
Abstract
Objective:
Pharmacological treatment is considered indispensable to major depressive disorder. In spite of this, a significant number of patients do not respond adequately to treatment based only on medication, presenting high relapse and recurrence rates. Therefore, psychosocial interventions, such as psychoeducation, have been increasingly recognized as an essential component in the treatment of depression, associated with pharmacological strategies. Thus, the aim of the present systematic review was to evaluate the effectiveness of psychoeducation for patients with unipolar depression, analyzing the evidence from the literature.
Method:
Searches were undertaken from April to October 2012 in LILACS, PsycINFO, PubMed, SCOPUS and ISI Web of Knowledge with keywords including ‘psychoeducation’, ‘psychoeducational intervention’ and ‘depression’, with no restriction regarding publishing dates.
Results:
Fifteen studies were included in the review, 13 of which evaluated the effectiveness of psychoeducation for patients with depression: 10 papers evaluated in-person psychoeducation approaches and three papers evaluated long-distance approaches. In addition to these 13 papers, one evaluated psychoeducational interventions for patients’ families and patients’ responses and another evaluated psychoeducational interventions for patients’ families and families’ responses. Findings suggest that increased knowledge about depression and its treatment is associated with better prognosis in depression, as well as with the reduction of the psychosocial burden for the family.
Conclusions:
Psychoeducation is a psychosocial treatment that has been well documented as an adjunct to pharmacological therapy. However, there are only a few studies regarding its effectiveness on adult patients with major depressive disorder. Although the publications in this area are still very limited, the articles selected in this review suggest that psychoeducation is effective in improving the clinical course, treatment adherence, and psychosocial functioning of depressive patients.
Introduction
Major depressive disorder (MDD) is a chronic, long-term disease with a high recurrence rate (Fleck et al., 2009; Kanai et al., 2003; Ramana et al., 1995). Major depression is identified by specific symptoms lasting for a few weeks, which bring manifest damage and suffering to patients’ lives (American Psychiatric Association, 2002). It may affect people at any moment of their lives; however, it has a higher incidence in the middle-aged population (Lewinsohn, 1989). In addition, the disorder is two to three times more common in women than in men, with a prevalence of around 10–25% for women and 5–12% for men (Fleck et al., 2009; Kessler et al., 2005).
This disorder often leads to functional disability, causing significant social, work and family problems for the patient (Broadhead et al., 1990; Wells et al., 1989). According to the World Health Organization (1992), depression affects about 340 million people around the world, causing severe consequences, such as functional disability, and high morbidity and mortality rates. There is a high occurrence of divorce (Kessler et al., 1998) and financial problems among MDD patients (Judd et al., 1996). It also negatively impacts on the economy, as the disorder is associated with higher work absence and increased medical assistance costs (Katon, 2003). When depression is compared with major chronic medical conditions, only severe cardiac ischemic diseases present the same disability rate among the main chronic diseases (Wells et al., 1989): MDD inflicts more damage to health than angina, arthritis, asthma, and diabetes (Moussavi et al., 2007). It was considered the fourth main cause of disability during the 1990s in a global scale for comparison with other diseases (World Health Organization, 2001). Forecasts indicate that, in 2020, depression will be the second major cause of global losses among all ages and sexes (Fleck et al., 2009; Kessler et al., 2005; Murray and Lopez, 1997). The occurrence of suicide is also high among these patients: between 15% and 20% of depressive patients commit suicide (Goodwin and Jamison, 1990).
Last decade, findings revealed the high relevance of pharmacological treatment, mainly for moderate and severe conditions (Anderson et al., 2000; Fleck et al., 2009). However, from 30% to 50% of depressed patients do not totally recover with medication (Rozenthal et al., 2004). From patients who were submitted to treatment for a depressive event, around 80% will experience a second event: individuals with depression usually have four events during their lifetimes (Fleck et al., 2009; Kupfer, 1991). However, low adherence rates have been recorded among all antidepressant categories, as most patients do not follow the recommended treatment (Lin et al., 1995; Maddox et al., 1994). Also, the longer depression remains untreated (i.e. the longer the time between the onset of symptoms and the beginning of treatment), the worse the clinical course of the disorder will be in terms of the number of recurrences and Axis I comorbidities (Fleck et al., 2009). Discontinuing treatment not only increases the risk of recurrence, but also increases the risk of poor response to subsequent treatment (Kennedy et al., 2002; Thase and Sullivan, 1995). Therefore, depression is a disease for which treatment remains unsatisfactory.
In spite of the fact that MDD is highly associated with genetic factors, several studies also show that psychosocial factors are highly relevant predictive signs of poor response to treatment (Fleck et al., 2009). Unsuitable social support, difficulty with social adjustment, a low social and economic level, and chronic stress significantly concur with MDD triggering and permanence (Kendler et al., 2002, 2003). According to some authors, stress can trigger the first depression event in genetically vulnerable individuals, making them even more sensitive to stress. After experiencing the first depressive event, those individuals require less stress to trigger new events and become more vulnerable to recurrences when facing different stress factors (Post, 1992; Zavaschi et al., 2002).
Within this scenario, pharmacological treatment combined with psychosocial intervention becomes more frequent. Among these psychotherapeutic approaches, psychoeducation (PE) is an alternative which targets the development of overall knowledge about depression for patients as a tool to help them deal with their disease (Colom, 2011). Considering that inadequate treatment leads to low recovery rates and frequent relapses (Faravelli et al., 1986), and both are strongly correlated to family environment, PE can also be an effective tool to improve the patient’s family environment, therefore reducing relapses and hospitalizations of patients with major depression (Corrigan, 2003; Murray-Swank and Dixon, 2004).
