
Abstract
The aim of the present study was to critically appraise current conceptual approaches; demographic, neurobiological and clinical correlates; and management strategies of treatment-resistant depression (TRD), especially in light of recent research findings. To this end, a review of the relevant English-language literature was undertaken using Medline, Embase and Psychinfo. TRD has been defined in conceptually restrictive terms as symptomatic non-response to physical therapies alone, with little systematic study of aetiology made. It is likely that a range of sociodemographic (such as higher socioeconomic status), genetic (such as variation in functional monoamine polymorphisms) and clinical variables (such as signal hyperintensities seen on structural neuroimaging scans) are responsible for non-response in individuals. There is insufficient evidence to suggest that TRD is associated with specific subtypes of depression, physical comorbidity, personality or chronicity. The large-scale Sequenced Treatment Alternatives to Relieve Depression (STAR∗D) and other studies have suggested that a structured psychotherapy such as cognitive behaviour therapy may be as effective as medication in initial drug non-responders. Also conventional alternatives such as the use of older antidepressant classes, pharmacological augmentation or electroconvulsive therapy in established cases of TRD are not as effective as traditionally thought. There is insufficient preliminary evidence to make formal recommendations about the use of novel brain stimulation techniques in TRD. TRD should be re-defined as the failure to reach symptomatic and functional remission after adequate treatment with physical and psychological therapies. Treatment resistance may be more usefully conceived within the context of well-defined cohorts such as patients with specific subtypes of depression. Although neurobiological markers such as gene polymorphisms, which are potentially predictive of medication tolerance and efficacy, may be used in the future, it is likely that sociocultural variables such as beliefs about depression, and evidence-based treatments for it, will also determine treatment resistance.
Keywords
The concept of treatment-resistant or refractory depression (TRD), first used in 1974 [1], [2], has spawned much literature but basic issues such as a standardized definition and aetiology remain elusive. Despite advances in our understanding of depression, TRD is still a significant challenge for clinicians and their patients, with non-response in at least one-third of clinical samples [3].
Recent research has shed light on structural brain changes and psychosocial factors relevant to TRD, biological markers of treatment response, and the efficacy of both conventional and novel therapies in the management of treatment resistance.
The aims of the present paper were to critically review TRD – its definition, conceptual basis and treatment approaches – and to outline clinical and other correlates.
Methods
The authors reviewed the published literature for the years 1995–2007, using the search engines Medline, Embase and Psychinfo. Search terms used were treatment-resistant/refractory depression, while the terms depression (response, resistance, refractory and outcome) were each combined successively with demographics, age, physical illness, and genetics. Additional articles were retrieved manually from the results of the initial electronic search. Only articles published in English were considered.
Definitions of TRD
Numerous definitions of TRD have been proposed over the past 30 years or so, many of which are similar or overlap (Table 1). While there is an absence of formal diagnostic criteria, proposed features of TRD have evolved over time, with broad agreement that TRD is characterized by (i) the syndrome of unipolar depression; (ii) the failure of antidepressant medication, which has been defined either categorically, for instance the failure of at least two antidepressants from different pharmacological classes [6], or according to increasing levels of resistance [9]; (iii) each antidepressant medication trial being adequate in terms of dose [1]; duration [7]; compliance and tolerability [12]; and (iv) the absence of physical illness or psychosocial dysfunction, which should be the primary focus of treatment [11].
