
Abstract
Prisoner populations are characterized by individuals from disadvantaged backgrounds. This includes those with poor educational attainment, the unemployed, people who are socially isolated, people with multiple physical health problems, and the itinerant [1]. Additionally, in Australia indigenous people are over-represented in the prisoner population [2].
Mental disorder has consistently been associated with prisoner populations [3–7]. A recent review of over 60 prison mental health surveys found that inmates were more likely than the general population to have a psychotic illness, major depression, and a personality disorder [3]. Explanations for this include the deinstitutionalization of the mentally ill, a lack of adequate diversionary options for mentally ill offenders, and inadequate general psychiatric and specialist forensic services in the community [8].
Several Australian studies have examined the prevalence of mental illness among prisoners; however, most have relied on small samples and were conducted at single sites, thus limiting their generalisability [7],[9],[10]. All found a high prevalence of mental disorder.
We report the 12-month ICD-10 prevalence estimates of mental illness in two NSW correctional populations, recent admissions to the correctional system, and sentenced prisoners.
Method
Reception prisoners were those who had been either remanded into custody pending a court appearance or sentenced to a period of incarceration. Sentenced prisoners were those inmates who were already serving a prison sentence at the time of the study.
The reception sample consisted of prisoners who were screened within 24 h of admission into the correctional system over a 4 month period. Male reception prisoners were screened primarily at the state's main reception centre in the Sydney metropolitan area and at three, smaller, rural sites. Females were screened at the main reception centre for women in western Sydney. The reception sample was screened consecutively whenever possible. However, due to procedural difficulties, this was not always possible and the reception sample therefore represents a consecutive convenience sample.
Reception prisoners were screened by mental health nurses recruited from within the correctional health system; the sentenced sample was assessed by both forensic psychology masters' students and Justice Health nurses. All interviewers received training and support from senior mental health staff (Cain, Owens, Muller) working on the project. Interviewers worked systematically through a list of prison receptions provided by correctional staff for the previous day. Prisoners were retrieved by custodial officers and escorted to the interview rooms located in the reception area. Those agreeing to participate were interviewed in a private office within in the reception area. On average the interviews lasted 1.9 h (range 45 mins to 6 h).
The sentenced sample consisted of inmates recruited into the 2001 NSW Inmate Health Survey [1]. This survey examined the physical and mental health status of the prisoner population using a random sample of inmates. The sample size was calculated to ensure that prevalence estimates could be generated for a range of health conditions of interest. A minimum sample size of 241 was found to be sufficient to give an adequately precise prevalence for low prevalence conditions. A total of 914 inmates (approximately 10% of all men and 34% of all women in full-time custody) were invited to participate in the study.
The sample was stratified by sex, age, and Aboriginality and is described elsewhere [1]. Participants were approached several weeks after the health survey was conducted and invited to undertake further mental health screening. The overall response rate to the 2001 Inmate Health Survey was 85%.
Both reception and sentenced prisoners were assessed using the same instrument developed for the Australian National Survey of Mental Health and Wellbeing (NSMHWB) [11]. This instrument is essentially a modified version of the CIDI-A and is delivered via a laptop computer. The interviewers administered the questions and input the information onto the computer. The questionnaire yields both DSM-IV and ICD-10 diagnoses.
Psychosis was diagnosed using a short screener incorporated into the program. For the purpose of this study, ‘Any mental illness’ is defined as follows: psychotic symptoms in the past 12 months, any ICD-10 affective or anxiety disorder in the previous 12 months.
Data from the CIDI were imported into SPSS Version 11 [12] and scored using a program developed by staff at the Clinical Research Unit for Affective Disorders, Sydney. Summary statistics were calculated using SPSS 11. Odds ratios were used to compare reception and sentenced prisoners.
Results
Nine hundred and fifty-three (953) reception inmates (777 men and 176 women) were screened between March and June 2001. This represents over 30% of all male reception prisoners and 56% of all female receptions during the study period. Five hundred and seventy-nine (579) sentenced inmates (63% of the original Inmate Health Survey sample) who had participated in the Inmate Health Survey were screened between July and December 2001.