Although several studies have proved the effectiveness of psychoeducational intervention to improve the clinical course, treatment adherence and the psychosocial functioning of patients, most of these were performed in patients with bipolar disorder or schizophrenia (Anderson et al., 1986; Batista et al., 2011; Clarkin, et al., 1998; Colom et al., 2003; Glick, et al., 1994; Honig et al., 1997; Juruena, 2001; Shimodera et al., 2000; Simoneau, et al., 1999). Moreover, even though there are abundant data available concerning the diagnosis and pharmacological treatment of depression (Chan, 1984; Clary et al., 1992; Juruena, 2001; Luderer and Böcker, 1993; Souery et al., 2007), there is not enough knowledge about the effectiveness of PE for depression. With regard to this, the aim of the present systematic review was to evaluate the effectiveness of PE for patients with unipolar depression, analyzing the evidence from the literature.
Methods
LILACS, PsycINFO, PubMed, SCOPUS and ISI Web of Knowledge were searched for articles published in English, with keywords including ‘psychoeducation’, ‘psychoeducational intervention’ and ‘depression’, with no restriction regarding publishing dates. These searches were performed from April to October 2012. The selected papers were refined through a systematic review of article abstracts evaluating the effectiveness of PE with unipolar depressive disorder. In addition to this, a further hand search was performed to retrieve the articles referred to by these papers. In order to be included in this review, the studies had to evaluate the effectiveness of PE for patients, the response of patients after PE for their families, or only the response of families to PE. With regard to studies that evaluated patients only, this review includes articles that assessed interventions performed in person (either through group or individual sessions) and from a distance (either online or by mail). For the other two groups of studies (those that evaluated patients and their families and those that evaluated patients’ families only), no further classification was applied. This review also includes studies where PE is associated with other types of psychotherapeutic interventions, as the initial search, including PE only, returned only a small number of papers. The exclusion criteria are detailed in Figure 1.
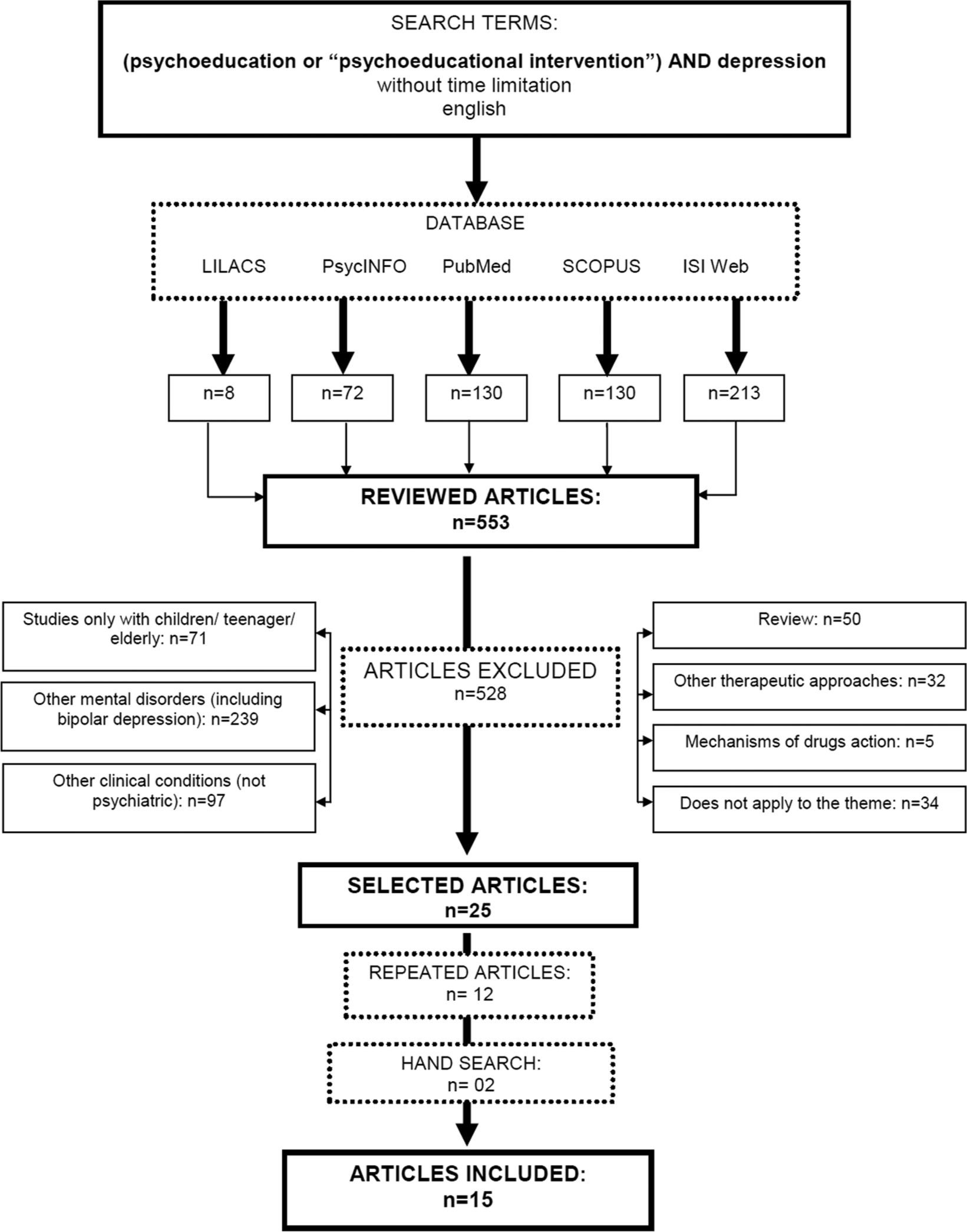
Methodology for article selection.
