
Abstract
The need to improve the identification and management of psychiatric disorders in the primary care setting has been well documented [1]. Patient, doctor and service factors have all been identified as contributing to the under-recognition and under-management of these conditions. Reasons for this include the stigma for patients associated with a psychiatric diagnosis, public ignorance of mental illness, the lack of diagnostic skills in general practitioners (GPs), and the lack of adequate specialist support services [1–3]. There are now moves to address some of these issues through the development of local and national initiatives [4]. Rather less attention has been paid to the differences in detection and management that are related to patient or doctor characteristics such as sex, ethnicity and socioeconomic status.
Increased recognition of the higher levels of morbidity and mortality experienced by people living in disadvantaged circumstances [5] challenges the health system to reflect on whether the services that are provided to these groups are accessible, appropriate and delivered without bias [6]. People who are unemployed are one group in the community who are recognised as having poorer health status and higher rates of general practitioner consultation [7–9]. Much of this poor health is due to conditions that are psychogenic in origin [10,11]. The National Mental Health and Well-being Study [14] confirmed the findings of other Australian and international studies of an association between unemployment and poor mental health [12,13]. In the National Mental Health and Well Being study 14.9% of people who were unemployed reported an anxiety disorder and 10.1% an affective disorder compared to 7.1% and 3.8% respectively of people in full-time work and 10.2% and 6.4% respectively of people in part-time work [14].
Harris et al. present a further analysis of data collected in a general practice-based study of anxiety and depressive symptoms [15]. It highlights some important differences in the levels of reported anxiety and depressive symptoms between employed and unemployed patients in general practice and in the ways in which employment status influences the management of these conditions by general practitioners.
Methods
The methods used to recruit GPs and patients for this study have been described in detail elsewhere [15]. GPs who participated in the study agreed to recruit 50 consecutive patients each. The study group consisted of patients aged 18 years or older, without a ‘major’ psychiatric condition such as psychosis or dementia, who were recruited by each of the 117 participating general practices in south-east and southwest Sydney.
Patients completed a three page self-administed questionnaire (available on request) while waiting for the GP consultation. Information sought from patients included demographic characteristics (age, sex, country of birth, language spoken at home, and employment status), whether the patient was seeing his/her usual GP, self-reported symptoms of anxiety and depression using a checklist (worry, nerves, stress, anxiety, depression or sleep problems) during the previous 4 weeks, medical treatment received, referral to a range of other health professionals dealing with psychological ill-health and satisfaction with care. Patient satisfaction with care was assessed in three ways: patients were asked if they desired more time to discuss their problems with their doctor, and more explanation of their care; finally, overall satisfaction with care measured using a five-point Likert scale devised for the study. Information on coping skills was assessed using a checklist relating to the use of exercise, relaxation, or keeping a diary of symptoms. Patients also completed the short form of the general health questionnaire (GHQ-12). As well as the English version, the questionnaire was translated into the main languages used by patients: Vietnamese, Chinese, Spanish, and Arabic.
Patients returned the questionnaire to their GP who completed the final page during the consultation. This section sought information on whether the GP had treated the patient for anxiety and depression during the previous 12 months, what treatment if any had been prescribed for symptoms, and what referrals to or communication from other health professionals had resulted.
During this study, three methods were used to identify patients experiencing symptoms of anxiety and depression: the GHQ-12 (a widely used screening aid for primary care settings) [16,17], a patient self-report checklist of symptoms during the previous 4 weeks for which they sought medical care, and a GP report of whether a diagnosis had been made and/or treatment administered for anxiety and depression during the previous 12 months. Individual items that comprised the GHQ-12 were regarded as positive if either of the most extreme two categories for that item were endorsed. The number of positive items were summed to give an individual score (range 0–12). An overall score of three or more was used to indicate a ‘case’ of anxiety and/or depression [18,19] although a higher cutoff has been recommended recently by Goldberg [20].
Completed questionnaires were obtained from 4867 patients attending 117 general practices in the Sydney metropolitan area (85% response). The present paper is based on data collected from adults aged 18–64 years (n = 2665) who indicated that they were involuntarily unemployed or employed part- or full-time at the time of study. Patients (n = 2202) who indicated that they were not in the workforce (retired, home duties, students and pensioners) or were not within the eligible age range, were excluded from the analysis. The GHQ-12 was not completed by 157 eligible patients, 54 among these who were unemployed and 103 among the employed. These patients were excluded from the regression analyses.
