
Abstract
Objective:
There have been debates about the linkages between abortion and mental health. Few reviews have considered the extent to which abortion has therapeutic benefits that mitigate the mental health risks of abortion. The aim of this review was to conduct a re-appraisal of the evidence to examine the research hypothesis that abortion reduces rates of mental health problems in women having unwanted or unintended pregnancy.
Methods:
Analysis of recent reviews (Coleman, 2011; National Collaborating Centre for Mental Health, 2011) identified eight publications reporting 14 adjusted odds ratios (AORs) spanning five outcome domains: anxiety; depression; alcohol misuse; illicit drug use/misuse; and suicidal behaviour. For each outcome, pooled AORs were estimated using a random-effects model.
Results:
There was consistent evidence to show that abortion was not associated with a reduction in rates of mental health problems (p>0.75). Abortion was associated with small to moderate increases in risks of anxiety (AOR 1.28, 95% CI 0.97−1.70; p<0.08), alcohol misuse (AOR 2.34, 95% CI 1.05−5.21; p<0.05), illicit drug use/misuse (AOR 3.91, 95% CI 1.13−13.55; p<0.05), and suicidal behaviour (AOR 1.69, 95% CI 1.12−2.54; p<0.01).
Conclusions:
There is no available evidence to suggest that abortion has therapeutic effects in reducing the mental health risks of unwanted or unintended pregnancy. There is suggestive evidence that abortion may be associated with small to moderate increases in risks of some mental health problems.
Keywords
Introduction
Recently there have been strong debates about the relationships between termination of pregnancy (abortion) and mental health (for reviews, see Bradshaw and Slade, 2003; Charles et al., 2008; Coleman, 2005, 2011; American Psychological Association, 2008). These debates have been stimulated by two major reviews of this topic which reached markedly different conclusions. Specifically, in a meta-analysis of 22 studies examining the linkages between abortion and mental health, Coleman (2011) found that abortion was associated with increased risks of mental health problems with these findings being evident for studies using different comparison groups. Coleman concluded “… the results revealed a moderate to highly increased risk of mental health problems after abortion” (p. 180). In contrast, a systematic review of the evidence prepared for the Academy of Medical Royal Colleges (AMRC) by the National Collaborating Centre for Mental Health (2011) concluded that, when variations in study design and study quality were taken into account, “The rates of mental health problems for women with unwanted pregnancy were the same whether they had an abortion or gave birth” (p. 8).
Following the publication of both reviews, there have been extensive criticisms of both Coleman’s study (Abel et al., 2011; Coyne, 2011; Howard et al., 2011; Kinney, 2011; Lagro-Janssen et al., 2011; Littell and Coyne, 2011; Polis et al., 2011; Robinson et al., 2011; Thygesen, 2011) and the AMRC report (Andrusko, 2011; Christian Medical Fellowship, 2011; Ertelt, 2011). Despite the apparently contradictory findings of these reviews both appear to be in agreement on one point: there is no evidence to suggest that the provision of abortion mitigates the mental health effects of unwanted pregnancy. The AMRC review concludes that there were little if any effects of abortion on mental health, whereas the Coleman analysis suggests that abortion may have harmful effects on mental health.
However, both studies fail to provide a formal review of the therapeutic benefits of abortion. More generally, there has been a dearth of discussion about the mental health benefits of abortion in all existing major reviews, including the 2008 review by the American Psychological Association (2008) and the review by Charles et al. (2008). In all cases, reviews have focussed on the issue of the extent to which abortion has iatrogenic effects which result in increases in mental health problems in women having abortion when compared with equivalent groups of women coming to term with an unwanted or unintended pregnancy.