Results
Eight articles were identified in LILACS, 72 in PsycINFO, 130 in PubMed, 130 in SCOPUS and 213 in ISI Web of Science, amounting to 553 articles. After the application of the exclusion criteria, 25 articles were selected. From these, 12 were eliminated because they were duplicate articles among the databases. Two additional articles were selected through a hand search, amounting to 15 articles to be examined in this review.
General findings
From the 15 studies included in this review, 13 evaluated the effectiveness of PE for patients only. These 13 patient studies can be split into two groups: in person (10 studies) and long distance (three studies). Regarding the 10 studies with patients seen in person, seven applied PE for patients in groups (Brown and Lewinsohn, 1984; Butler et al., 2008; Dalgard, 2006; Dowrick et al., 2000; Lara et al., 2003; Steinmetz et al., 1983; Swan et al., 2003) and three applied PE for patients individually (Katon et al., 2001; Simon et al., 2002; Von Korff et al., 2003). The other three studies with patients applied PE from a distance, using either the Internet (Christensen et al., 2004; Meyer et al., 2009) or mail (Seedat et al., 2008). Finally, from the 15 selected papers, two assessed the patients’ families: one study performed PE for patients’ families, evaluating responses in patients (Shimazu et al., 2011); the other study performed PE for patients’ families, evaluating responses in families only (Katsuki et al., 2011).
The pioneering study on the efficacy of PE conducted by Steinmetz et al. (1983) examined the efficacy of a psychoeducational approach in treating unipolar depression using ‘Coping with Depression’ (CWD), a structured psychoeducational program. Another three authors also tested the effect of a modified CWD on unipolar depression in a randomized controlled trial (RCT) design in adults (Brown and Lewinsohn, 1984; Dalgard, 2006; Swan et al., 2003). More recently published studies performed psychoeducational intervention involving families (Katsuki et al., 2011; Shimazu et al., 2011). We identified a total of only nine RCTs that analyze the effectiveness of PE (Butler et al., 2008; Christensen et al., 2004; Dalgard, 2006; Dowrick et al., 2000; Katon et al., 2001; Meyer et al., 2009; Shimazu et al., 2011; Simon et al., 2002; Von Korff et al., 2003). Moreover, most of these RCTs evaluated the effectiveness of PE when associated with other therapeutic approaches (Butler et al., 2008; Christensen et al., 2004; Dalgard, 2006; Dowrick et al., 2000; Meyer et al., 2009). The study conducted by Christensen et al. (2004) and Meyer et al. (2009) was performed through the Internet. The gender composition of the samples varied in all of these studies; only Lara et al. (2003) conducted a study with a sample of women exclusively.
Ten papers reported having trained professionals to perform the technique of PE (Dalgard, 2006; Dowrick et al., 2000; Katon et al., 2001; Katsuki et al., 2011, Lara et al., 2003; Seedat et al., 2008; Shimazu et al., 2011; Simon et al., 2002; Swan et al., 2003; Von Korff et al., 2003) and only one study reported lay interviewers (Christensen et al., 2004). Most of the studies reported inclusion and exclusion criteria; however, not with consensus. The assessment of the effectiveness of PE for depression was also not uniform, but most studies used an internationally recognized interview. Among the studies, the most consistently employed measure was the Beck Depression Inventory (BDI), which was used in seven studies, followed by the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID I), which was used in four studies. The following instruments were also employed: Hamilton Rating Scale for Depression (HRSD), Symptom Check List (SCL), Cornell Dysthymia Rating Scale–Self Reported (CDRS-SR), and the Center for Epidemiologic Studies Depression Scale (CES-D), among others.
The study with the smallest sample, which was conducted by Katsuki et al. (2011), had 32 participants, including patients and controls, and performed PE for families. On the other hand, the biggest sample was from a study by Seedat et al. (2008), which assessed the possible benefits of a patient PE program using newsletters on a monthly basis and had 664 participants. Different study groups used varying numbers of sessions ranging from four to 12, lasting from 20 to 50 minutes, and performing follow-up during periods that ranged from 1 to 12 months. The main methods and results will be detailed in the following items.
Psychoeducation for patients
This section comprises the studies that evaluated the effectiveness of PE both in person and from a long distance. The studies performed in person applied individual and group interventions, as in Table 1. The ones performed from a long distance, by Internet or mail, are described in Table 2.
Main results of psychoeducational intervention with patients conducted in person.