Definitions of treatment resistance based on different principles
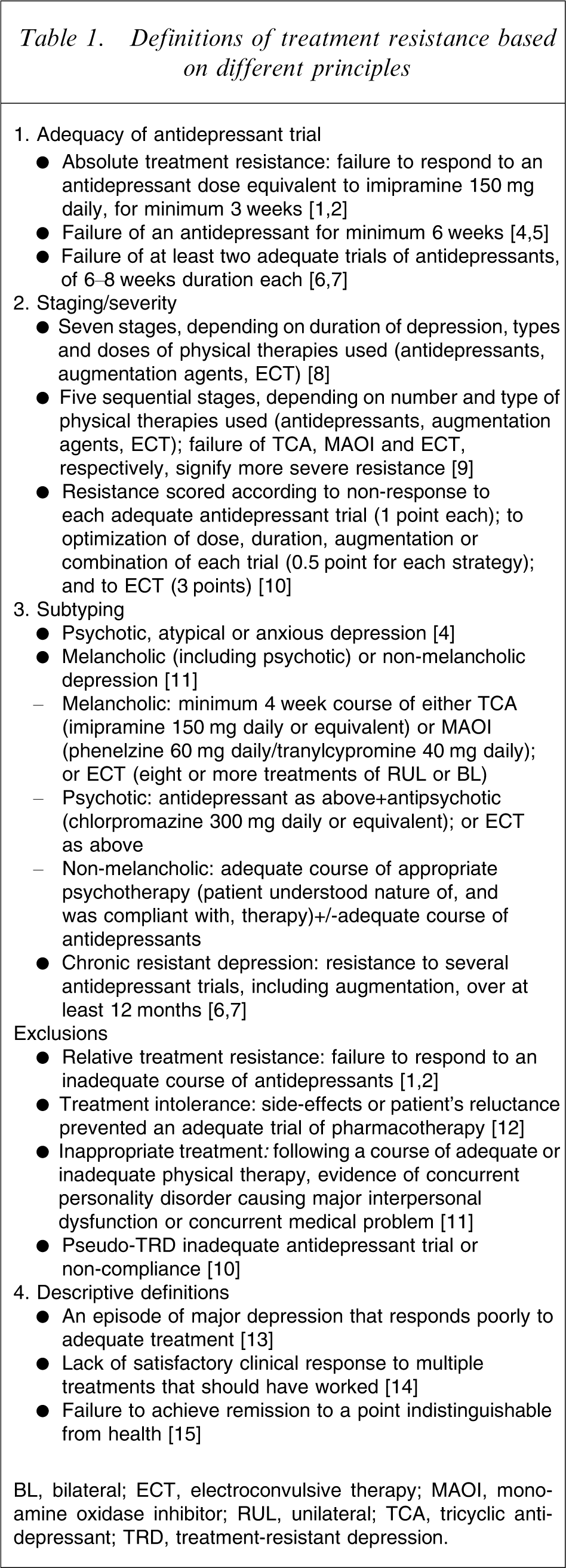
BL, bilateral; ECT, electroconvulsive therapy; MAOI, monoamine oxidase inhibitor; RUL, unilateral; TCA, tricyclic antidepressant; TRD, treatment-resistant depression.
Several recommendations from the early literature need revision, in particular an adequate dose being relative to imipramine 150 mg daily [1]. The stipulation of an adequate duration of 3 weeks [1] has been supported by trials that show that a statistically significant difference in mean Hamilton Rating Scale for Depression (HRSD) scores between drug and placebo may be demonstrated at 3–4 weeks [16]. That the magnitude of this difference increases with study length and that some patients, especially the elderly, demonstrate a slower rate of response would make the later recommendation of 6–8 weeks as an adequate treatment trial [7] more appropriate.
Although psychiatry has developed a clear lexicon for denoting improvement in depression [17], there are only descriptive, rather than objective, definitions of resistance (Table 1). One solution to the absence of an agreed definition of resistance is to adapt from the literature of treatment outcome studies of depression. ‘Response’ has been accepted as a 50% decrease from the baseline score on a standard rating scale such as the HRSD or the Montgomery–Äsberg Depression Rating Scale (MADRS) [18].
More recent studies have preferred ‘remission’ (HRSD score <8) as a more rigorous marker of persistent improvement [19], [20]. Importantly, discordance between symptomatic improvement and improvement in psychosocial function has suggested that symptom-based measurement of remission alone is inadequate [21]. For instance, patients with no symptoms and impaired function reported similar levels of quality of life as those with persistent symptoms and no impairment [22].
Another difficulty in defining resistance relates to patients who demonstrate an initial improvement that is not sustained. A standard duration criterion of 8 weeks of sustained remission has been used to denote recovery [23]. Resistance may then be reasonably defined as a failure to achieve sustained remission, which in turn seems best defined by symptomatic and functional recovery over a prolonged period of at least 8 weeks.
Conceptual basis of TRD
Although several authors have identified patients with TRD as being heterogenous [24], only a couple have advocated classifying TRD into empirically derived subtypes to improve treatment specificity and outcome [4], [11]. The literature has tended to take a narrow conceptual view of what is meant by ‘depression’ in TRD. The approach of conceptualizing depression as a unitary disorder with a single pathophysiology [25] has been criticized by a number of eminent authorities [26–28].
The inclusion of multiple potential clinical phenotypes, yet defining TRD in terms of non-response to physical therapies alone, seems contradictory and self-limiting [9], [10]. This is most apparent in the failure to incorporate psychological therapies.