Analysis
Date analysis was completed using the Statistical Package for the Social Sciences (
Multivariate logistic regression analysis was used to examine the association of employment status and occurrence or treatment of anxiety and depression when the effect of the covariates (age, sex, non-English speaking country of birth (NESB) and symptom severity as indicated by the GHQ-12 score) was controlled in the model. Age was stratified for the purposes of these analyses as follows: 18–29 years, 30–49 years and 50–64 years. The estimates of the logistic regression coefficients were derived from an iterative maximum likelihood method using
Results
There were 2665 patients aged 18–64 years who met the criteria for inclusion in this study. Of these, 392 patients indicated they they were unemployed and 2273 indicated that they were employed either part-time or full-time. The mean age of unemployed patients was 36.2 (±12.3) years and was slightly lower than that of employed patients (37.5, ± 11.6 years) t = 2.0, df = 2663, p = 0.4). The distribution of males (45%) and females (55%) was similar for both groups. A greater proportion of unemployed patients (43.8%; 95% CI = 38.8–49.0%) were from a non-English speaking background (NESB) than employed patients (23.1%; 95% CI = 21.4–24.9%, χ2 = 72.8, df = 1, p = 0.001) and spoke a language other than English at home (41.3%; 95% CI = 36.0–46.8% compared with 25.9%, 95% CI = 24.0–27.8%, χ2 = 33.9, df = 1, p = 0.001). Most patients (overall 81.4%; 95% CI = 79.9–82.9%), in both groups, were attending their usual GP.
Identification of anxiety and depression
The results of the GHQ-12 screen indicated that anxiety and depression were significantly more prevalent in the unemployed patients than in the employed patients and that the symptoms may be more severe. The mean GHQ-12 score was 3.8 for unemployed patients and 2.4 for employed patients (mean difference = 1.4, 95% CI(difference) = 1.0–1.7, t = 7.33, df = 2506, p < 0.001). Patients who reported unemployment were significantly more likely to have a GHQ-12 score of 3 or more (50.9%; 95% CI = 45.3–56.2% for unemployed and 34.7%; 95% CI = 32.7–36.7% for employed; χ2 = 33.1, df = 1, p < 0.001) and a GHQ-12 score of 4 or more (40.5%; 95% CI = 35.3–46.0% for unemployed and 27.1%; 95% CI = 25.2–29.0% for employed; χ2 = 25.9, df = 1, p < 0.001). When the effects of the covariates (age, sex, and NESB) were controlled using logistic regression, unemployed patients were twice as likely to have a positive GHQ-12 score as employed patients (odds ratio = 2.0, 95% CI = 1.5–2.7 for 3 or more and odds ratio = 1.9, 95% CI = 1.5–2.4 for 4 or more).
Anxiety and depressive symptoms based on the patient self-report checklist (worry, nerves, stress, anxiety, depression, and sleep problems) that required medical treatment during the previous 4 weeks were reported by 453 patients. Unemployed patients (30.9%) were twice as likely as employed patients (14.6%) to report such symptoms (Table 1). As there was an association between patient self-report of symptoms and age and there was association between NESB and unemployment, a logistic regression model was developed to control for the effect of these variables. The results showed that unemployed patients were 2.7 times (95% CI = 2.1–3.6) more likely than employed patients to self-report any of the symptoms of anxiety and depression that required treatment during the previous 4 weeks (χ2 = 59.6, df = 1, p < 0.001). Unemployed patients (82.6%; 95% CI = 74.5–88.7%) were also more likely, compared with employed patients (71.4%; 95% CI = 66.1–76.1%) to have experienced the identified symptoms for more than 4 weeks (χ2 = 5.9, df = 1, p = 0.02).