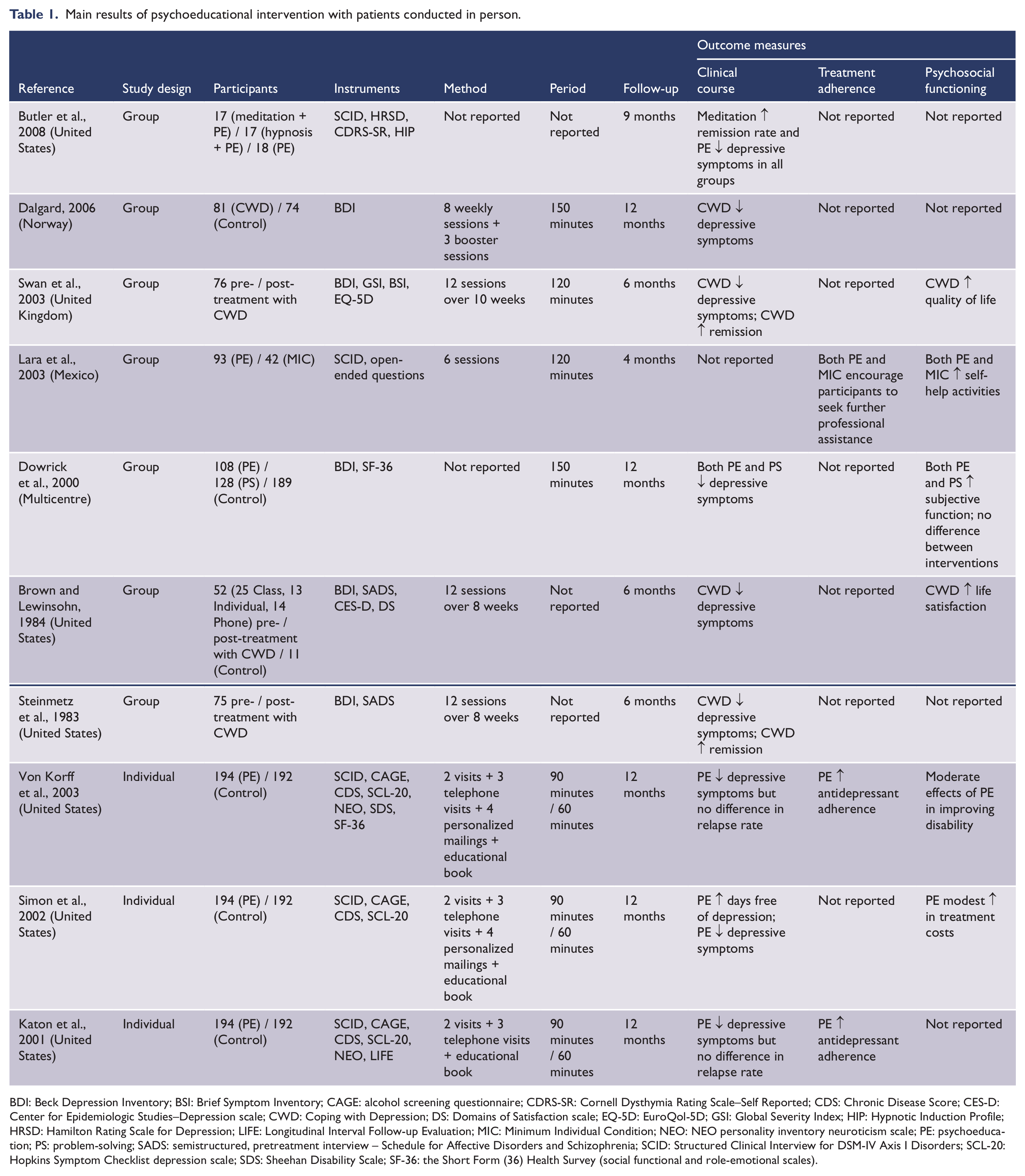
BDI: Beck Depression Inventory; BSI: Brief Symptom Inventory; CAGE: alcohol screening questionnaire; CDRS-SR: Cornell Dysthymia Rating Scale–Self Reported; CDS: Chronic Disease Score; CES-D: Center for Epidemiologic Studies–Depression scale; CWD: Coping with Depression; DS: Domains of Satisfaction scale; EQ-5D: EuroQol-5D; GSI: Global Severity Index; HIP: Hypnotic Induction Profile; HRSD: Hamilton Rating Scale for Depression; LIFE: Longitudinal Interval Follow-up Evaluation; MIC: Minimum Individual Condition; NEO: NEO personality inventory neuroticism scale; PE: psychoeducation; PS: problem-solving; SADS: semistructured, pretreatment interview – Schedule for Affective Disorders and Schizophrenia; SCID: Structured Clinical Interview for DSM-IV Axis I Disorders; SCL-20: Hopkins Symptom Checklist depression scale; SDS: Sheehan Disability Scale; SF-36: the Short Form (36) Health Survey (social functional and role-emotional scales).
Main results of psychoeducational intervention with patients at distance.