This approach ignores the tradition of research centred on validating distinct phenotypes of depression by treatment specificity and longitudinal outcome. Such a model distinguishes between four broad types of depression currently best defined according to cross-sectional phenomenology, and will be used as a relevant framework in this paper. These are as follows: (i) melancholic (endogenous) depression signifies a subtype with a typical symptom profile, psychomotor changes, a comparatively lower rate of placebo response, and no clear evidence of response to the psychotherapies [29–31]; (ii) psychotic depression, a subgroup with melancholia, with additional delusions or hallucinations; (iii) anxious (neurotic) depression, which lacks the aforementioned features and presents with associated symptoms of anxiety and particular personality or temperamental variables [32]; and (iv) atypical depression, which has been defined by reactivity of mood, reversed neurovegetative symptoms and interpersonal sensitivity to rejection [33].
Current treatment approaches to TRD
The current conceptual and treatment approach to TRD is best exemplified by a frequently quoted paper by Thase and Rush, published a decade ago [9]. This particular staging method advocated five levels of resistance, starting at resistance to one antidepressant trial (stage 1), then resistance to at least two classes of antidepressants (stage 2), additional resistance to a tricyclic antidepressant (TCA; stage 3), additional resistance to a monoamine oxidase inhibitor (MAOI) antidepressant (stage 4), and additional resistance to bilateral electroconvulsive therapy (ECT; stage 5).
This proposal may be viewed as a depression treatment algorithm, albeit unintendedly, with several important notions about treatment efficacy. These are that (i) an alternate antidepressant class should be tried after failure of the first; (ii) TCA and MAOI antidepressants should be reserved as later treatments; and (iii) ECT should be used as a last-line physical therapy; while (iv) psychological therapies have been omitted altogether. A number of recent studies allows more formal evaluation of the utility of this system.
The results of the STAR∗D trial of non-psychotic depression in some 2876 patients attending primary care and psychiatric settings were not supportive of the first two notions. STAR∗D reported an initial remission rate of 36.8% with the selective serotonin re-uptake inhibitor (SSRI) antidepressant, citalopram [20]; yet the rate of remission in citalopram non-remitters who participated in the second phase of that trial (30.6%) was not statistically different whether they were switched to another SSRI (sertraline), a SNRI (venlafaxine), or an NDRI (bupropion) antidepressant [34]. Subsequent phases of that study showed that augmentation with either lithium or tri-iodothyronine achieved modest (13.7%) gains in remission [35], and that another switch to a fourth medication strategy (including the MAOI, tranylcypromine) yielded even more modest (13.0% remission) results [36].
The strategy of sequential antidepressant trials produced a pattern of diminishing returns in STAR∗ D, in which the cumulative remission rate was 67%, so that more was not better. Higher relapse rates were seen when more antidepressant treatments had been tried, even in patients with symptomatic remission [3].
The practice of withholding TCA or MAOI antidepressants until later in management is largely due to their potentially greater adverse effects and lethality, or dietary restrictions. Yet the prolonged use of antidepressants that target only serotonergic and noradrenergic neurotransmission may be associated with treatment resistance in some patients (this area will be discussed more fully in a following section).
Similarly, viewing ECT as an end-stage therapy, no doubt because of stigma and the need for anaesthesia, is also flawed in medication-resistant patients. ECT response rates were lower (42%) in patients with adequate pre-ECT pharmacotherapy (i.e. TRD) compared to rates (69%) in those without prior treatment resistance [37]. Pre-ECT resistance to pharmacotherapy is also a potent predictor of relapse after ECT [38].
Finally, the STAR∗D series emphasizes the need for any staging of TRD to incorporate psychotherapy. Cognitive therapy, either alone or in combination with a failed initial pharmacotherapy, was as effective a strategy as switching antidepressants, although associated with a slower rate of response [39]. Elsewhere the addition of a structured psychotherapy such as cognitive behaviour therapy (CBT) or interpersonal therapy (IPT) to pharmacotherapy has improved response rates in resistant or partially responsive depression [40], [41].
Have novel physical therapies reduced the rate of TRD?
Newer antidepressants may theoretically lower the rate of TRD by improving drug tolerability and adherence. A review of 75 placebo-controlled antidepressant trials between 1981 and 2002 showed that the overall rate of drug (and for that matter placebo) response had increased over time [16]. Yet neither the rate of response nor effect size was substantially better for newer (SSRI) drugs over older (TCA) drugs.