Influence of unemployment on patient self-report of symptoms of anxiety and depression within the last 4 weeks
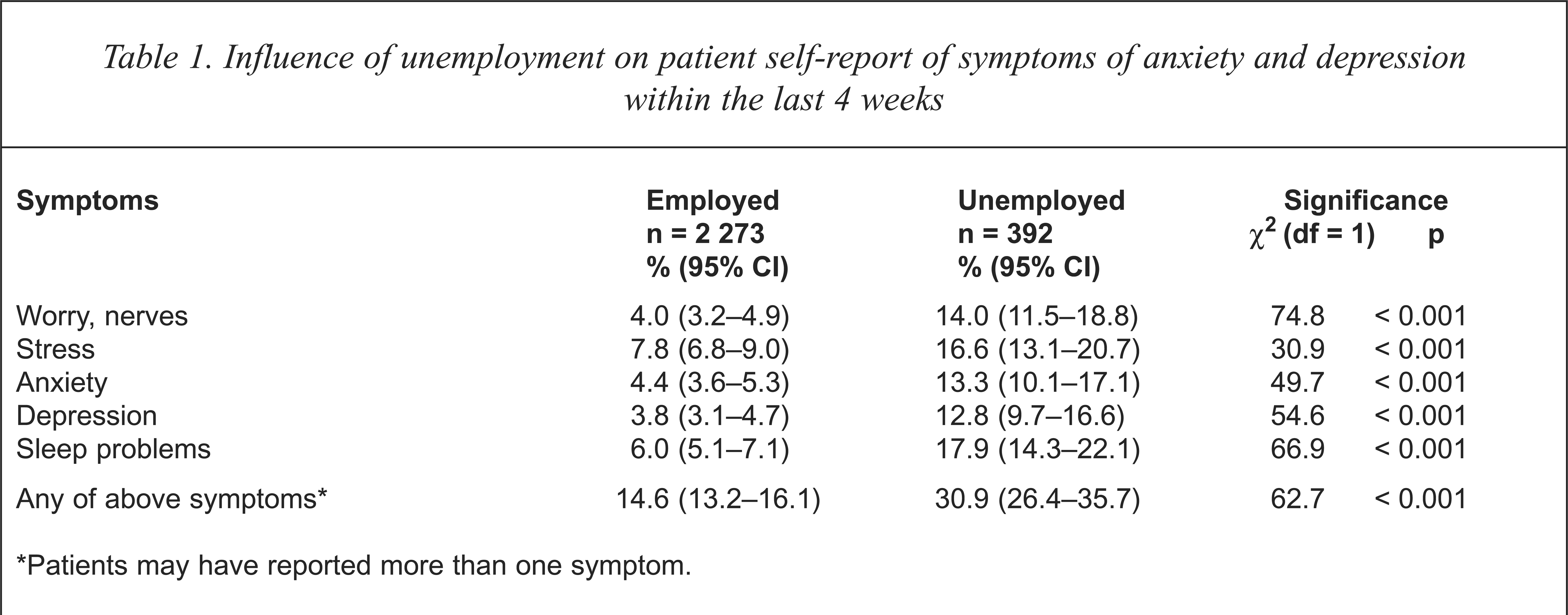
Patients may have reported more than one symptom.
GPs indicated that they had treated 465 patients (17.4% of the total sample) for symptoms of anxiety and depression during the previous 12 months. According to their report, unemployed patients (27.8%) were nearly twice as likely to have been diagnosed and treated than were employed patients (15.7%; 95% CI = 14.2–17.2%, χ2 = 34.2, df = 1, p < 0.001). Using the logistic regression model to control for age, sex, and NESB, unemployed patients were 2.39 times (95% CI = 1.8–3.1, χ2 = 43.6, df = 1, p < 0.001) more likely to have been treated for anxiety and depression by their GP during the previous 12 months compared to employed patients.
Treatment of unemployed GP patients
For the 465 patients whom the GP reported treating for anxiety and depression during the last 12 months, GPs were nearly twice as likely to report that medication had been prescribed for anxiety and depressive symptoms among unemployed patients compared with employed patients (Table 2). These trends were observed for the prescription of anti-anxiety drugs, antidepressant drugs and sleeping medications. Next, a logistic regression model was applied to control for the potential confounding factors identified above, and symptom severity as measured using the GHQ-12. Compared with employed patients unemployed patients were three times (95% CI = 1.9–4.8%) as likely to be prescribed medication when the influence of age, sex, and NESB was controlled. This association was not influenced by the additional inclusion as a covariate of the GHQ-12 score (Table 2). The findings held for each of the three groups of medication for which information was sought (anti-anxiety, antidepressant and sleeping medication).
