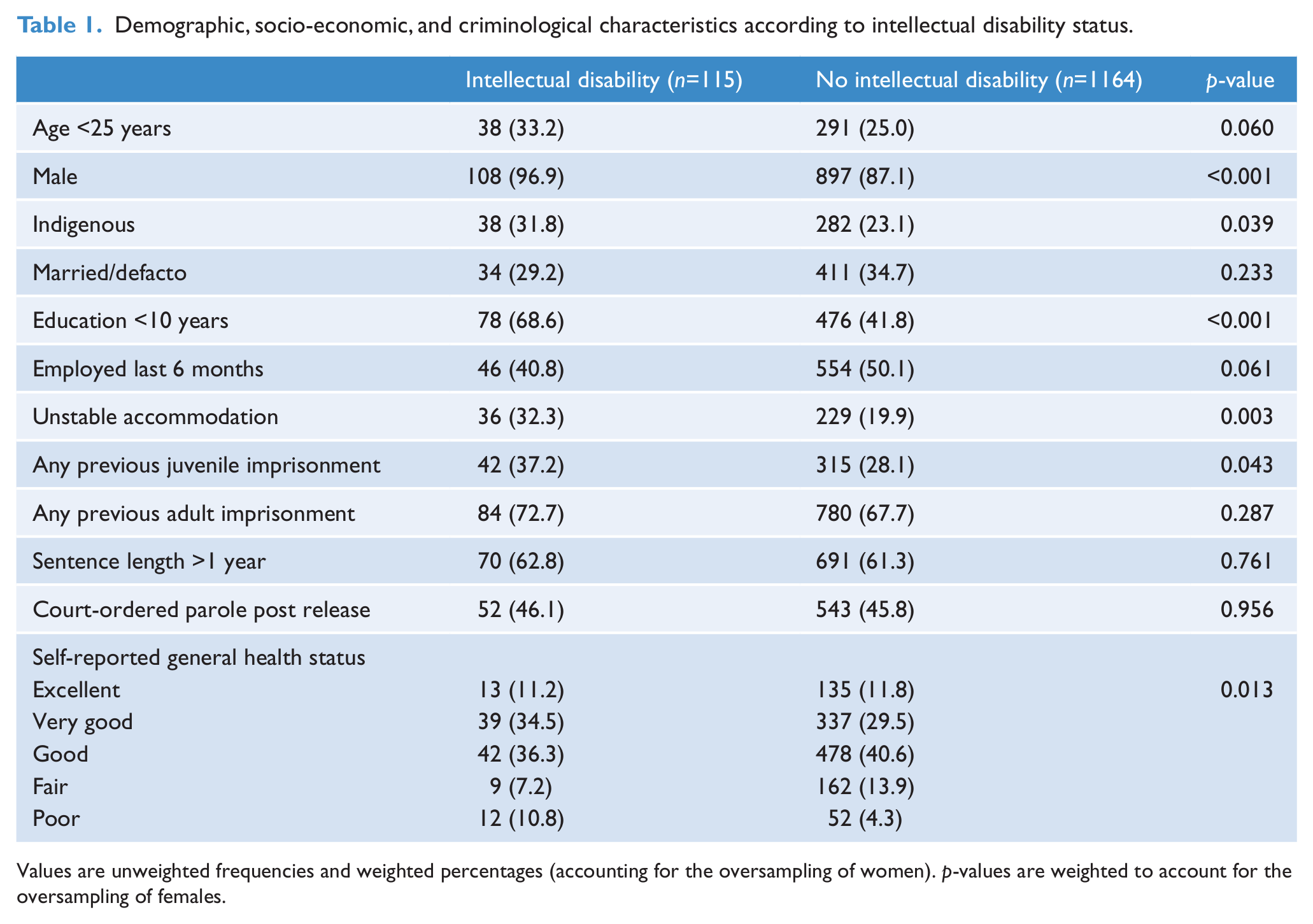
Values are unweighted frequencies and weighted percentages (accounting for the oversampling of women). p-values are weighted to account for the oversampling of females.