The continuing failure for a substantial group of patients with depression to achieve remission with conventional antidepressants has led to the study of novel brain stimulation or neuromodulation techniques. Two such therapies, repetitive transcranial magnetic stimulation (rTMS) and vagus nerve stimulation (VNS), have been studied in TRD populations, although initial results have been modest or limited by methodology.
The rate of remission in a TRD group receiving VNS and treatment as usual (TAU; 27%) was twice as high as those receiving only TAU in a non-randomized multicentre trial [42]. Two year follow up of this cohort has shown persistence of improvement, with around three-quarters of the sample remaining well at 24 months [43]. An open study of 11 patients with chronic TRD reported a 12 month remission rate of 27% [44].
A multicentre trial of real versus sham rTMS of patients who had failed antidepressant medication showed a combined response and remission rate of 17% for active rTMS [45]. Another study showed no difference in outcome at 6 months in treatment-resistant patients assigned to either rTMS or ECT, but marked superiority was demonstrated for ECT in the rate of acute remission (59% vs 17%) [46].
These studies of novel physical therapies again highlight the pitfalls of defining TRD as a biological problem that awaits a gold standard physical therapy. There may be as much value in highlighting non-biological factors in the presentation and management of TRD.
Sociodemographic correlates of treatment resistance
Demographic variables such as Caucasian ethnicity, female gender, better education, [20], and residence in a middle-income census tract [47] have been associated with better response to antidepressants. Adverse life events have predicted lower tendency to remission in depression [48].
These findings could be interpreted to support a hypothesis that social advantage is inversely related to treatment resistance, for which several mediating factors may be operative. For instance, health literacy, that is, the capacity for basic reading and numeracy tasks needed for functioning in the health system, may impact on the ability to act on treatment advice [49].
Mental health literacy, that is, knowledge and beliefs about mental disorders [50], may also be relevant. Community preference for lifestyle changes and unproven complementary therapies to treat depression [51] may delay help seeking from an appropriate professional and the acceptance of effective treatments, ultimately leading to the development of TRD. For instance, evidence-based treatments such as taking an antidepressant, seeing a general practitioner or consulting a psychologist are increasingly sought as levels of psychological distress rise and peak in those with the highest level of distress [52]. The importance of individual patient preference and treatment availability was highlighted by a study of primary care patients, with a preference for psychotherapy over antidepressants, who tended to forego all treatment if counselling was not offered [53].
Attitudes to treatment may partly explain differences in outcome by gender, with young women significantly more likely to identify a vignette of depression, and young men more likely to endorse using alcohol over antidepressants for depression [54].
There has been no formal study of ethnicity in TRD, although again patterns of treatment preference may help explain outcome differences. African– and Hispanic–Americans were more likely than white Americans to prefer counselling to antidepressant medication, which was perceived as ineffective and addictive [55]. In London, south Asian patients were less likely to receive antidepressant medication [56], although this was at least partly due to the prescribing practices of south Asian-trained general practitioners [57].
Clinical correlates of treatment resistance
Personality
There is a longstanding perception that personality pathology adversely influences depression outcome [58]. Yet two recent reviews came to very different conclusions.
A meta-analysis of 34 studies of drug and/or psychological therapy concluded that comorbid personality disorder was associated with a doubling of the risk of a poor outcome of depression [59]. Its conclusion was limited by the exclusive use of studies that used categorical diagnoses of mainly DSM personality disorder, which themselves have not been formally validated. Also, that patients with personality disorder were more severely depressed may have influenced outcome data.
In contrast, another meta-analysis of only studies of physical therapies showed no effect of personality on depression outcome [60]. Most of the studies reviewed had a small sample size, although the largest trial reported no difference in outcome either [61]. A study that specifically compared patients with TRD and those without found no difference in the prevalence of personality disorder [5].
When dimensional personality traits have been considered, only neuroticism has been associated with poorer long-term outcome [62]. Yet many neuroticism items overlap with items contained in the HRSD, which is most commonly used to measure outcome, and neuroticism scores tend to improve along with depression anyway.
Comorbidity with other disorders
The presence of anxiety disorders, in particular obsessive–compulsive and post-traumatic stress, alcohol and substance use/dependence disorders, has been associated with a reduced rate of depression remission [20]. These data were derived from the STAR∗D series, so it could be argued that patients were treated for depression, and comorbid conditions were not a specific focus of treatment.