General practitioner prescription of psychotropic medication for unemployed patients who were treated by GPs within the last 12 months
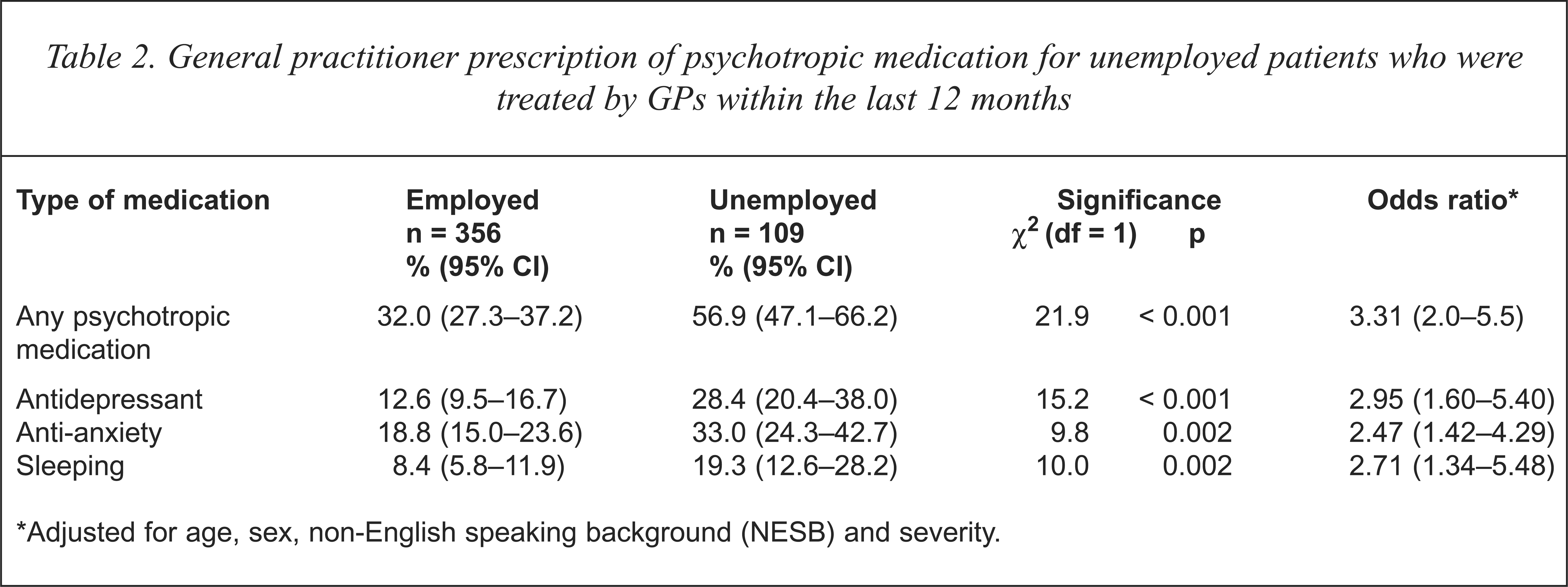
Adjusted for age, sex, non-English speaking background (NESB) and severity.
Employment status of patients who were treated by GPs did not influence patterns of referral to other professional services. While GPs referred their patients with anxiety and/or depression to a variety of other health professionals (Table 3), there were no differences between unemployed and employed patients in the proportion referred (27.5%; 95% CI = 19.6–37.0% of unemployed compared with 25.3%; 95% CI = 20.9–30.2% of employed; χ2 = 0.2, df = 1, p = 0.6) or in number of contacts from other services with the GP about the patient (11.9%; 95% CI = 6.8–19.9% of unemployed and 13.8%; 95% CI = 10.4–17.9% of employed; χ2 = 2.4, df = 1, p = 0.6). GPs were significantly less likely, however, to refer unemployed patients with anxiety and depression to self-help groups compared to employed patients (Table 3).