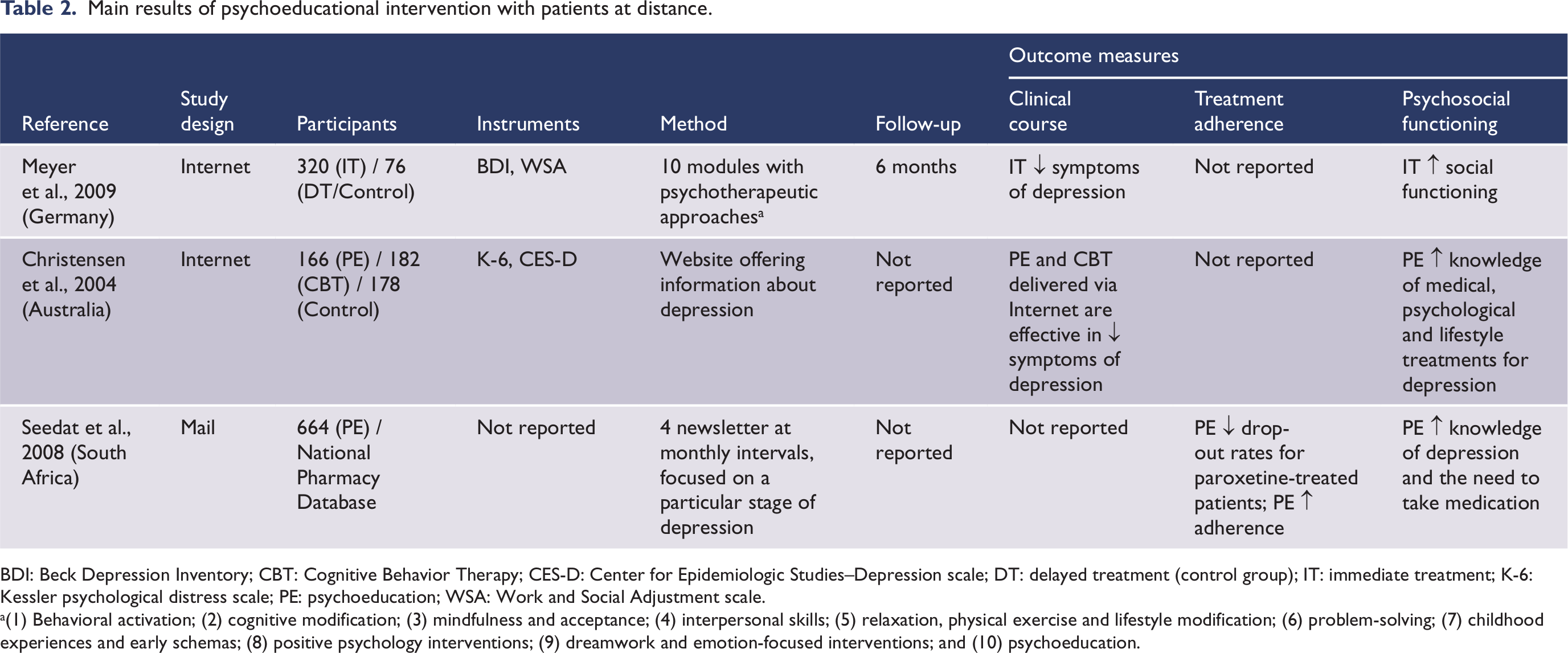
BDI: Beck Depression Inventory; CBT: Cognitive Behavior Therapy; CES-D: Center for Epidemiologic Studies–Depression scale; DT: delayed treatment (control group); IT: immediate treatment; K-6: Kessler psychological distress scale; PE: psychoeducation; WSA: Work and Social Adjustment scale.
(1) Behavioral activation; (2) cognitive modification; (3) mindfulness and acceptance; (4) interpersonal skills; (5) relaxation, physical exercise and lifestyle modification; (6) problem-solving; (7) childhood experiences and early schemas; (8) positive psychology interventions; (9) dreamwork and emotion-focused interventions; and (10) psychoeducation.
In-person approaches
Group sessions
The seven selected papers evaluated patients with depression according to standardized diagnostic interviews based on the Diagnostic and Statistical Manual of Mental Disorders (Butler et al., 2008; Dalgard, 2006; Dowrick et al., 2000; Lara et al., 2003), the International Classification of Diseases (Swan et al., 2003) or the Research Diagnostic Criteria (Brown and Lewinsohn, 1984; Steinmetz et al., 1983).
Four of the seven studies used the Coping with Depression (CWD) course, a psychoeducational group program developed by Lewinsohn, et al.; three papers compared patients in previous and post-treatment stages (Dalgard, 2006; Steinmetz et al., 1983; Swan et al., 2003) and one paper compared patients according to their assignment to one of these four conditions: class, individual tutoring, minimal contact or delayed treatment control (Brown and Lewinsohn, 1984). Two of the seven group-session papers investigated the effects of PE in comparison to other psychotherapeutic approaches (Butler et al., 2008; Dowrick et al., 2000). One study reported evaluation of a brief group intervention compared to a minimum individual condition group intervention in samples composed only by women (Lara et al., 2003), while the other six articles performed PE with both sexes.
We identified five RCTs (Brown and Lewinsohn, 1984; Butler et al., 2008; Dalgard, 2006; Dowrick et al., 2000; Lara et al., 2003). Those five study groups used different numbers of sessions, ranging from six to 12 (Brown and Lewinsohn, 1984; Dalgard, 2006; Lara et al., 2003; Steinmetz et al., 1983; Swan et al., 2003). The length of time of the group sessions ranged from 120 to 150 minutes (Dalgard, 2006; Dowrick et al., 2000; Lara et al., 2003; Swan et al., 2003); all studies performed follow-up during periods ranging from 1 to 12 months. The number of participants, either subjects or controls, ranged from the minimum of 52 (Butler et al., 2008) to the maximum of 425 (Dowrick et al., 2000). Among these five RCTs, only two studies reported the average number of participants per group: 8–10 in Dalgard’s paper (2006) and 5–19 in Lara et al. (2003). All studies reported the participation of patients older than 18 years; only the study from Lara et al. (2003) restricted the age from 20 to 45 years. Subjects with psychotic symptoms, a psychiatric diagnosis other than unipolar depression, suicidal ideation, or mental retardation; severe visual, hearing, or memory impairment; mania, hypomania, schizoaffective or schizophrenic disorder; and a current drug or alcohol disorder, suicidal risk, pregnancy, or organic damage, were excluded from the studies.