However, addressing the issue of whether abortion has beneficial consequences for the mental health of women having unwanted or unintended pregnancy is central to the appraisal of both clinical practice and the interpretation of the law in those jurisdictions which require that access to legal abortion is authorized by registered medical practitioners. These jurisdictions include England, Wales, Scotland, and New Zealand (1967;, 1977) and some states of Australia (Cica, 1998). Legislation was passed in the 1960s and 1970s in these jurisdictions which gave women access to legal abortion provided that the abortion was authorized by two medical practitioners on medical grounds. In these societies over 90% of all abortions are currently authorized on the grounds that continuation of the pregnancy would pose a serious threat to the woman’s mental health (Statistics New Zealand, 2003; South Australian Abortion Reporting Committee, 2008; Department of Health, 2011). Given the high frequency with which mental health grounds are used in these jurisdictions to authorize abortion, it becomes important for both clinical and legislative reasons to examine the evidence on the extent to which abortion has therapeutic benefits that mitigate any mental health effects of unwanted pregnancy.
Under ideal circumstances it would be desirable to examine this issue using randomized controlled trials of the effectiveness of abortion in mitigating any adverse mental health effects of unwanted pregnancy. However, such trials are currently ethically and practically impossible to conduct. Under these circumstances, data from observational studies may be used to examine this hypothesis. In particular, if abortion has the therapeutic benefits that have been ascribed to the practice, one would expect to find that rates of mental health problems amongst those having abortion were lower than those in an equivalent series of women coming to term with unwanted or unintended pregnancy.
In this paper we present a re-analysis and re-appraisal of data from 14 analyses reviewed by the Coleman review, the AMRC review, or both. In these analyses, the mental health outcomes of women having abortion were compared to control series of women having unwanted or unintended pregnancy coming to term, with these comparisons being controlled for a number of potentially confounding covariates. The 14 analyses examined five mental health outcomes: anxiety, depression, alcohol misuse, illicit drug use/misuse, and suicidal behaviour. The re-analysis and re-appraisal of these findings has the explicit aim of addressing the question of whether this research provides any evidence that would support the conclusion that abortion has beneficial consequences which mitigate the mental health risks of unwanted or unintended pregnancy.
Methods
Data extraction