The sample
Representativeness was examined by comparing the characteristics of male and female participants and non-participants in both the reception and sentenced group and, for the sentenced group only, comparisons with the general prisoner population were available from the 2001 NSW Inmate Census [13].
Reception prisoners who participated in the survey were similar to non-participants with regards to age (male = 29.6 years vs. 29.8 years, p = 0.57; female = 29.1 years vs. 29.5 years, p = 0.7), and detoxification referrals (male = 40% vs. 43%, p = 0.19; female = 43% vs. 38%, p = 0.44).
Differences were observed between participants and non-participants in the reception group within the sexes. Male reception participants differed from non-participants in terms of the proportion of indigenous prisoners (12% vs. 15%, p = 0.02), and the proportion referred for crisis intervention (13% vs. 17%, p = 0.014). Among female reception participants, there were no significant differences in the proportion of indigenous prisoners screened (29% vs. 22% not screened, p = 0.21), referrals for crisis intervention (17% vs. 22% of non-participants, p = 0.36), and detoxification referrals (43% vs. 38%, p = 0.44).
For the sentenced group, participants and non-participants were similar in terms of age (male = 33.8 years vs. 32.2 years, p = 0.07; female = 32.7 years vs. 33.9 years, p = 0.42), the proportion of indigenous inmates (male = 30% vs. 30%, p = 0.94; female = 16% vs. 19%, p = 0.83), incarceration for violent offences (male = 53% vs. 48%, p = 0.36; female = 36% vs. 30%, p = 0.81), and a self-reported history of receiving psychiatric treatment (male = 41% vs. 40%, p = 0.69; female = 53% vs. 54%, p = 0.96). However, as might be expected given the lag between the Inmate Health Survey and the mental health assessment, participants had slightly longer median sentences than non-participants (male = 2.2 years vs. 1.5 years, p = 0.001; female = 1.5 years vs. 0.91 years, p = 0.18).
For the sentenced group, the census provided a further means of assessing the representativeness of the sample with regards to both demographic and crimographic characteristics. The median age of the men in the sentenced sample was 31 years vs. 30 years for the NSW prisoner population and, for females, 32 years vs. 29 years. The survey sample contained a higher proportion of indigenous males than the census population (30% vs. 15%) but a lower proportion of indigenous females (16% vs. 25%). The offence profile in the sentenced sample was similar to the census population for men and women as was the proportion of prisoners held in maximum, medium and minimum security.
Any mental illness
Overall, reception prisoners suffer from mental illness to a greater extent than sentenced prisoners (46% vs. 38%, OR = 1.4, 95% CI = 1.1–1.7) (Tables 1,2). Women also have higher levels of psychiatric morbidity than men (61% vs. 39%, OR = 2.5, 95% CI = 1.9–3.2) (Table 1).