Steinmetz et al. (1983), Brown and Lewinsohn (1984), Swan et al. (2003) and Dalgard (2006) found a reduction of depressive symptoms, improved rates of remission and quality of life and effectiveness in the treatment of unipolar depression. Butler et al. (2008) evaluated the effects of meditation with yoga and PE versus group therapy with hypnosis and PE versus PE only on diagnostic status, and suggested that all groups had some reduction of symptom levels without a significant intensity difference. Dowrick et al. (2000) showed that problem-solving treatment was more acceptable than the course on prevention of depression. However, both interventions reduced caseness and improved subjective function. Lara et al. (2003) did not find a significant difference regarding symptom reduction, but found a significant increase in self-help activities and in the search for further professional assistance when necessary.
Individual sessions
Katon et al. (2001), Simon et al. (2002) and Von Korff et al. (2003) described a relapse prevention program for patients who had recovered from a depressive episode and remained at high risk for relapse. A total of 386 patients aged from 18 to 80 years old, with recurrent major depression or dysthymia, and at high risk of relapsing, received a new antidepressant prescription. After this, they were randomized to a relapse prevention program (n = 194) or usual primary care (n = 192). Alcohol-addicted patients, pregnant patients and patients recently using lithium or antipsychotic medication were excluded from the study. This program was a multifaceted intervention including an educational book and videotape; two in-person visits from a depression prevention specialist, three scheduled telephone monitoring contacts (2, 5, and 9 months after enrollment) including monitoring of depressive symptoms and treatment adherence; and four personalized mailings (3, 6, 10, and 12 months after enrollment) for continued monitoring of depressive symptoms and treatment adherence.
In spite of using the same sample, the objectives of the studies were different, as Katon et al. (2001) hypothesized that an intervention would improve adherence to antidepressants and improve depression outcomes in high-risk patients in comparison to usual primary care, Simon et al. (2002) evaluated the incremental cost-effectiveness of the program in primary care, and Von Korff et al. (2003) evaluated the effects of this program on depression assessing disability outcomes among patients treated for depression at high risk for relapse.
In the Katon study (2001), the intervention group had significantly greater adherence to adequate dosage of antidepressant medication for 90 days or more within the first and second 6-month periods and was significantly more likely to refill medication prescriptions during the 12-month follow-up in comparison to usual care controls. Intervention patients had significantly fewer depressive symptoms, but not fewer episodes of relapse/recurrence over the 12-month follow-up period. Simon et al. (2002) described the incremental cost and cost-effectiveness of an organized program to reduce the risk of depression relapse among primary care patients from the perspective of the health insurer. A program to prevent depression relapse in primary care brings modest increases in days free of depression and modest increases in treatment costs. These modest differences reflect high rates of treatment in usual care. Along with other recent studies, these findings suggest that improved care of depression in primary care is a prudent investment of health care resources. Usual care patients and relapse prevention program patients had high rates of use of maintenance pharmacotherapy. Von Korff et al. (2003) showed that both relapse prevention and usual care patients showed improved functioning over the 12-month follow-up period. Moderate effects of a relapse prevention intervention on depressive symptoms were associated with modest and variable effects on disability outcomes. Inconsistent effects of the intervention for disability outcomes may happen because of the high rates of maintenance pharmacotherapy among usual care patients, relatively average levels of depressive symptoms among both intervention and control patients at baseline, the absence of a specific relapse prevention effect of the intervention, and the resultant modest differences in depressive symptoms between intervention and control patients in this trial.
Long-distance approaches
From the three articles which performed long-distance intervention for patients, two evaluated the effectiveness of PE through the Internet (Christensen et al., 2004; Meyer et al., 2009) and the other by mail (Seedat et al., 2008) (Table 2). Christensen et al. (2004) evaluated the effectiveness of two Internet interventions for community-dwelling individuals with symptoms of depression: a PE website offering information about depression and an interactive website offering cognitive behavior therapy. A total of 525 individuals with increased depressive symptoms were recruited by survey and randomly allocated to a website offering information about depression (n = 165), or a cognitive behavior therapy website (n = 182), or a control intervention using an attention placebo (n = 178). Participants aged 18–52 years, scored 22 or above on the Kessler psychological distress scale and not receiving clinical care from either a psychologist or psychiatrist were selected. Lay interviewers contacted participants weekly by phone to direct their use of the websites. Participants were sent detailed guides outlining navigation and weekly assignments for BluePages (PE) or MoodGYM (cognitive behavior therapy). Both BluePages and MoodGYM participants were directed each week to one of the five sections of the website, submitted a weekly review and a final one at the end of the sixth week. In the control intervention, participants were contacted weekly by phone over the 6 weeks to answer questions about lifestyle and environmental factors that may have an influence on depression. Intention-to-treat analysis indicated that information about depression (PE) and interventions that used cognitive behavior therapy and were delivered via the Internet were more effective than a credible control intervention in reducing the symptoms of depression in a community sample. PE (BluePages) significantly improved participants’ understanding of effective treatments for depression. Both PE and cognitive behavior therapy delivered via the Internet are effective in reducing the symptoms of depression.
The model of Meyer et al. (2009) evaluated the effectiveness of Internet-based intervention in a RCT. There were 396 adults, above the age of 18 years, sourced from Internet depression forums and randomly assigned to either 9 weeks of immediate-program-access as an add-on to treatment-as-usual (n = 320), or to a 9-week delayed-access plus treatment-as-usual condition (n = 76); follow-up was at pre- and post-treatment and 6 months. The Internet-based intervention consisted of 10 content modules representing different psychotherapeutic approaches, each of which to be completed in 10–60 minutes. This integrative, Internet-based intervention was effective in reducing the symptoms of depression and in improving social functioning. Findings suggest that the program could serve as an adjunctive or stand-alone treatment tool for patients suffering from the symptoms of depression.