Use of other health professional services by unemployed patients comparing the group who self-reported symptoms with the group who were detected and treated by general practitioners
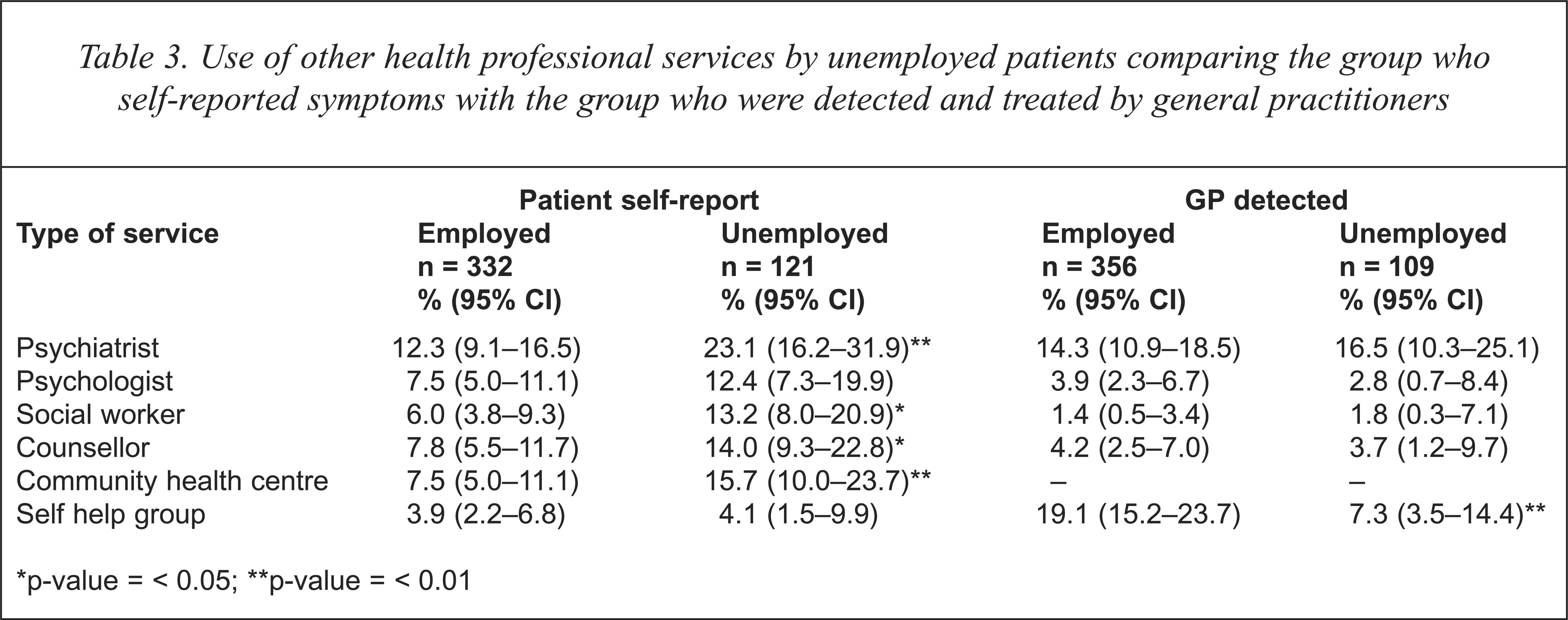
p-value = < 0.05;
p-value = < 0.01
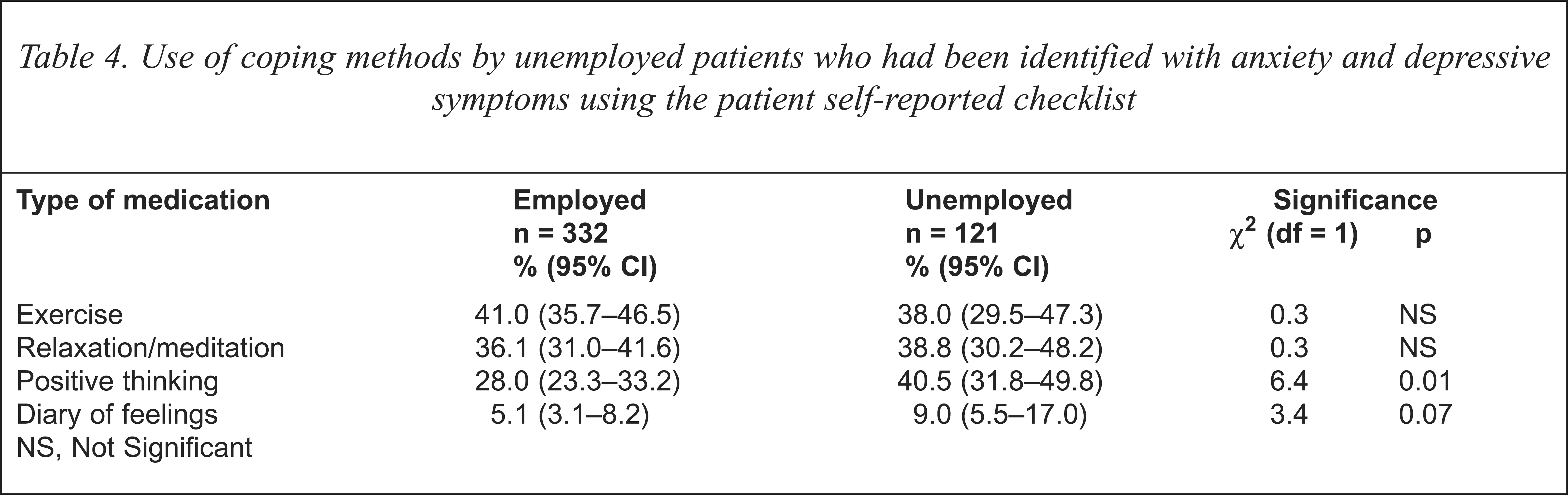
Of the 453 patients with anxiety and depression using the patient self-report checklist, unemployed patients were more likely to report that their doctor was the main health professional treating their symptoms (74.4%; 95% CI = 65.5–81.7% compared with 63.0%; 95% CI = 57.7–68.1%; χ2 = 5.2, df = 1, p < 0.05). Unemployed patients were also significantly more likely to report that they had seen another health professional for their symptoms than employed patients (Table 3). Unemployed patients who reported symptoms of anxiety and depression were comparable to employed patients in their use of simple coping methods listed in the questionnaire (exercise, relaxation or keeping a diary) but were more likely to report using positive thinking (Table 4). Unemployed patients who reported symptoms were significantly more likely to report use of medication (51.2%; 95% CI = 42.0–60.4%) compared with the employed (36.4%; 95% CI = 31.3–41.9%; χ2 = 8.1, df = 1, p < 0.01).
Use of coping methods by unemployed patients who had been identified with anxiety and depressive symptoms using the patient self-reported checklist
