
Abstract
Objective:
Because comorbidity between mental and physical disorders is commonly found in patients, it would be expected that this pattern would also be reflected at the family level. During a recent population-based survey of common mental disorders, respondents were asked about the presence of selected mental and physical disorders in their relatives. The aim of this research was to describe the within-family co-occurrence of selected common physical and mental disorders in a population-based sample.
Methods:
Subjects were drawn from the Australian National Survey of Mental Health and Wellbeing 2007. A modified version of the World Mental Health Survey Initiative of the Composite International Diagnostic Interview (WMH-CIDI 3.0, henceforth CIDI) was used to identify lifetime-ever common psychiatric disorders (anxiety disorders, depression, drug or alcohol disorders). The respondents were asked if any of their relatives had one of a list of psychiatric (anxiety, bipolar disorder, depression, drug or alcohol problem, schizophrenia) or general physical disorders (cancer, heart problems, intellectual disability, memory problems). We examined the relationship between the variables of interest using logistic regression, adjusting for potential confounding factors.
Results:
Compared to otherwise-well respondents, those who had a CIDI diagnosis of major depressive disorders, anxiety disorders, or drug or alcohol abuse/dependence were significantly more likely to have first-degree relatives with (a) the same diagnosis as the respondent, (b) other mental disorders not identified in the respondent, and (c) a broad range of general physical conditions.
Conclusions:
Individuals with common mental disorders report greater familial co-occurrence for a range of mental and physical disorders. When eliciting family histories, clinicians should remain mindful that both mental and physical disorders can co-occur within families.
Introduction
A recent population-based study of mental illness in Australians found that of those with a history of any mental disorder during the previous year, one-quarter (25.4%) had more than one class of disorder (Slade et al., 2009). In other words, comorbidity within mental disorders is common. In addition, comorbidity between mental disorders and a wide range of general physical disorders is also prevalent in the community, and tends to increase across the lifespan (Barnett et al., 2012). Apart from the co-occurrence of disorders within individuals, disorders also tend to co-occur within families. Familial factors, which include genetic factors (e.g. risk alleles segregating within pedigrees) and/or shared environmental factors (e.g. exposure to risk-modifying factors related to lifestyle and socioeconomic status), can contribute to this finding. In addition to these factors, family members of those with chronic physical or mental disorders often face a substantial caregiver burden (Raina et al., 2004). This role can translate into an increased risk of both stress-related conditions like depression and anxiety, and also a range of general physical conditions (Schulz and Beach, 1999; Schulz et al., 1997; Vitaliano et al., 2003).
The co-occurrence of both mental and physical disorders within families is usually assessed by clinicians when taking the routine history (e.g. family history of mental disorders, family history of other conditions). However, convenience samples based on those in contact with services will bias the sample with (a) prevalent cases and (b) those who use services frequently. Register linkage studies can help explore the within-family co-occurrence of disorders. Generally, these studies have focused on the links between one mental disorder and particular physical conditions. For example, studies have suggested that individuals with schizophrenia are more likely to have family members affected by autoimmune disorders (Eaton et al., 2006). Other studies have reported that relatives of those with schizophrenia are less likely to have certain types of cancer (Ji et al., 2012). In the absence of national, comprehensive health record linkage studies, population-based surveys may provide clues into this research question. We had the opportunity to explore the within-family co-occurrence of selected common mental and general physical disorders in a large, Australian community-based survey. In particular, we wished to examine if those with common mental disorders were more likely to report family members with these same disorders, and a range of broadly defined common general physical disorders. Based on findings from previous studies, we hypothesised that both common mental and general physical disorders cluster within families.
Methods
Participants
Subjects were drawn from the Australian National Survey of Mental Health and Wellbeing (NSMHWB) 2007. Details of the methodology have been published elsewhere (Slade et al., 2009). In brief, the NSMHWB was a national face-to-face household survey of community residents aged between 16 and 85 years. Sampling was based on random selection from a stratified, multistage area probability sample of private dwellings. Interviews were carried out by trained interviewers from the Australian Bureau of Statistics, a statutory body responsible for conducting such surveys using ethical protocols that include written consent. In total, 8841 individuals participated in the survey.