In contrast, comorbid physical illness has not been associated with reduced response to treatment in studies that have provided intensive multi-focal treatment including antidepressants. A study that randomized patients with depression and multiple chronic physical illnesses to either case management or to TAU did not find that physical comorbidity predicted poorer response [63]. A similarly designed study found that chronic pulmonary disease adversely affected outcome in the TAU group but not in the intervention group, concluding that any association between physical illness and depression outcome was due to the intensity of treatment provided [64].
An observational study of patients with heart failure and chronic pulmonary disease, treated with antidepressants and psychotherapy, found that low levels of overall physical morbidity predicted good outcome at 6 weeks but not at 24 weeks [65]. Other samples have confirmed that physical comorbidity does not predict poorer response to antidepressants alone [66]. For instance, the degree of physical illness did not influence eventual outcome in fluoxetine non-responders assigned to one of three groups: increased dose fluoxetine, lithium augmentation, or desipramine augmentation [67].
Chronic depression
It has been assumed that there is significant overlap between TRD and chronic depression (defined as a duration of 24 months without full or sustained remission [68]), with chronicity regarded as a marker of severe treatment resistance [69]. Yet only around 25% of sufferers with chronic depression have failed previous antidepressant trials [68].
The largest randomized controlled trial of patients with chronic depression included those with partial response to prior drug trials [70]. The antidepressant, nefazadone, was as effective as cognitive behavioural analysis system of psychotherapy (CBAS), and the combination of the two treatments more so. A meta-analysis of seven studies involving some 900 patients concluded that the combination of pharmacotherapy and psychotherapy was more effective than psychotherapy alone in moderate chronic depression [71].
These findings again highlight the importance of incorporating psychological therapy in treatment-resistant populations. This group tends to experience issues such as financial adversity, occupational loss, social isolation and irrational cognitions that perpetuate depression, and may be more appropriately managed with a psychological, rather than an alternate pharmacological, treatment [14]. A number of structured psychotherapies such as IPT, CBT and CBAS have proved effective, and no clear evidence for the superiority of one specific therapy over another has been reported [14].
Depression subtypes
Few studies have attempted to identify depression subtypes in TRD populations. One that did so reported an overrepresentation of melancholic (psychomotor changes) but not atypical (hypersomnia and hyperphagia) features in a ‘high treatment resistance’ group [72]. The authors hypothesized that melancholia was the prototype for TRD, but the sample was derived from a tertiary referral clinic and the results may not be generalizable.
There have been several studies that found no relationship between depressive subtype and treatment response [23], [73], [74]. Although one strength of all these studies is medium- to longer-term follow up, differences in the way subtypes are characterized in the literature is a confounding issue, which is particularly the case for atypical depression [75]. It is notable that the STAR∗D series did not formally attempt to study treatment response by subtype.
An apposite hypothesis is that depression subtypes have differential sensitivity to specific antidepressant classes [76], so that failure to treat according to this principle may increase the tendency to treatment resistance. The best evidence here is the apparent superiority of the TCA class over the SSRI class in melancholia [77], especially in older age [78]. In psychotic depression, although the clinical wisdom is that combination antidepressant and antipsychotic therapy is more effective, the quality of the evidence is limited by the paucity of studies, low sample sizes and heterogeneity in diagnostic criteria [79]. The perception that ECT is more effective in melancholic and psychotic depression was not supported by a large multicentre study in which there was no difference in the presence of psychomotor change or psychosis between effective and ineffective forms of ECT [38].
A seminal characteristic of atypical depression was the initial finding of superior response to a MAOI (phenelzine, 71%) over a TCA (imipramine, 50%) and placebo (28%) [80], [81]. Since then, efficacy has been demonstrated for the SSRI class in atypical depression [82], including one study that suggested that this was predicted by temperamental characteristics rather than neurovegetative symptoms [83].
The lack of a clear correlation between clinically determined subtypes of depression and treatment resistance suggests the need to re-assess this relationship using subtypes with a pathophysiological basis.
Biological correlates of treatment resistance
Structural brain changes
A more recently defined depression subtype is ‘vascular depression’, which presents with late age at onset (typically ≥50 years), greater psychomotor retardation, infrequent family history, associated vascular disease or risk factors, and diffuse cerebrovascular changes [84]. The latter has been demonstrated by structural neuroimaging techniques, in particular cerebral magnetic resonance imaging (MRI), on which an increase in signal hyperintensities has been equated with vascular damage. Both Alexopoulos et al. [84] and subsequent authors also reported poor response to antidepressants and to ECT in patients with a high vascular load [85], [86].