Unemployed patients identified using the self-report checklist indicated that they were less content with treatment for symptoms than were employed people with symptoms. The unemployed expressed a desire to spend more time discussing their emotional problems with their doctor (34.7%; 95% CI = 56.0–73.6% compared with 19.3%; 95% CI = 15.3–24.0%, χ2 = 11.8, df = 1, p < 0.001) and wished for more explanation about medications that were prescribed (31.4%; 95% CI = 23.4–40.6% compared with 21.1%; 95% CI = 16.9–26.0%, χ2 = 5.2, df = 1, p = 0.02). However, there was no significant difference between unemployed and employed patients in their responses to the perceived helpfulness of the advice and treatment they had received (67.8%; 95% CI = 58.6–75.8% unemployed compared with 59.6%; 95% CI = 54.1–64.9% employed, χ2 = 2.5, df = 1, p = 0.1).
Discussion
The study demonstrates that there is a strong association between unemployment and the occurrence of symptoms of anxiety and depression measured by GHQ, patient self-report using a checklist and by GP detection. In addition, patients who were unemployed were significantly more likely to receive medication from their GP but no more likely to be referred to other health professionals.
The demographic characteristics of the unemployed patients differed from those of employed patients. The increased proportion of NESB patients and the younger age among those patients who were unemployed is consistent with the patterns of unemployment that occur in the communities where the survey was conducted [14]. Thus adjustment was made for age, sex and non-English speaking background in the relevant analyses.