Assessment of DSM-IV diagnoses among participants
A modified version of the World Mental Health Survey Initiative of the Composite International Diagnostic Interview (WMH-CIDI 3.0) was used to generate Diagnostic and Statistical Manual of Mental Disorders – fourth edition (DSM-IV)-based diagnoses of a wide range of common mental health disorders including anxiety disorders, major depressive disorders (MDDs), and drug or alcohol abuse/dependence. Full details of these diagnoses are available in our earlier publications (Saha et al., 2011a, 2011b; Saha et al., 2012). In brief, a DSM-IV lifetime diagnosis of anxiety disorders was based on any diagnosis of panic disorder with or without agoraphobia, social phobia, generalised anxiety disorder, obsessive–compulsive disorder, and agoraphobia without panic.
MDDs included mild, moderate, and severe forms of disorders. Allocation to these subtypes was based on the total number of particular depressive symptoms with a duration of at least 2 weeks. Complete details of the symptom list and related rules to deal with multiple episodes can be found in the full report (Australian Bureau of Statistics, 2008). In brief, mild MDD was characterised by the presence of at least four symptoms, moderate MDD by at least six symptoms, and severe MDD by at least eight symptoms. These subtypes of MDD were mutually exclusive.
To explore the presence of DSM-IV alcohol use disorders, participants were initially asked whether they had consumed at least 12 alcoholic drinks (containing 10 g of ethanol) in any 1 year in their lifetime. For the assessment of any drug abuse disorder, subjects were screened for any lifetime use of cannabis, amphetamines or stimulant use. Those participants who screened positive for alcohol or other substance use were then asked a series of questions to establish a lifetime diagnosis of harmful use/dependence disorder (Teesson et al., 2009). For this study, we combined drug abuse/dependence and alcohol abuse/dependence disorders into a single category of drug or alcohol disorders.
Assessment of disorders among relatives
Respondents were also asked a series of questions about the health of their family (e.g. Do any of your immediate family members have any of the following problems?). They were then provided with probes for specific mental health disorders and other non-psychiatric disorders. The probes for mental health disorders were as follows: anxiety, depression, drug or alcohol problems, schizophrenia or psychosis (henceforth schizophrenia), manic depression or bipolar disorder (henceforth bipolar disorder). The probes for non-psychiatric disorders included cancer, serious heart problems (henceforth heart problems), serious memory problem like senility or dementia (henceforth memory problems) and intellectual disability. Finally, respondents were asked to specify the nature of the relationship between the affected relative and the proband. In this study, we restricted our focus to disorders in first-degree relatives (i.e. father, mother, brother, sister, son, and daughter). Because we do not have any additional information on these pedigrees (e.g. the size of the pedigrees, who is deceased, etc.), the raw counts cannot be used to infer the relative force of morbidity for these disorders in the general population.
Many individuals with common mental disorders also act as caregivers to other immediate family members affected by mental disorders. While the survey did not allow precise matching between the respondent’s caregiving role with respect to their affected relative(s), a general question allowed us to estimate the proportion who were in caregiving role for their family members.
Data analysis
For the main analyses, we examined the association between the three DSM-IV categories (MDD, anxiety disorders, and drug or alcohol abuse/dependence) as the predictor variable, and family history of different disorders (psychiatric and non-psychiatric) as the outcome variable using logistic regression. For outcome variables, we combined all yes answers for any particular disorder (e.g. MDD) as the exposed category while all no answers were used as the reference group. Results were presented unadjusted (Model 1) and adjusted for sex and age at testing, as there is evidence that DSM-IV diagnoses vary with age and sex (Model 2).
The sample was weighted to adjust for differential probabilities of selection within households, oversampling of population subgroups, and non-response to match census population distribution on a number of geographic and sociodemographic variables (Slade et al., 2009). The initial weights were calibrated against known population estimates. Replicate weight variables were developed using the jackknife procedure of replication (i.e. the analysis was repeated after one subject was dropped and then the standard error was derived from the distribution of results from all minus one resamples) (Rust and Rao, 1996). For the main analyses, we used the PROC SURVEYLOGISTIC statement in SAS version 9.3 (SAS Institute Inc., Cary, North Carolina, USA) which is capable of dealing with complex survey design) (An, 2004). In addition, we used the PROC SURVEYFREQ procedure for frequency distributions.