The importance of lesion location in vascular depression was highlighted by one study that found an association between poor antidepressant response and pontine and basal ganglia vascular lesions [87]. Longitudinal study has shown that depressed patients with less progression of white matter hyperintensities on cerebral MRI were more likely to achieve sustained remission, after controlling for age, depression severity and physical illness [88]. Subcortical grey matter hyperintensities too have been shown to predict poor response to antidepressants [89].
That education in the Taylor et al[88] study and subjective social support in the Steffans et al. [89] study also contributed to poor antidepressant response, highlights the interaction of biological and psychosocial factors in vascular depression. It is consistent with the threshold hypothesis in which accumulation of lesions is required to predispose an individual to depression, which may be triggered by non-biological factors [84].
One implication of these findings is that treatments that are beneficial in cerebrovascular disease need to be considered in vascular depression. The addition of the calcium-channel antagonist, nimodipine, to a vascular depression cohort already treated with fluoxetine resulted in improved response, remission and lower relapse compared to fluoxetine alone [90]. The authors speculated that nimodipine, which dilates the small resistance cerebral vessels and increases cerebral blood flow, may have prevented further neuronal damage from cerebrovascular disease. Problem-solving therapy has been shown to be more effective than supportive therapy in this population [91].
Dopaminergic dysfunction
Two recent review papers have explored another possible subtype of depression marked by dopaminergic dysfunction [92], [93], which is of potential relevance to TRD. This hypothesis is based on the limited efficacy of serotonergic and noradrenergic antidepressants, which have only small or indirect effects on dopamine transmission. Compared to non-responders, patients who do respond to SSRI medication have exhibited increased dopamine D2 receptor binding, the degree of which correlated with improvements in HRSD scores [94].
In addition, key features of depression such as anhedonia, amotivation, cognitive and psychomotor cognitive changes are all regulated by dopaminergic pathways [93]. Cerebrospinal fluid studies of dopamine neurotransmission have reported that concentrations of dopamine metabolites such as homovanillic acid (HVA) are lower in depression, and that this was accentuated in patients with psychomotor changes [92]. One study found that the effectiveness of three antidepressants in patients with psychomotor retardation was correlated with the level of dopamine transmission [95].
In treatment-resistant patients, reduced levels of HVA and inverse correlation between HRSD scores and dopamine turnover have been noted [96]. In addition, reduced dopamine transmission may lead to compensatory upregulation of D2 (dopamine) receptors. D2 receptor binding studies in depression samples before and after antidepressant treatment have shown conflicting results, including increased or no change in binding [94], and decreased binding in another [97]. Results may have been confounded by the use of varying antidepressant classes, duration of treatment and small sample sizes.
These findings suggest that antidepressants with specific dopaminergic activity, in particular MAOIs, need to be tried earlier in patients with the aforementioned symptom profile. Other dopaminergic agents have been studied in TRD. For instance, augmentation of citalopram with the stimulant methylphenidate in older patients was more effective than citalopram alone [98]. The same agent was not effective in a younger sample [99], although this may have been due to the absence of patients with psychomotor change [100]. The D2 agonist, bromocriptine, has been effective in open-label studies of TRD [101].
Hypothalamus–pituitary–adrenal axis changes
There are several lines of evidence suggestive of hyperactivity of the hypothalamus–pituitary–adrenal (HPA) axis in depression [102]. The most widely studied marker of HPA axis function is the dexamethasone suppression test, subsequently refined as the dexamethasone/corticototropin-releasing factor test (DEX/CRF). Patients with depression do not demonstrate the normal pattern of cortisol suppression after administration of the glucocorticoid, dexamethasone, and after CRF injection [103].
Of particular relevance to TRD is that persistent cortisol elevation has been demonstrated to have high sensitivity as a prognostic marker of poorer antidepressant response [104] and greater relapse [105]. The routine use of tests of HPA axis function in depression, however, is limited by several variables.
The first limitation is that HPA axis changes tend to vary by depressive subtype. Psychotic depression has been associated with a particularly high rate of cortisol non-suppression [106], [107], which has been less evident in atypical depression [108] and chronic depression [109]. Although no association has been found between HPA hyperactivity and symptom-based criteria of melancholic depression, a robust association has been found when psychomotor disturbance is used as a marker of melancholia [110].
The second limitation is that the DEX/CRF test may be a trait rather than a state marker. This has been suggested by the finding that asymptomatic first-degree relatives of patients with depression exhibit decreased cortisol suppression [111]. A polymorphism in the FKBP5 gene has also been associated with DEX/CRF results [112].