The lifetime prevalence of coexisting mental disorder among prisoners with intellectual disability was 52.5% (95% CI 43.3–61.5%), compared with 41.7% (95% CI 38.8–44.7%) in the non-disabled mainstream prisoner population. The adjusted odds of prisoners with intellectual disability reporting lifetime mental disorder were nearly double those of their non-disabled peers [adjusted odds ratio (AOR) 1.7, 95% CI 1.1–2.5; Table 2]. The overall percentage of prisoners in the mainstream population who had both an intellectual disability and had received a psychiatric diagnosis in their lifetime was 5.1% (95% CI 4.0–6.6%).
Association between intellectual disability and self-reported psychiatric diagnosis, mental health screening measures, psychotropic (CNS) medication, mental health service contact, suicide attempts, and self-harm.
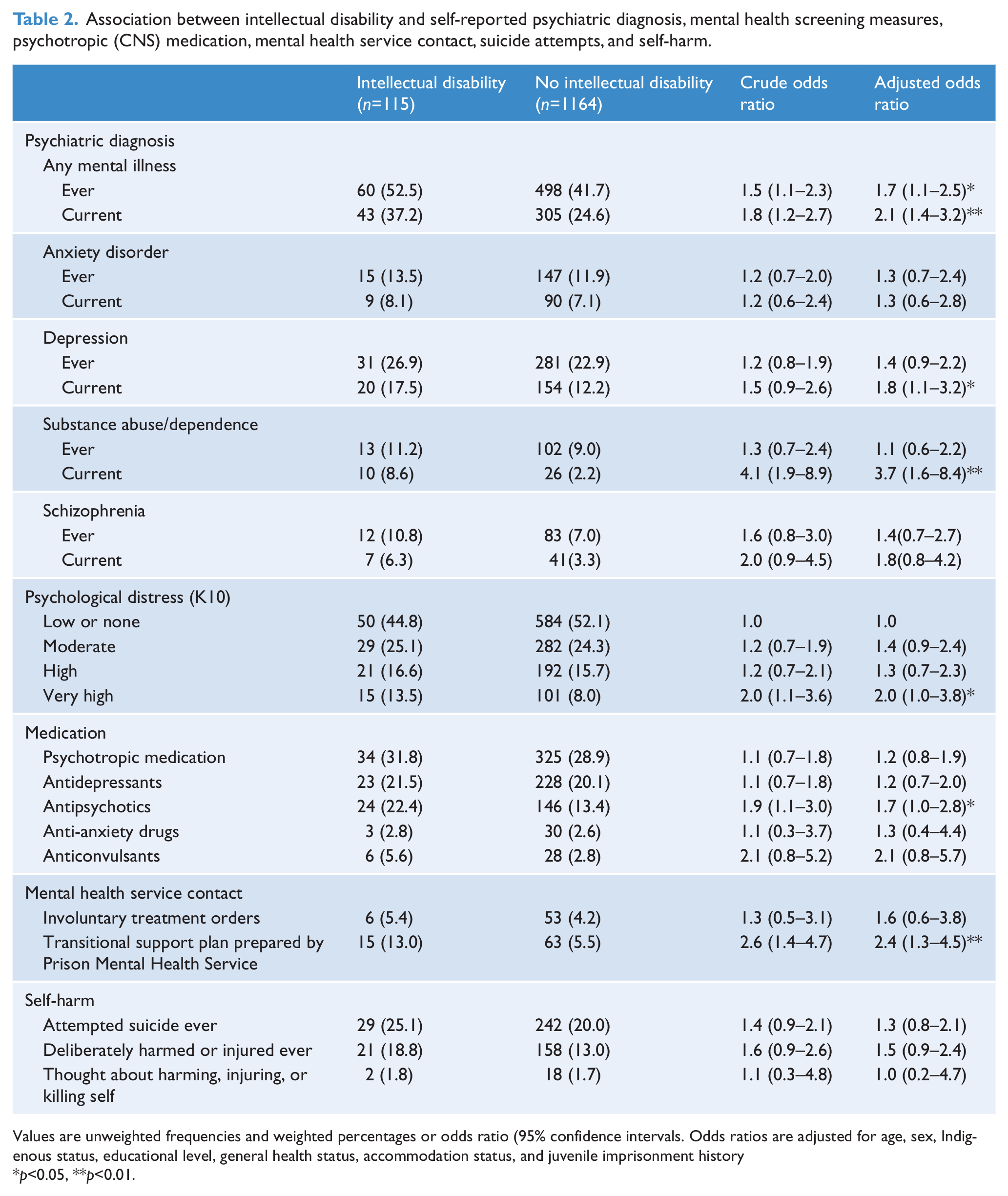
Values are unweighted frequencies and weighted percentages or odds ratio (95% confidence intervals. Odds ratios are adjusted for age, sex, Indigenous status, educational level, general health status, accommodation status, and juvenile imprisonment history
p<0.05, **p<0.01.