Results
Of the 8841 subjects included in the study, 12.8% (n = 1174) had MDD, 16.3% (n = 1473) had an anxiety disorder, and 24.2% (n = 2043) had any drug or alcohol abuse/dependence disorder. Of the 1174 subjects with MDD, 33.3% (n = 359) endorsed the caregiver item. The corresponding percentages for those in caregiving roles with anxiety disorders (n = 1473) and any drug or alcohol abuse/dependence disorders (n = 2043) were 35.4% (n = 498), and 22.4% (n = 462) respectively. In contrast, 20.3% (n = 1538) individuals who had no MDD endorsed the caregiving item, while 19.3% (n = 1399) who had no anxiety disorders, and 21.8% (n = 1435) who had no drug or alcohol abuse/dependence disorders had caregiving roles.
Concerning the distribution of the nominated disorders in the first-degree relatives, the most frequently reported disorders in relatives were heart problems and depression in male and female relatives respectively (see Table 1). Overall, the pattern of these disorders (e.g. male versus female; parent versus sibling versus offspring) was generally consistent with expectations.
Frequency distribution of different disorders in first-degree relatives a by sex (n = 8841).
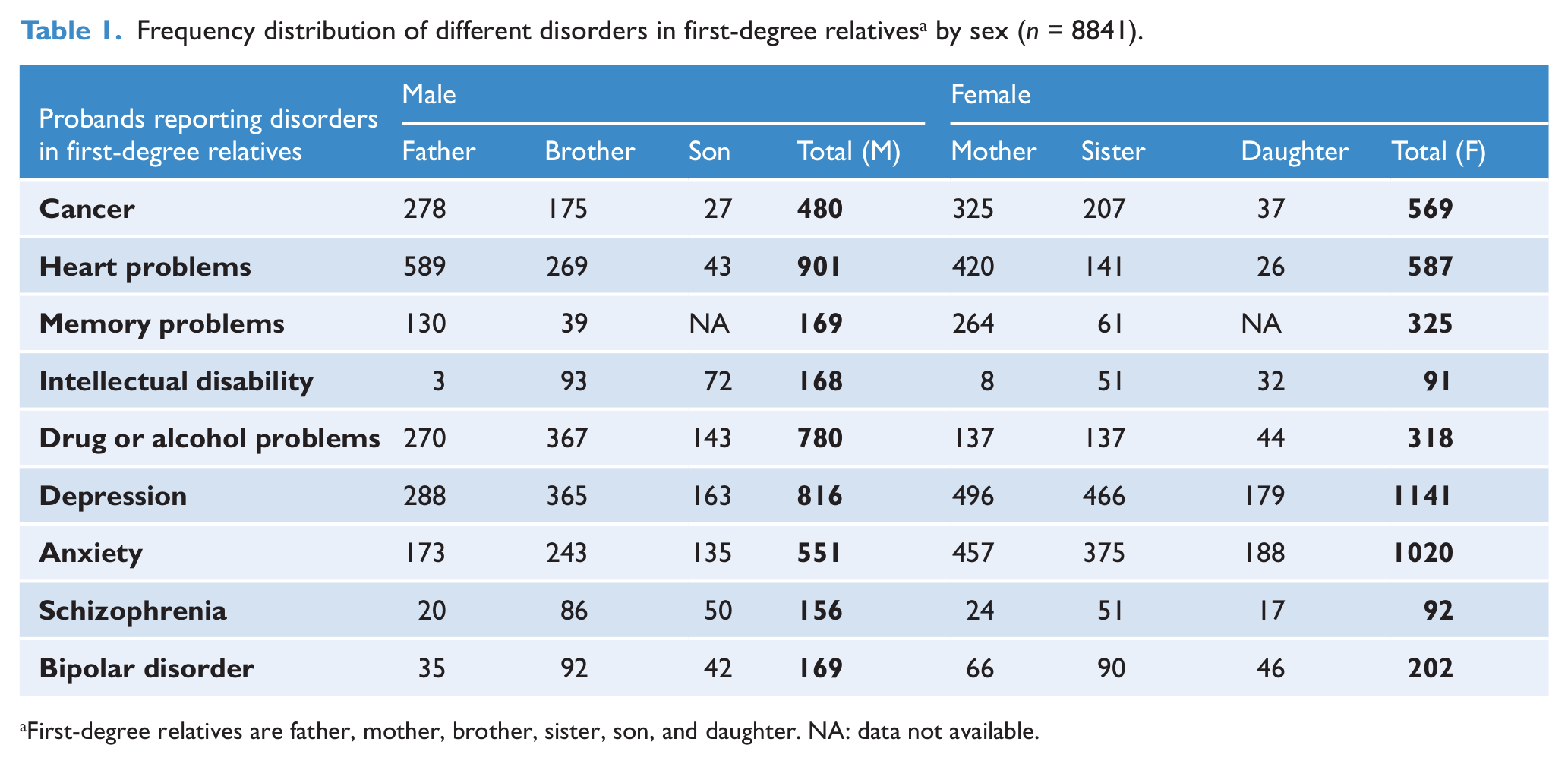
First-degree relatives are father, mother, brother, sister, son, and daughter. NA: data not available.
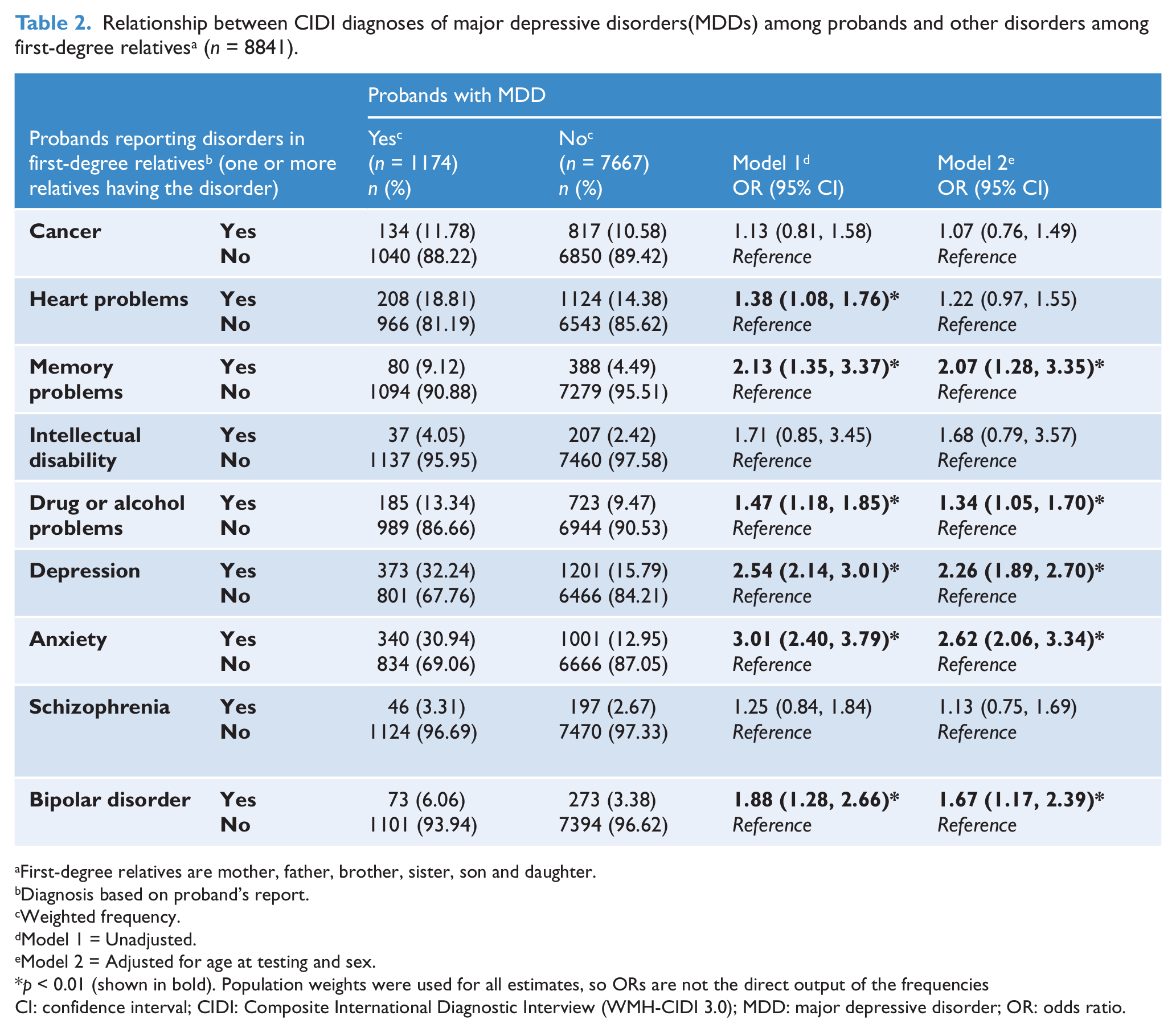
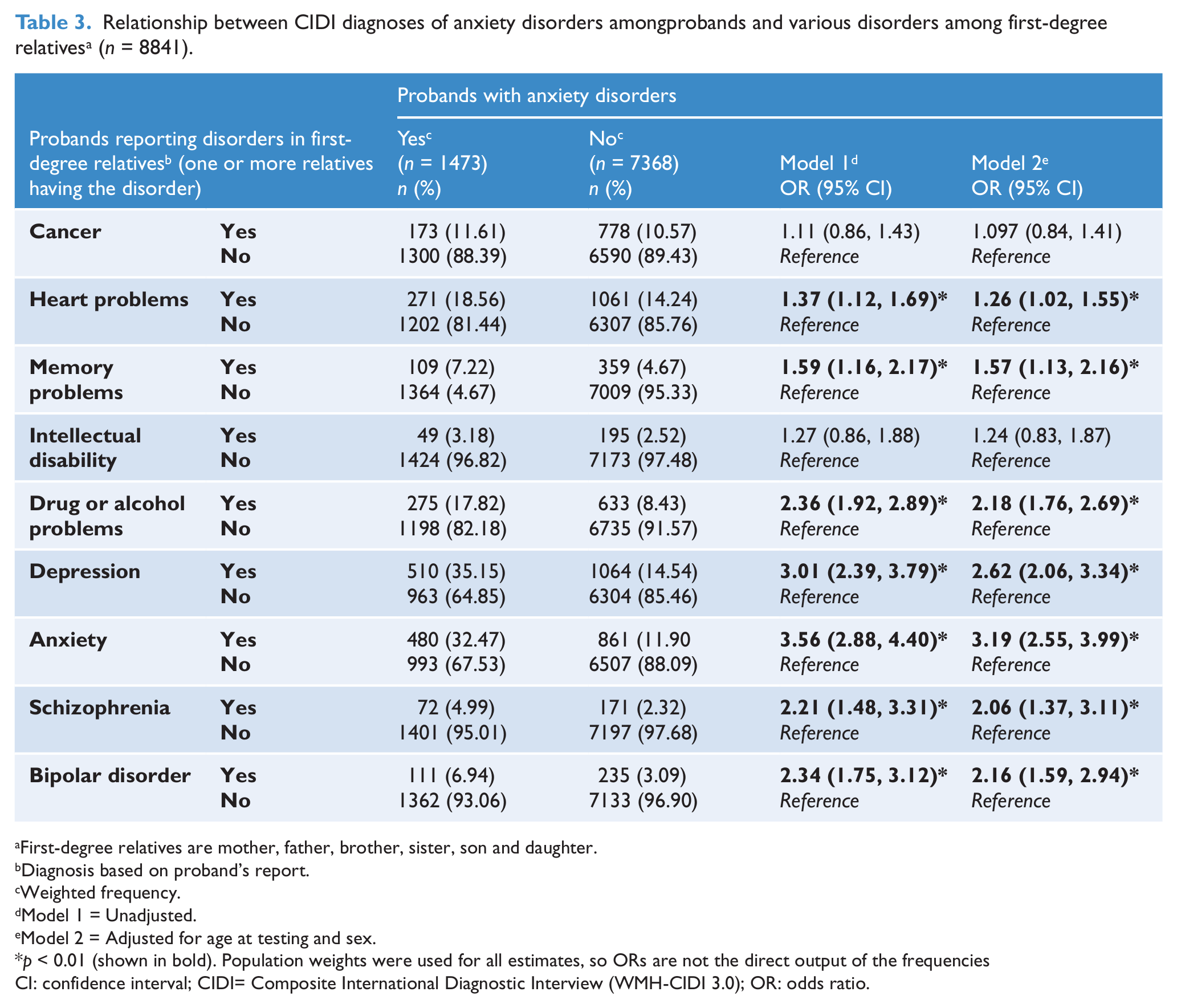
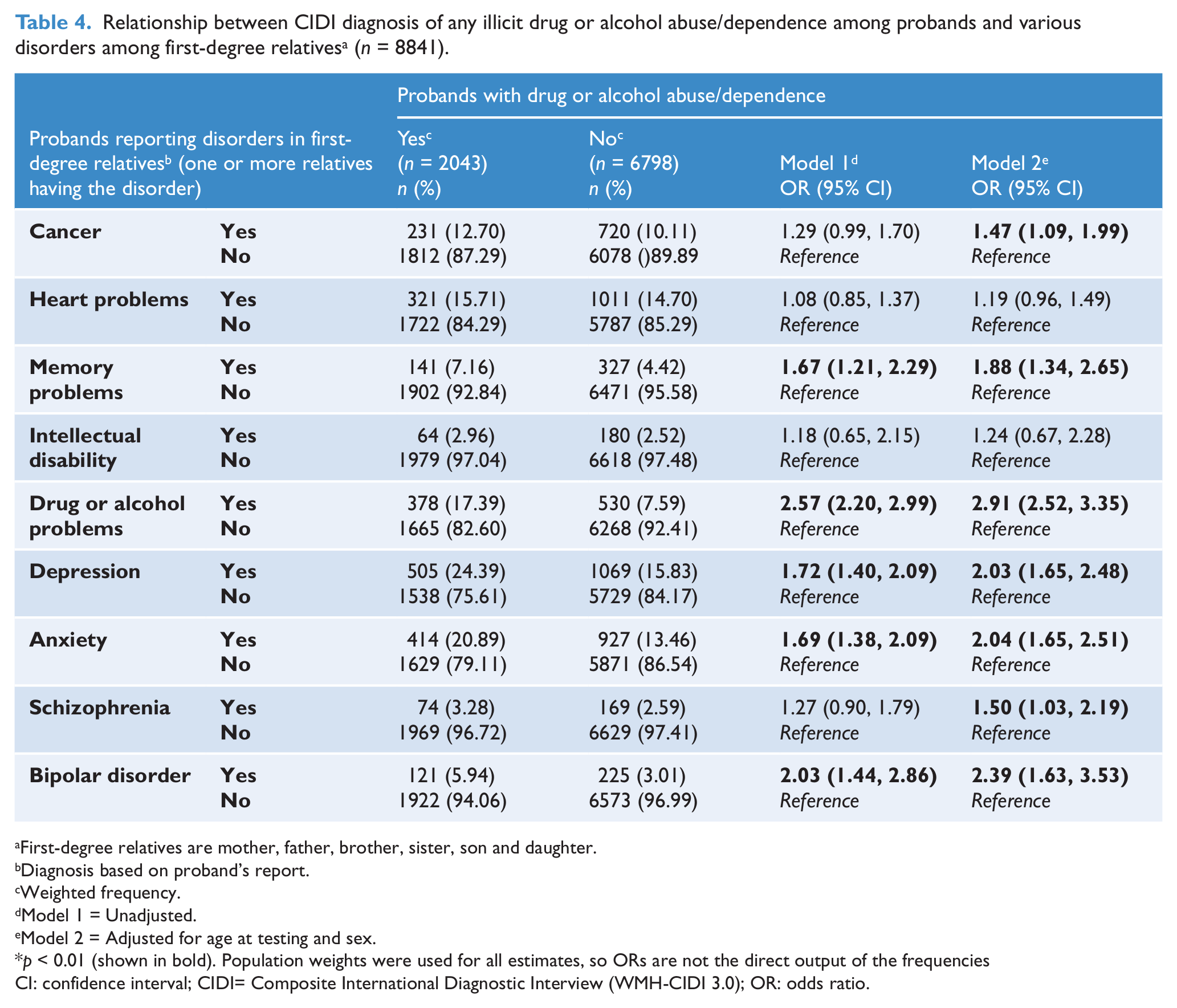
Compared to those without the salient CIDI diagnoses, those with lifetime-ever MDD were significantly more likely to report the following disorders in their first-degree relatives (ranked in descending order of adjusted odds ratios); anxiety, depression, memory problems, bipolar disorder, and drug or alcohol problems. Similarly, those with CIDI diagnosis of anxiety disorders were significantly more likely to report; anxiety, depression, drug or alcohol problems, bipolar disorder, heart