Twelve month ICD-10 diagnoses of major mental disorders for reception and sentenced prisoners in NSW
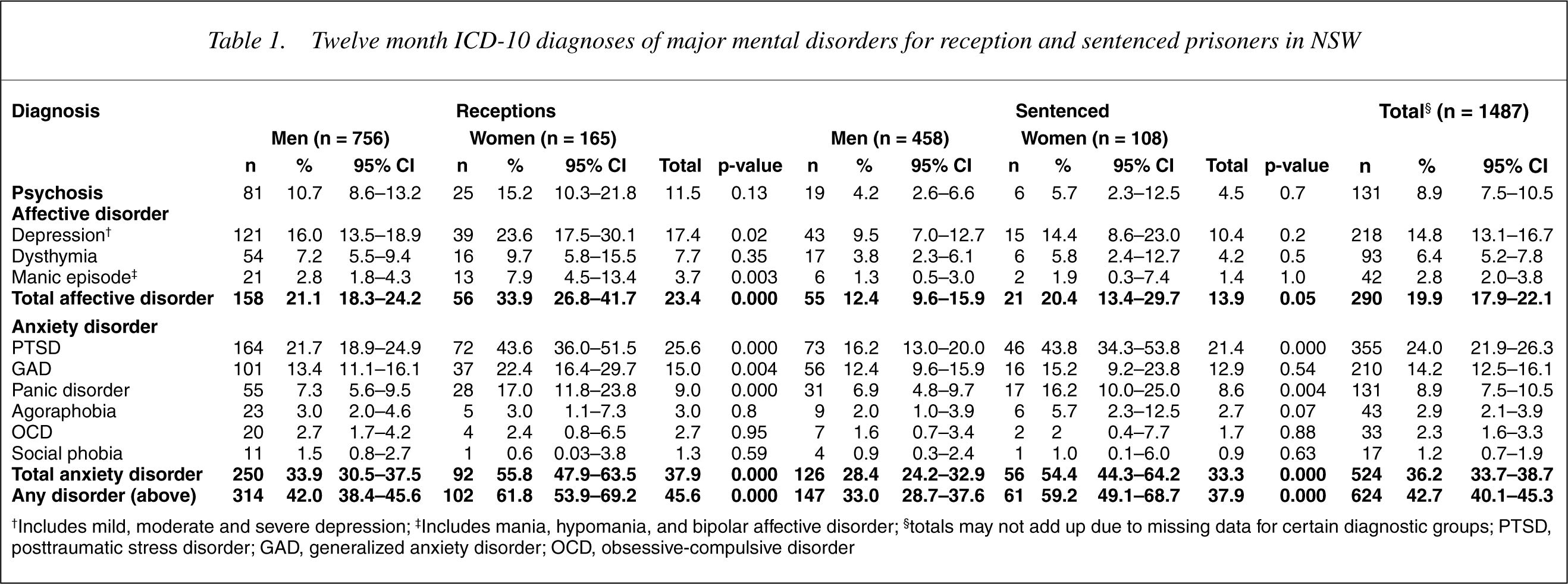
†Includes mild, moderate and severe depression; ‡Includes mania, hypomania, and bipolar affective disorder; §totals may not add up due to missing data for certain diagnostic groups; PTSD, posttraumatic stress disorder; GAD, generalized anxiety disorder; OCD, obsessive-compulsive disorder
Odds ratios for reception versus sentenced prisoners and women versus men
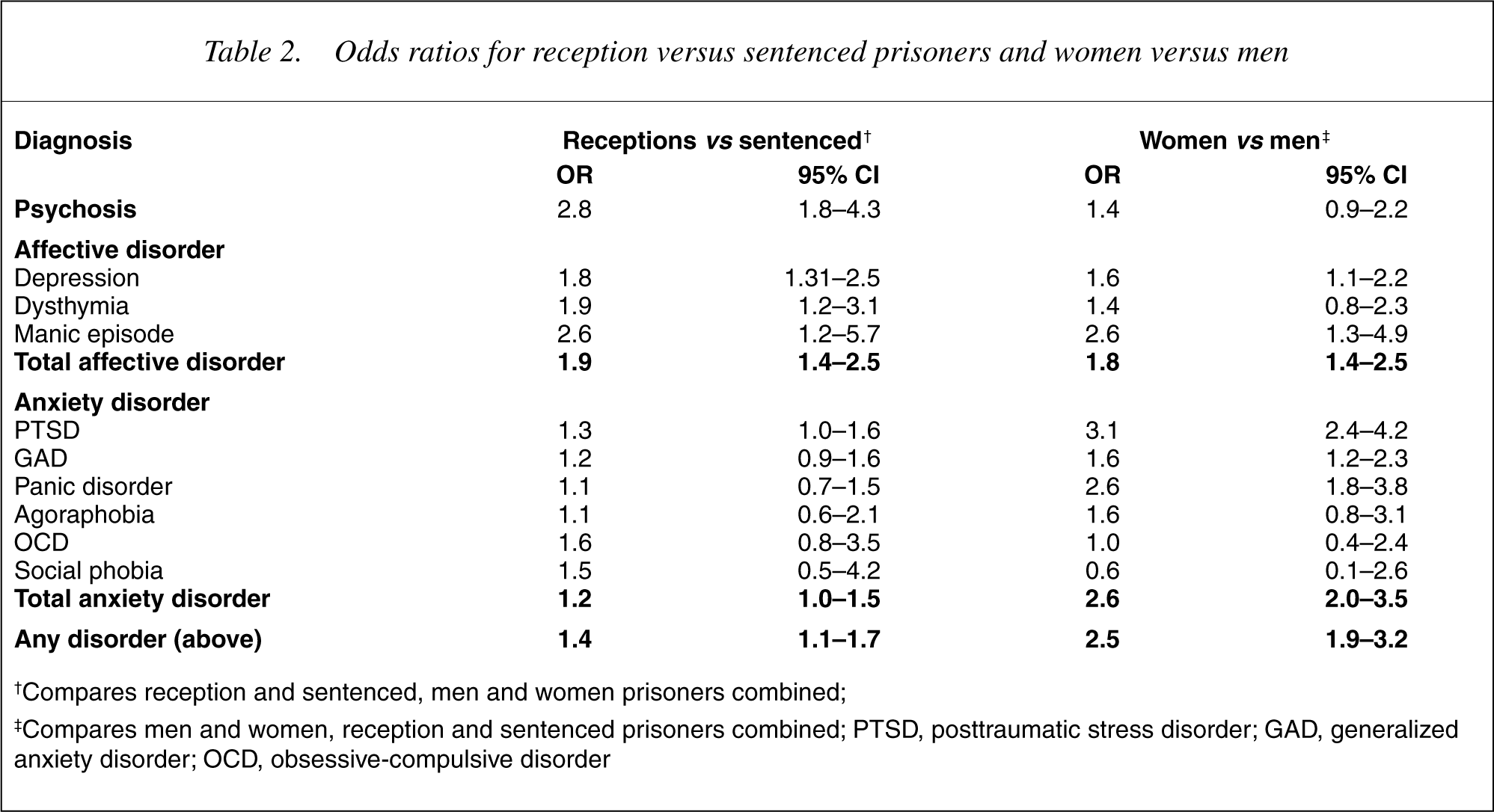
†Compares reception and sentenced, men and women prisoners combined;
‡Compares men and women, reception and sentenced prisoners combined; PTSD, posttraumatic stress disorder; GAD, generalized anxiety disorder; OCD, obsessive-compulsive disorder