The prevalence of current mental disorder was 37.2% (95% CI 28.8–46.5%) in prisoners with intellectual disability and 24.6% (95% CI 22.2–27.2%) in prisoners without intellectual disability, a statistically significant association (AOR 2.1, 95% CI 1.4–3.2). The association between intellectual disability and mental disorder was stronger for current psychiatric disorders than for lifetime psychiatric diagnoses. For example, prisoners with intellectual disability were significantly more likely than their non-disabled counterparts to report a current diagnosis of depression (AOR 1.8, 95% CI 1.1–3.2) vs. a lifetime diagnosis of depression (AOR 1.4, 95% CI 0.9–2.2) or a current diagnosis of substance dependence (AOR 3.7, 95% CI 1.6–8.4) vs. a lifetime diagnosis of substance dependence (AOR 1.1, 95% CI 0.6–2.2).
We found a significant association between intellectual disability and psychological distress (AOR 2.0, 95% CI 1.0–3.8). Prisoners with intellectual disability (13.5%, 95% CI 8.3–21.1%) were more likely than those without intellectual disability (8.0%, 95% CI 6.6–9.7%) to report very high psychological distress according to the K10 (Table 2). Prisoners with intellectual disability had a mean MCS score of 44.7±11.9 compared with 45.1±13.3 in their non-disabled peers, a non-significant difference after adjusting for potentially confounding variables (adjusted mean difference –1.2, 95% CI –3.6 to 1.2).
Prisoners with intellectual disability were significantly more likely than their non-disabled peers to use antipsychotic medication (AOR 1.7, 95% CI 1.0–2.8; Table 2). Similarly, prisoners with intellectual disability were more likely than their non-disabled peers to report having received a transitional support plan prepared by the prison mental health service (AOR 2.4, 95% CI 1.3–4.5), although the vast majority of those with intellectual disability (87%) did not report receiving such a transitional support plan.
Discussion
Almost one in ten adult prisoners in this study screened positive for intellectual disability and more than half of prisoners with intellectual disability had a lifetime mental disorder. Prisoners with intellectual disability reported more severe social disadvantage, higher levels of psychological distress, a greater burden of mental illness, and greater use of psychotropic medication, compared with their non-disabled peers. This association remained even after adjusting for potentially confounding variables, including self-reported general health status.
These findings are generally consistent with those of previous studies. The positive association between intellectual disability and lifetime psychiatric diagnosis is consistent with previous studies that report elevated rates of mental illness among both offenders and non-offending populations with intellectual disability (Lund, 1985; Iverson and Fox, 1989; Reiss, 1990; Reid, 1994; Cooper, 1997; Hobson and Rose, 2008). However, in contrast to Hassiotis et al. (2011), we did not find that self-evaluated health status mediated the association between intellectual disability and mental illness. After adjusting for confounding variables including self-rated health, the strength of the association between intellectual disability and many of the indicators of poor mental health increased.