The third limitation is that dysfunction of the HPA axis may also be dependent on specific environmental factors. A study of the DEX/CRH test in men with current depression and a history of early life stress (emotional, physical and sexual abuse) showed increased cortisol response compared to both healthy controls and men with depression but no early life stress [113]. Cortisol elevation was associated with the earlier onset, duration and severity of abuse.
Thus the DEX/CRH test could be a marker of certain subtypes of depression mediated by both genetic vulnerability and childhood trauma. Chronic elevation of glucocorticoids has been associated with hippocampal and prefrontal damage, which may in turn cause emotional dysregulation and mediate treatment resistance [114].
Mifepristone, a glucocorticoid receptor antagonist, has been shown to be effective in a large sample with psychotic depression, randomized to mifepristone or placebo [115]. That study was limited by the demonstration of response on the Brief Psychiatric Rating Scale but not to HDRS, and a larger than expected placebo response rate.
Pharmacogenetics
Pharmacogenetics is concerned with the identification of genetically determined differences in drug response among individuals. The advantages of this method are that measurement of genotype is not confounded by illness or treatment, and there is little measurement error in contrast to other biological markers such as HPA axis [116]. Current studies have been limited by the use of short-term antidepressant trials, heterogenous depression phenotypes, and the absence of placebo controls.
Most genetic association studies in the mood disorders have focused on functional monoamine polymorphisms, which are variations in genetic expression that occur in >1% of the population [117]. The best studied is the functional polymorphism in the promoter region of the serotonin transporter gene (SLC6A4), known as 5-HTTLPR, which has been associated with depression-related trait scores [117], [118].
Of relevance to TRD is that the ‘short’ form of 5HTTLPR (S allele) may reduce the efficacy of SSRI antidepressants [119], although this has not been replicated in age-specific and non-European cohorts. A study of late-life depression found that the poor outcome of S allele carriers was more significantly related to tolerance rather than SSRI efficacy [120]. In both Korean and Japanese patients, the S allele was associated with a better response to SSRI medication [121].
While a multitude of other polymorphisms have been studied as markers of treatment response [122], [123], two are relevant to areas already discussed in this paper. One, already discussed, is the FKBP5 gene, which has been associated with cortisol non-suppression in the DEX/CRH test, as well as with antidepressant response.
The other comes from study of the AGTR1 gene, which is implicated in cerebral infarction [124]. Patients with vascular depression and the C/C genotype of the A1166C polymorphism were less likely to achieve remission from a standardized treatment algorithm. Yet this genotype was present in only 7% of the sample and subjective social support was a more significant predictor of response, highlighting once again the limitation of a narrow biological approach to TRD.
Conclusion
It is difficult to incorporate the plethora of often contradictory findings in TRD into a coherent whole, which highlights the conceptual limitations of TRD. This entity has been significantly limited by the notion of depression as a unitary disorder, with resistance framed in terms of non-response to physical therapies alone. Studies of TRD tend to originate from clinics based in academic settings, which underlines the importance of the STAR∗ D trial, which included primary care settings.
It has been difficult to achieve consensus of very basic concepts such as resistance per se. We propose that resistance could be understood as the failure to achieve sustained symptomatic and functional improvement, which may be defined using standard rating scales (Table 2).