problems, schizophrenia, and memory problems. Those with a CIDI diagnosis of drug or alcohol abuse/dependence were significantly more likely to report: drug or alcohol problems, bipolar disorder, depression, anxiety, memory problem, schizophrenia, and cancer (see Tables 2–4).
Relationship between CIDI diagnoses of major depressive disorders(MDDs) among probands and other disorders among first-degree relatives a (n = 8841).
First-degree relatives are mother, father, brother, sister, son and daughter.
Diagnosis based on proband’s report.
Weighted frequency.
Model 1 = Unadjusted.
Model 2 = Adjusted for age at testing and sex.
p < 0.01 (shown in bold). Population weights were used for all estimates, so ORs are not the direct output of the frequencies
CI: confidence interval; CIDI: Composite International Diagnostic Interview (WMH-CIDI 3.0); MDD: major depressive disorder; OR: odds ratio.
Relationship between CIDI diagnoses of anxiety disorders amongprobands and various disorders among first-degree relatives a (n = 8841).
First-degree relatives are mother, father, brother, sister, son and daughter.
Diagnosis based on proband’s report.
Weighted frequency.
Model 1 = Unadjusted.
Model 2 = Adjusted for age at testing and sex.
p < 0.01 (shown in bold). Population weights were used for all estimates, so ORs are not the direct output of the frequencies
CI: confidence interval; CIDI= Composite International Diagnostic Interview (WMH-CIDI 3.0); OR: odds ratio.
Relationship between CIDI diagnosis of any illicit drug or alcohol abuse/dependence among probands and various disorders among first-degree relatives a (n = 8841).
First-degree relatives are mother, father, brother, sister, son and daughter.
Diagnosis based on proband’s report.
Weighted frequency.
Model 1 = Unadjusted.
Model 2 = Adjusted for age at testing and sex.
p < 0.01 (shown in bold). Population weights were used for all estimates, so ORs are not the direct output of the frequencies
CI: confidence interval; CIDI= Composite International Diagnostic Interview (WMH-CIDI 3.0); OR: odds ratio.
Discussion
Individuals with common mental disorders were significantly more likely to report the presence of affected family members with both mental and physical disorders. Approximately, one-third of those with MDD or an anxiety disorder report that they are also caregivers to relatives with health problems, while the comparable proportion in those with any drug or alcohol abuse/dependence disorder is lower (22.4% ). In contrast, only one-fifth of those with no mental disorders reported that they had a caregiving role. The burden of caring for someone with significant health problems is a known risk factor for mental health problems (Pruchno and Resch, 1989; Schulz et al., 1997). It would be of interest to explore the time course of the onset of the caregiver role and mental disorder in prospective, longitudinal studies (Goode et al., 1998).