In their pilot study, Seedat et al. (2008) explored the possible benefits of a PE program for patients in order to increase medication adherence. Following the prescription of paroxetine for depression, patients were asked by their practitioners if they were willing to receive a newsletter about depression. Patients who agreed were sent four newsletters, each focusing on a particular stage of depression, at monthly intervals. Interviews with 664 adult patients on paroxetine (18–65 years of age), by telephone, attempted to determine whether they were still taking their medication (if not, when and why they had stopped?), whether they had received the newsletters sent out, and whether they had found the articles beneficial. At the time of interview, 448 of 664 patients (67.5%) were still taking their medication. Prescription collection was thus used in this survey as a proxy indicator of adherence. Adherence data for the control group were derived from a national pharmacy database. Patients who participated in a psychoeducational program demonstrated comparatively lower drop-out rates during treatment compared with drop-out rates in patients on paroxetine (and other selective serotonin re-uptake inhibitors (SSRIs)) obtained from a national pharmacy database. Improved adherence on the psychoeducational program was attributed to an increased understanding of depression and the need to take medication, a realization that patients are not alone and a better understanding and acceptance of the possible side effects of medication. Both practitioners and patients were positive about their experience of the program and 80% of doctors judged the program to be very useful. Drop-out rates during SSRI treatment appear to be unacceptably high, whether or not patients receive concomitant benzodiazepines. Psychoeducational programs may prove valuable in increasing adherence to treatment regimes.
Psychoeducation for patients’ families evaluating response in patients
In the only study found in this category, Shimazu et al. (2011) examined family PE in the maintenance treatment of depression and investigated the influence of the family’s expressed emotion (EE) on its effectiveness. In these findings, the authors compared the participation of 24 families in the intervention group and 30 in the control group. The participants were patients who satisfied defined eligibility criteria (age 18–85 years, with MDD, living with the family for 3 months or longer, not having undergone electroconvulsive therapy or having organic disease) and their primary family members. Family PE took the form of courses attended by up to five family members, without the participation of the patients. Sessions took place once every 2 weeks (the full course comprised four sessions), lasted 90–120 minutes, and used a videotape and textbook to explain depression. With regard to the clinical outcome measures, Shimazu et al. (2011) show that time to relapse was statistically significantly longer in the PE group than in the control group. Relapse occurred before completion of the 9-month follow-up assessment in two patients (8%) in the intervention group and 15 (50%) in the control group. Moreover, the remission rates at 9 months were 83% and 33%, respectively, showing a significant difference between the two groups. However, when evaluating the influence of baseline EE status on the effectiveness of the intervention, no association was found among intervention, EE and outcomes.
Psychoeducation and response assessment for patients’ families only
In Katsuki et al. (2011), 32 relatives of patients with MDD participated in a study testing the effectiveness of brief multifamily PE. The relatives of patients with MDD who had a current diagnosis of primary anxiety disorder, personality disorder, substance abuse or dependence were excluded. The intervention consisted of four sessions over the course of 6 weeks, lasting approximately 2 hours. Each of the four multifamily psychoeducational program groups consisted of the relatives of approximately six patients. They did not include patients with MDD in the family groups because the patients with MDD easily felt guilty. The teaching materials for the relatives of the patients were two videotapes. The outcome measures focused on the assessment of psychosocial functioning of patients’ families. The emotional distress, care burden and expressed emotion of the family all showed statistically significant improvements from baseline to after the family intervention. This study suggests that brief multifamily PE is a useful intervention to reduce the psychosocial burden of relatives from patients with depressive disorder. Further evaluation of family PE for relatives of patients with depressive disorder is warranted.
Discussion
The main objective of this review was to identify all the available studies that evaluated the effectiveness of PE in adult patients with depression by extensively searching the main databases. However, most of these studies were not well designed or well described with regard to the therapeutic approaches they employed, making it difficult to compare them. In the 15 papers selected, there was a diversity of methodologies, ranging from the heterogeneity of participants, methods and criteria of evaluation to the variety of interventions used to analyze the effectiveness of PE, which brought significant barriers to a straightforward and direct comparison among the studies; owing to this, no meta-analyses were attempted.
Concerning the differences of participants included in the studies, PE and response evaluation were sometimes performed only for patients (Brown and Lewinsohn, 1984; Butler et al., 2008; Christensen et al., 2004; Dalgard, 2006; Dowrick et al., 2000; Katon et al., 2001; Lara et al., 2003; Meyer et al., 2009; Seedat et al., 2008; Simon et al., 2002; Steinmetz et al., 1983; Swan et al., 2003; Von Korff et al., 2003), sometimes for patients and their families (Shimazu et al., 2011) and at other times just for the patients’ families (Katsuki et al., 2011). In recent years, family PE has been recognized as part of the optimal treatment for patients with depressive disorder. Although few studies have been published, it is noticeable that studies published more recently performed psychoeducational intervention involving families (Katsuki et al., 2011; Shimazu et al., 2011). However, an important limitation to the comparative analysis of these papers is the fact that one of them evaluated the effectiveness of PE for patients’ families assessing response in patients (Shimazu et al., 2011), while the other performed PE and evaluated response to the intervention only in patients’ families (Katsuki et al., 2011).