Proposed criteria for TRD
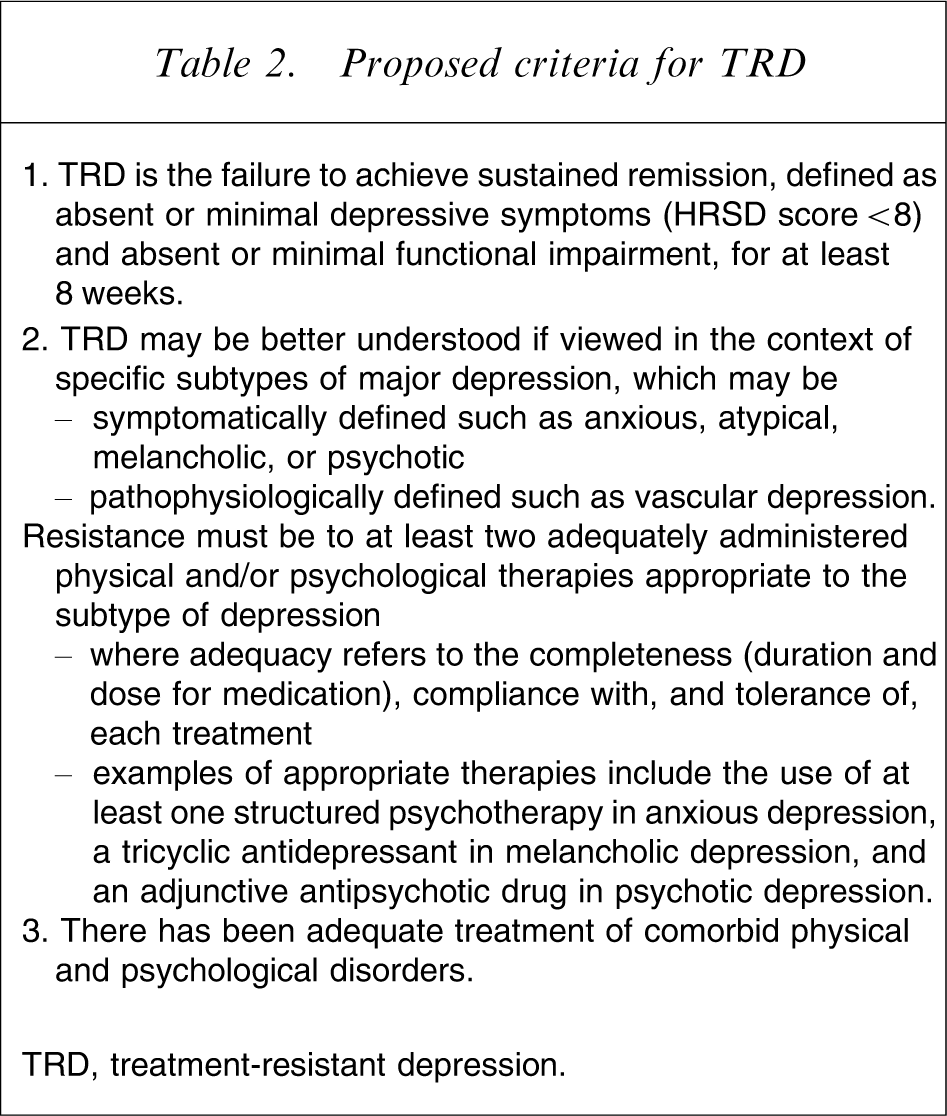
TRD, treatment-resistant depression.
The use of conventional antidepressants has been associated with TRD in approximately one-third of cohorts. Preliminary evidence does not suggest that the rate of TRD has declined with either novel antidepressant or brain stimulation therapies, which themselves may be limited by the need for 4–6 weeks of almost daily treatment in the case of rTMS, or surgery in the case of VNS. Yet structured psychotherapy substantially increases response in non-psychotic depression and is essential to any future definition of TRD.
Treatment response has been associated with a number of sociodemographic factors, while patient beliefs about depression and treatment preference, in particular for psychological therapy over medication, may also influence outcome. The association with comorbid anxiety and substance use disorders may reflect inadequate treatment of these disorders rather than true treatment resistance, not least because there is no such association with physical disorders that have been treated with multi-focal methods.
There has been insufficient study of clinically defined depressive subtypes to determine correlation with treatment resistance. Although melancholia has been proposed as the prototype for TRD, varying definitions, especially the accentuation of symptoms by some researchers and signs by others, limit any firm conclusion. Psychomotor change has been well associated with a number of putative markers of treatment resistance such as cerebrovascular disease, dopamine dysfunction and persistent hypercortisolaemia.
Future directions and treatment
It may reasonably be asked whether psychiatry, a specialty bedevilled by more and more categories, needs to promote the study of yet another entity. Although not a specific disorder, TRD does highlight the failure to reach expected outcomes, and ongoing disability in the sufferer. The concept of treatment resistance has also been used in other medical specialities as a framework to guide further studies of aetiology and targeted drug treatment [125].
Importantly, TRD would be useful only if it is not used as a platform for more and more trials of conventional antidepressant therapies, especially in the absence of an aetiological basis. It may also be useful if seen as a marker of the need for adequate psychological therapy.
Future research should aim to study prospectively subjects with well-defined subtypes of depression with an associated pathophysiological basis. Cerebrovascular disease and psychomotor change appear to be the most promising aetiological markers of relevant phenotypes. Both sociodemographic and neurobiological correlates of treatment resistance need to be studied concurrently. Future treatment trials need to incorporate psychological and physical therapies, which need to be matched to particular subtype.