The data on the presence of anxiety and depressive symptoms collected during this study were derived from patient self-reports, patients' GPs and a short form of the General Health Questionnaire (GHQ-12). There was no attempt at independent verification of these measures using, for example, independent interviews by psychiatrists. Notwithstanding that limitation, there was convergence in the finding: GHQ score using varying cut-offs, patient self-report and GP detection all suggested an association of increased anxiety and depressive symptoms in the unemployed. This association remained statistically significant when age and birth in a non-English speaking country were controlled for in the analysis.
Unemployed patients who were symptomatic were also significantly more likely to be prescribed psychotropic medication, and this pattern was not accounted for by severity of GHQ-12 scores. This finding provides evidence that GPs may manage unemployed patients differently, that is, unemployed patients who are symptomatic are more likely to be prescribed medication but not more likely to be referred to other health professionals. That these differences in management were based on the GP's perception of the demands of patients and their capacity to participate in other management strategies (such as stress management programs) was supported by the results of an associated study [15]. Several doctors participating in focus groups reported that they prescribed drugs more often for patients who were unemployed. Their reasons for so doing included differential levels of demand by the patients for medicatioin and a sense that many unemployed patients did not have the financial, social or personal resources to cope with more active management strategies.
In the present study unemployed patients who self-reported symptoms using the checklist were more likely to express dissatisfaction with aspects of their treatment. Specifically, they expressed a desire for more time to discuss their emotional problems with their GP and for more extensive explanation about medications that were prescribed. This could mean that there is a mismatch between the GP and the patient in perceptions and expectations; GPs feeling that the unemployed patients expect medication, whereas unemployed patients desire a better understanding of how and why medications might be useful; and GPs feeling that patients lack the resources to deal with their problems, and patients wanting more time to examine their emotional problems with their GPs. Unemployed patients were also more likely to report the use of positive thinking which suggests that they may be accepting of non-drug solutions to their difficulties. However, it may be that many GPs feel that they do not have the time or skills to deal with the problems presented by unemployment, an issue that GPs may regard as essentially a social rather than a medical problem. Despite these discrete areas of dissatisfaction with their care, unemployed patients were as likely as employed patients to find the management offered by their doctor useful.
A possible mismatch of perceptions/expectations again appears to be highlighted in the observed referral patterns to other services. GPs reported no difference in their referral patterns for employed and unemployed patients to other services, but the unemployed patients reported a significant excess in use of services compared to employed patients. Unemployed patients reported using community health services, psychiatrists, psychologists, social workers and counsellors more than employed patients, a rate of use that was greater than referral levels reported by GPs. GPs referred both employed and unemployed patients primarily to psychiatrists and were more likely to refer employed rather than unemployed people to self-help groups (Table 2). Unemployed people therefore may be finding their way to these other services through means other than through their usual GP. This is despite the fact that most unemployed patients saw their GP as the manager of their care and were attending their regular doctor at the time of the study. This aspect of the study would benefit from further exploration.
The results of this study have some important implications for general practice. Unemployed patients should be seen as a high-risk group for anxiety and depressive symptoms, and symptoms of mood disturbance should be routinely screened for in consultations with unemployed patients. GPs should reflect more critically on their motivation for prescribing medication to people who are unemployed. Does such management reflect the severity of the condition, or, alternatively, the attitudes/perceptions they, or their patients have, about treatment? There may be a need for GPs to take a more active role in assisting their unemployed patients to deal with their emotional problems in ways other than drug therapy; this may be by the GP being more involved in problem-solving strategies with their patients or through appropriate referral.
If GPs are perceived by the unemployed patient as the health professional primarily responsible for the management of their symptoms, and the role of the principal caregiver is accepted by the GP, there needs to be better understanding by the GP of other services that are useful to patients whose psychological difficulties are associated with unemployment. The level of anxiety and depressive symptoms experienced by people who are unemployed may, over time, act as a barrier to re-employment. The GP has a crucial role in managing these and other conditions in ways that create pathways back to employment, rather than to further marginalisation from the workforce.
Acknowledgments
This study was funded by a grant from the General Practice Evaluation Program of the Commonwealth Department of Human Services and Health. We would like to thank the South-west and South-east Divisions of General Practice in Sydney and the GPs who participated in the study. We would also like to recognise the contribution of Eva Kehag, Alex Barratt, Jocelyn Pan, John Frith, Alex Blaszczynski and Dimity Pond to the design and implementation of the study.