As expected, respondents with MDD, an anxiety disorder, or drug or alcohol abuse/dependence disorders were significantly more likely to report the same disorder in their first-degree relatives (two- to threefold increased risk). This within-family co-occurrence reflects the well described heritable nature of these particular disorders (Bierut, 2011; Merikangas and Swanson, 2010; Norrholm and Ressler, 2009; Saveanu and Nemeroff, 2012). Twin and other family studies indicate that heritable factors can be shared across a range of disorders (Kendler et al., 2003). For example, twin and health register-based studies indicate that anxiety disorders and depression share an underlying risk architecture (Hettema, 2008) and that common mental disorders share risk factors with substance use disorders (Fu et al., 2002; Kendler et al., 1995, 2003).
In fact, recent mental health register-based studies demonstrate that the within-family co-occurrence of mental disorders is much wider than previously suspected (e.g. bipolar disorder versus schizophrenia, any mental disorder versus risk of schizophrenia) (Dean et al., 2010; Lichtenstein et al., 2009). More recently, evidence from genome-wide association studies suggests that at least some common variants are shared between schizophrenia and bipolar disorder (International Schizophrenia Consortium et al., 2009). With respect to the co-occurrence of different psychiatric disorders within families, our study found that individuals with common mental disorders are more likely to report a broad array of mental disorders in their first-degree relatives.
With regards to physical disorders in the families of those with common mental disorders, we found that memory problems were significantly more common in first-degree relatives of probands with common mental disorders. Interestingly, there is evidence that depression and anxiety could be a risk factor for later dementia (Antonogeorgos et al., 2012; Gallagher et al., 2012; Kessing, 2012). Alternatively, caring for a relative with dementia is a risk factor for depression and anxiety (Dunkin and Anderson-Hanley, 1998). We found a significantly positive association between having an anxiety disorder and having a relative with heart problems. This may be a direct result of the anxiety disorder or may be mediated by other factors, such as cigarette use (Kawachi et al., 1994; Morissette et al., 2007; Suls and Bunde, 2005). The increased risk of cancer in first-degree relatives of those with drug or alcohol abuse/dependence problems is difficult to explain. The relationship was significant after adjusting for age at testing and sex, thus demographic factors do not underpin the association. It is feasible that within-family patterns of smoking and alcohol use contribute to an increased risk of cancer in the proband’s relatives (Lim et al., 2012; Murray and Lopez, 1997; Williams and Horm, 1977).
Our study has several important limitations. As mentioned, we lack information about the size and age distribution of the respondents’ families, and thus cannot derive meaningful estimates of disease risk in the families. Reporting biases may also influence the findings – respondents with a particular disorder may be more likely to recall the same disorder in members of their immediate family. While the mental health disorders in the respondents were formally assessed with the CIDI, we relied on respondent-reported diagnoses in the family members. The validity of these broadly defined domains cannot be evaluated. The probes used in the survey were restricted to a short list of common disorders and, in keeping with health literacy within the general population, were described in generic, everyday terms. While we have age of onset for the respondent’s CIDI-based diagnoses, we lack this information for the affected family members. Thus, we are unable to determine the temporal sequence of disorders within the family (e.g. Did the stress of caring for a disabled relative contribute to mental illness in the respondent?). Finally, the sampling framework in this study was not based on family units, but individuals living within a household. However, we believe that the findings would be broadly representative of the population.
Despite these limitations, our data suggest that individuals with common mental disorders have greater familial co-occurrence for a range of mental and physical disorders in their first-degree relatives. Obviously, family members are key partners in the planning and implementation of service delivery to those with mental disorders. From a service delivery perspective, the added burden of both comorbid mental and physical health within the family unit needs to be taken into account. Clinicians should remain mindful that many individuals with common mental disorder are often also caregivers to their immediate family members. Addressing the burden of care experienced by an individual may be an important psychosocial intervention (Dunkin and Anderson-Hanley, 1998). When eliciting family histories, clinicians should pay particular attention to the co-occurrence of both mental and physical disorders within the family unit.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.