Psychosis
Nine percent (9%) of all prisoners had experienced psychotic symptoms (due to any cause) in the prior 12 months. Psychosis was more common among reception than sentenced prisoners (12% vs. 5%, OR = 2.8, 95% CI = 1.8–4.3) (Table 1). Psychosis was lowest (4%) in men over 40 years old (Table 3).
Prevalence of mental disorder by sex and age group†
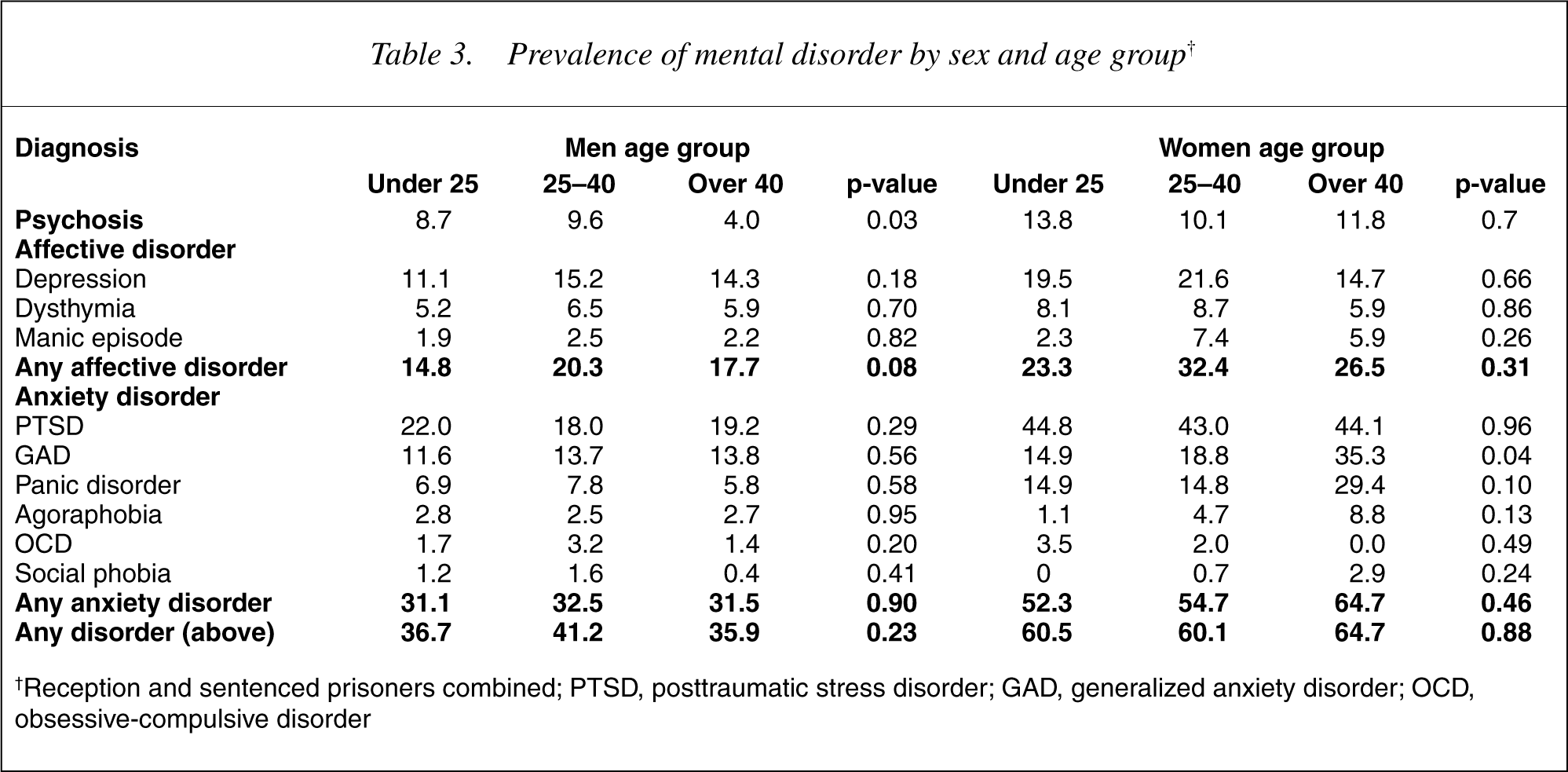
†Reception and sentenced prisoners combined; PTSD, posttraumatic stress disorder; GAD, generalized anxiety disorder; OCD, obsessive-compulsive disorder
Affective disorder
Twenty percent (20%) of all prisoners had suffered from at least one type of mood disorder in the prior 12 months (Table 1). Affective disorder was more common among receptions than sentenced prisoners (23% vs. 14%, OR = 1.9, 95% CI = 1.4–2.5). Mania was the least common mood disorder; only 4% of receptions and 1% of those sentenced had experienced at least one manic episode in the previous 12 months. Females were more likely than males to suffer from depression (20% vs. 14%, OR = 1.6, 95% CI = 1.1–2.2) and manic episodes (6% vs. 2%, OR = 2.6, 95% CI = 1.3–4.9).
Anxiety disorder
Thirty-six percent (36%) of all prisoners screened had experienced an anxiety disorder in the 12 months prior to interview. The prevalence of anxiety disorder was similar in the reception and sentenced groups (38% vs. 33%, OR = 1.2, 95% CI = 1.0–1.5) and substantially higher among women than men (55% vs. 32%, OR = 2.6, 95% CI = 2.0–3.5).