Previous research regarding prisoners with intellectual disability has largely focused on offending behaviour and criminal profiles. Studies considering intellectual disability and comorbid mental health needs have been limited by small cohorts from different contact points within the criminal justice system (e.g. courts) or large sample data of low reliability. The present study addressed these concerns by investigating the association between presence of intellectual disability and mental health in a large, representative cohort of mainstream adult prisoners and used an innovative combination of subjective and objective measures of mental illness to assess the association between intellectual disability and mental illness.
Full-scale psychometric testing of intelligence and adaptive behaviour is a prerequisite for a diagnosis of intellectual disability, but this was beyond the scope of the current study. In the absence of “gold standard” assessment criteria, we relied on a screening tool used widely in criminal justice settings. Using a pragmatic composite measure to compensate for the HASI’s over-inclusiveness, we estimated that 9.0% of the mainstream prison population had an intellectual disability, similar to an estimate of 10.8% obtained from a methodologically rigorous Norwegian study (Søndenaa et al., 2008).
Although designed to increase specificity over the HASI alone, our composite measure is also likely to capture prisoners with mild and borderline intellectual disabilities and other forms of intellectual impairment associated with mental illness and substance dependence. Cognitive impairment related to acquired brain injuries, which are common in this population (Schofield et al., 2006), coupled with low rates of literacy and poor educational attainment among prisoners, further complicate the detection of intellectual disability in this population. Diagnosis of intellectual disability is also dependent on assessment of adaptive behaviours, which was beyond the scope of our study. However, irrespective of diagnoses, our study highlights an extremely vulnerable group of prisoners who have complex and unmet dual psychiatric needs. Referral of such individuals for further psychometric and/or diagnostic assessment is strongly recommended in future research. Limitations of the study include reliance on self-reported information for diagnosed mental disorders, leading to possible recall bias. Detection of mental illness in people with intellectual disability is particularly challenging. This challenge arises partly because of problems with communication, which often makes it challenging for the individuals to access, recall, and express mental symptoms, and partly as a result of diagnostic overshadowing of mental illness by intellectual disability, leading to a possible underestimate of mental health disorders (Reiss, 1990; Prosser et al., 1998). However interviewers were trained by researchers with extensive experience in communicating with people with intellectual disability.
Consistent with previous studies (Leonard et al., 2003), the current study found that Indigenous prisoners were over-represented in the intellectual disability group. In addition to the uncertain cultural appropriateness of the HASI, the over-representation of Indigenous prisoners among the intellectual disability group may reflect cognitive impairments associated with the high rates of acquired brain injury in Indigenous prisoners, flowing from trauma, substance abuse, and cognitive decline associated with foetal alcohol syndrome disorders (Fortune and Wen, 1999; Simpson and Sotiri, 2006; NIDAC, 2009). Further research is required to establish the cultural appropriateness of the HASI.
Recently, there has been significant interest in the identification, assessment, and diagnosis of psychiatric disorders in people with intellectual disability (Einfeld et al., 2006; Cooper et al., 2007). Early detection of intellectual disability and routine screening and mental health needs assessments for prisoners with intellectual disability is strongly recommended at different contact points within the criminal justice system. Once detected, the non-custodial alternatives and diversion schemes to community-based specialist mental health ID services, where they exist, or generic psychiatric services, as well as social care needs could be addressed (Magistrates Court of Western Australia, 2012).
Prisoners with intellectual disability and comorbid psychiatric disorder are a vulnerable subgroup of prisoners who often have unmet mental health needs. Given the well-documented links between poor mental health and offending behaviour among people with intellectual disability (Glaser and Florio, 2004), improving mental health outcomes for prisoners with intellectual disability is important from both a criminal justice and a public health perspective. The development of models and targeted transitional interventions could benefit the individual, their family, and the whole community and reduce the financial cost to society. Rigorous evaluation of such interventions and models may provide evidence to support their wider adoption. Furthermore, an enhanced understanding of mental health characteristics prior to release can direct treatment and support pathways out of the criminal justice system and inform transitional planning of mental health services and policies for this profoundly disadvantaged group.
Footnotes
Funding
This work was supported by the National Health and Medical Research Council (NHMRC) (strategic award 409966, and career development award 1004765 to SAK).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.