Regarding the 13 papers that performed PE for patients, comparison was even more difficult because the studies were designed using very different forms of intervention. They had to be categorized as interventions and evaluations performed either from a long distance for patients using the Internet (Christensen et al., 2004; Meyer et al., 2009) and mail (Seedat et al., 2008), or interventions and evaluations performed in person. Those studies in which interventions and assessment were carried out in person (10 papers), were subdivided according to the use of group sessions (Brown and Lewinsohn, 1984; Butler et al., 2008; Dalgard, 2006; Dowrick et al., 2000; Lara et al., 2003; Steinmetz et al., 1983; Swan et al., 2003) or individual sessions (Katon et al., 2001; Simon et al., 2002; Von Korff et al., 2003).
Also, some of these 13 patient-only studies tended to be less well structured, impairing relevant conclusions. For example, in the studies conducted from a long distance, the authors offered information about depression either via a website (Christensen et al., 2004; Meyer et al., 2009) or monthly newsletter (Seedat et al., 2008). It may be a bias not to know how the patient received the information, or what the quality of their learning was. Another point of divergence between the interventions was that they were sometimes performed in group sessions and at other times individually.
Summing up, the primary limitation to the comparison of the selected articles concerns the fact that there was no consensus as to the methodology, as it is quite diversified (sample sizes, the use of control groups, instruments applied, number and duration of sessions were all heterogeneous among the studies) and some papers do not even mention some of these elements (Brown and Lewinsohn, 1984; Butler et al., 2008; Dowrick et al., 2000; Steinmetz et al., 1983). In their study, Brown and Lewinsohn (1984) assessed PE in participants in four conditions: class, individual tutoring, minimal contact, or delayed treatment control. The results indicated clinical improvement in the whole active treatment group compared to the delayed treatment conditions. Alternatively, Lara et al. (2003) assessed women in a psychoeducational intervention comparing them with other women in a minimum individual condition. Furthermore, in interventions performed individually, Katon et al. (2001), Simon et al. (2002), and Von Korff et al. (2003) belong to the same research group and use the same intervention, methods and sample, demonstrating using a single study while assessing different aspects of the sample. Katon et al. (2001) evaluated a relapse prevention intervention for improving adherence to medication, Simon et al. (2002) evaluated the incremental cost-effectiveness of this same program, and Von Korff et al. (2003) evaluated the effects of this prevention program on disability outcomes among patients treated for depression at high risk.
Among the 15 studies, only nine were RCTs; it should be stressed that three of these nine papers are from the same group and evaluate the same sample (Katon et al., 2001; Simon et al., 2002; Von Korff et al., 2003). Thus, although RCT studies are supposed to show greater methodological rigor, the studies analyzed have flaws and limitations because some authors do not adequately describe the method, form of intervention, instruments, inclusion criteria, sample size, number and duration of sessions or follow-up.
In the RCTs, Dowrick et al. (2000), Christensen et al. (2004), Butler et al. (2008) and Shimazu et al. (2011) conducted psychoeducational intervention compared to other approaches, while Dalgard (2006) and Meyer et al. (2009) performed PE along with other therapeutic approaches. The studies conducted by Christensen et al. (2004) and Meyer et al. (2009) were performed by Internet, which may reduce the reliability of results. With regard to the therapeutic approach, in these studies there is a difficulty in analyzing whether the improvement is due to PE or other associated approaches (Brown and Lewinsohn, 1984; Darlgard, 2006; Meyer et al., 2009; Steinmetz et al., 1983; Swan et al., 2003).
Therefore, the fundamentals of each article have been comprehensively discussed and the main conclusion is the absence of a strict and rigorous methodology for studies that evaluate the effectiveness of PE for those patients, such as the methodology used in PE studies with bipolar disorder and schizophrenia (Batista et al., 2011; Shimodera et al., 2000). Despite the several limitations of the studies discussed in this review, relevant findings regarding the effectiveness of PE for patients with unipolar depression showed benefits. In spite of the large methodological variation, the effectiveness of PE for patients with unipolar depression seems a consensus among the articles (Brown and Lewinsohn, 1984; Christensen et al., 2004; Dalgard, 2006; Dowrick et al., 2000; Katon et al., 2001; Katsuki et al., 2011; Lara et al., 2003; Meyer et al., 2009; Seedat et al., 2008; Shimazu et al., 2011; Simon et al., 2002; Steinmetz et al., 1983; Swan et al., 2003; Von Korff et al., 2003). Only in the study by Butler et al. (2008), did the patients did not show any improvement.
The mechanism of action of PE remains unknown. We may hypothesize that teaching lifestyle regularity may play a role in the prevention of depression, whereas early detection of prodromal symptoms may be crucial for preventing relapses, which has been reported in previous studies. A brief family PE is effective in the prevention of relapse (Shimazu et al., 2011) and a reduction of the psychosocial burden of relatives of patients with MDD (Katsuki et al., 2011). PE was also helpful in increasing rates of adherence to pharmacological treatment (Katon, et al., 2001; Seedat et al., 2008; Von Korff et al., 2003). In these findings, a relapse prevention program is considered a prudent investment of health care resources for the improved care of depression (Simon et al., 2002).
Conclusions
PE is a psychosocial tool that has been comprehensively documented as an effective treatment for schizophrenia and bipolar affective disorder along with pharmacological therapy. Thus, the present systematic review identified selective studies regarding the effectiveness of PE in adult patients with major depressive disorder and their families. Moreover, the papers selected suggest that PE is effective in improving the clinical course, treatment adherence, and psychosocial functioning of depressive patients. Thus, further RCTs to better elucidate the effectiveness of PE in patients with MDD are still needed.
Footnotes
Acknowledgements
To Carolina Fernandez, Marina Maia, Luiz Braga and Ana Maria Stingel, who helped with style corrections and grammar.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.