Overall, post traumatic stress disorder (PTSD) was the most common disorder, diagnosed in 26% of receptions and 21% of sentenced prisoners. Panic disorder, agoraphobia, obsessive-compulsive disorder, and social phobia were relatively rare in both the reception and sentenced groups. Social phobia was the only condition which was less prevalent among women than men.
Women were more likely than men to suffer from PTSD (44% vs. 20%, OR = 3.1, 95% CI = 2.4–4.2), panic disorder (17% vs. 7%, OR = 2.6, 95% CI = 1.8–3.8) and generalized anxiety disorder (20% vs. 13%, OR = 1.6, 95% CI = 1.2–2.3) (Tables 1,2). Generalized anxiety disorder increased with age and was highest in women over 40 years (Table 3). Among females, the prevalence of anxiety disorder did not differ markedly between the reception and sentenced prisoners (56% vs. 54%, p = 0.9).
Discussion
This is the first large-scale prevalence survey of mental illness conducted among Australian prisoners. Overall, 43% of those screened met the diagnostic criteria for at least one mental illness. Prisoners recently received into custody were more likely to be diagnosed with a mental illness than those who had been detained for some time and women were more likely than men to suffer from a mental illness.
These findings confirm that prisoners are a highly mentally disordered group compared with the general community [14]. The NSMHWB found the 12-month prevalence of any mental illness in the community was 15%, compared with 42% among inmates; psychosis was 0.4% in the community and 9% among inmates; affective disorder was 6% in the community and 22% among inmates; and anxiety disorder was 10% in the community and 43% among inmates [11].
The psychosis screener used in this study identified psychotic symptoms in 9% of prisoners. In comparison, a recent meta-analysis found that 3.7% of male prisoners and 4% of female prisoners had a psychosis due to mental illness [3]. This difference is likely due to the screener's inability to distinguish between psychosis due to mental illness and psychosis from other causes (e.g. substances), and a tendency towards false positives rather than false negatives.
The same meta-analysis found a higher prevalence of major depressive disorder in studies examining sentenced prisoners compared with detainees. This survey found that depression was significantly higher among those recently received into custody compared with sentenced prisoners. This could be explained by differences in the period of incarceration at the time of interview and the diagnostic criteria used for depression.
Posttraumatic stress disorder was the most prevalent condition, with one-fifth of all prisoners meeting the criteria for a 12-month diagnosis. Ironically, the wider community perceives prisoners as traumatisers but, as we found, they are also a highly traumatized group.
There are a number of explanations for the high number of mentally ill people in prison including: homelessness, a lack of adequate diversionary options in the community, inadequate specialist community forensic psychiatric services, deinstitutionalization of the mentally ill, the high threshold for admission to general psychiatric facilities, the reluctance of general psychiatric services to accept mentally ill patients from the courts, and society's intolerance of deviant behaviour by the mentally ill [15].
The reasons for a higher prevalence of mental illness at the point of reception are complex and reflect the poor psychosocial circumstances of offenders as a group. While prison is an unsatisfactory environment in which to treat those suffering a mental illness, the relatively lower prevalence of mental illness in the sentenced group suggests that imprisonment may be an important treatment opportunity for the mentally ill. We do not, however, advocate imprisonment as a therapeutic option.
These findings confirm the high prevalence of psychiatric disturbance among women prisoners. Women are generally less likely to offend than men and these findings suggest that when they do, they are more likely to be suffering from a mental illness.
An examination of participants and non-participants did not identify any major differences between the two groups. However, in the sentenced sample, men with longer sentences were more likely to have been screened. In the reception sample, there was a slight under-representation of indigenous men and those who had been referred to the mental health team for further assessment. The exclusion of those who were too mentally unwell to be screened is likely to have underestimated the prevalence of mental illness.
As part of the quality assurance, we reviewed 139 out of a possible 254 medical records of men at the main reception site in Sydney who had been referred for crisis intervention and could not participate in the project. This file review identified that 55% were on psychotropic medication, 70% had been identified as having a mental health disorder (excluding personality or substance use disorder), and 27% had a diagnosis of schizophrenia.
Most other studies of prisoner populations have examined either remanded prisoners or sentenced prisoners. It was an objective of our study to examine the burden of mental illness placed on the health services at the time of entry into prison. Collecting medical information at the point of entry into the correctional system is a reflection of the mental health status of the incarcerated offenders at the time of their arrest in the community. This is a critical and important point in the prisoners' course through the correctional system and an opportunity to intervene and initiate treatment.
Our intention was to screen a consecutive sample of prisoners. However, due to the inherent difficulties involved in prison-based research, this was not feasible. Obstacles to screening a consecutive sample in this setting include: variations of between zero and 50 reception prisoners on any one day resulting in a lack of interview staff to screen potential participants, rapid transfer of prisoners to other gaols before they could be interviewed, no custodial staff to retrieve inmates from the cells, prisoners released to freedom, unpredictable industrial action by correctional officers, and ‘lock downs’ (periods of time when inmates are locked in their cells and access is limited to emergency needs only). For the sentenced group, release to freedom and internal transfers to other prisons were the main reason for loss to follow-up.
Several drawbacks were inherent in using the NSMHWB screening tool which was preprogrammed. Certain demographic data could not be collected, the substance use module did not include cocaine use disorder, and the psychosis screener did not distinguish between the different psychotic disorders. However, these minor drawbacks need to be tempered against our ability to directly compare the prisoner sample with the community.
The mentally ill often revolve through prisons, with periods of incarceration interspersed with spells in the community, and place high demand on services [16]. Despite these factors, prisons provide an opportunity for intervention and treatment and, in some cases, may be a rare opportunity for certain individuals to receive treatment [17]. Given the high prevalence detected in this study, it is essential that prison mental health services be adequately resourced to cope with this demand and, at minimum, ensure that mental health does not deteriorate during incarceration.
Institutionalized populations including prisoners are excluded from community surveys such as the NSMHWB and the Australian National Health Survey. Given the extraordinarily high prevalence of mental illness detected, it is crucial that separate surveys such as this one be replicated in prisons so that marginalized populations are not overlooked. To this end, a national prisoner mental health survey is recommended.
These findings present a cogent argument for screening systems and diagnostic instruments to detect inmates with a mental illness at the point of reception. Once identified, there will likely be an increased demand for multidisciplinary mental health services to manage mental disorders and to co-ordinate linkage with community mental health services on release to freedom. Internationally and nationally, strategies have been adopted to address the disproportionately high number of offenders with a mental illness [18]. These include: diverting mentally ill offenders who have committed minor offences away from the criminal justice system, admission to secure forensic mental health facilities of those requiring involuntary psychiatric treatment and those found ‘not guilty by reason of mental illness’ or ‘unfit to stand trial’, and community support for ‘high risk’ and ‘forensic’ psychiatric patients.
Resources for the management of mentally disordered offenders in NSW have traditionally flowed into the correctional environment rather than the community. As a consequence, NSW has a relatively sophisticated correctional mental health service. However, forensic mental health services do not meet internationally accepted standards. Most forensic patients are hospitalized within the correctional system and forensic patients in the community are managed by general forensic psychiatric services. Recently there has been a commitment to reforming forensic services as evidenced by an expansion of the court liaison service, plans to build a high security forensic hospital outside of the correctional system, the establishment of a state-wide Directorate of Forensic Psychiatry, and resources made available to develop community forensic psychiatric services.
The high prevalence of mental illness in the prison community supports the argument for psychiatric and psychological treatments that target specific disorders. Biological treatments have been the dominant approach. However, this is not consistent with a multidisciplinary model. Greater attention should be given to treatment modalities such as cognitive behavioural, interpersonal and supportive psychotherapy. In addition there should be an emphasis placed on long-term drug and alcohol rehabilitation.
Footnotes
Acknowledgements
We wish to thank the Department of Corrective Services for assistance with operational aspects of conducting this project and the NSW Health Department (Centre for Mental Health) for financial assistance. Mr Glenn Wagner was responsible for coordinating the reception component of the survey.