The studies examined in this re-appraisal of the evidence are based on a series of analyses included in the reviews by Coleman (2011) and the AMRC (National Collaborating Centre for Mental Health, 2011). These were all studies in which comparisons were made between a group of women exposed to abortion and a control series of women coming to term with unintended/unwanted pregnancy. This process identified a series of 14 analyses based on four studies and summarized in eight publications, with these studies examining five mental health outcomes: anxiety, depression, alcohol misuse, illicit drug use/misuse, and suicidal behaviour. Table 1 provides a summary and overview of the eight publications upon which this re-appraisal of the evidence is based. This summary includes information on sample sizes, the assessment of the control group, outcomes measured, control factors employed in each study, and assessment of study quality.
Description of studies.
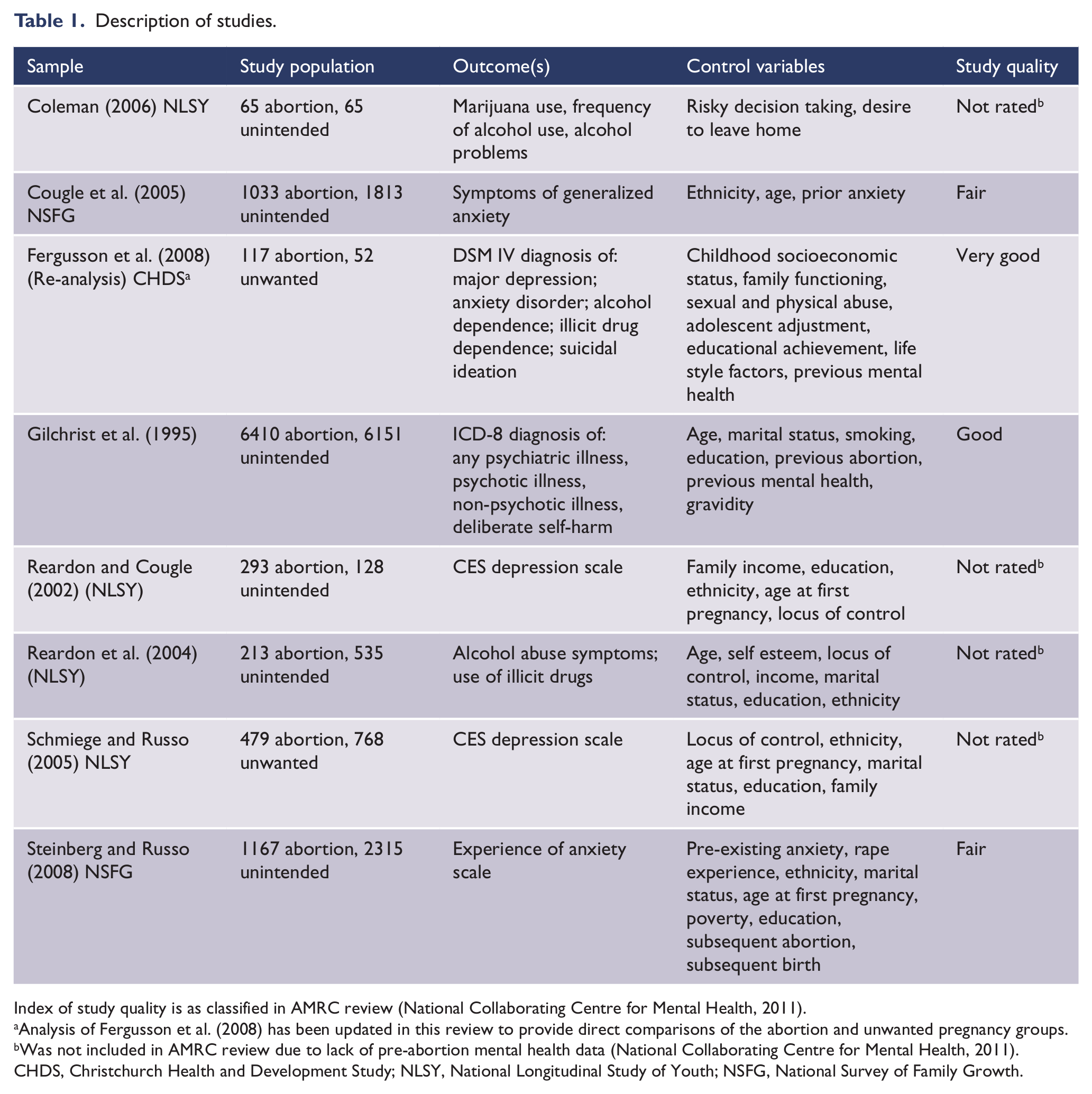
Index of study quality is as classified in AMRC review (National Collaborating Centre for Mental Health, 2011).
Analysis of Fergusson et al. (2008) has been updated in this review to provide direct comparisons of the abortion and unwanted pregnancy groups.
Was not included in AMRC review due to lack of pre-abortion mental health data (National Collaborating Centre for Mental Health, 2011).
CHDS, Christchurch Health and Development Study; NLSY, National Longitudinal Study of Youth; NSFG, National Survey of Family Growth.
Of the analyses summarized in Table 1, all were included in the Coleman review (2011) but a number of these publications were not included in the AMRC review (National Collaborating Centre for Mental Health, 2011). These publications were Reardon and Cougle (2002), Reardon et al. (2004), Schmiege and Russo (2005), and Coleman (2006). The reason for these studies being excluded from the AMRC review was that these studies provided inadequate control of pre-existing mental health outcomes prior to pregnancy. For all studies estimates of adjusted odds ratios (AORs) and 95% confidence intervals were abstracted from the original reviews and cross-checked with the original studies. In all cases, AORs were scored so that an AOR <1 implied that rates of mental health problems were lower in those having an abortion. The Fergusson et al. (2008) data were re-analysed to produce estimates of the AORs for the direct comparison between the unwanted pregnancy and abortion groups after adjustment for covariates.
Assessment of study quality
Table 1 also includes assessments of study quality derived from the ratings given in Table 18 in the AMRC review. These ratings were based on a modified version of the review criteria used by Charles et al. (2008). These criteria considered six study features: appropriate comparison group, validated mental health tools, previous mental health problems, confounder control, sample representativeness, and comprehensive data exploration. These criteria were used to rank studies into six quality groups ranging from “very poor” to “excellent”. Of the studies subject to this review, one (Fergusson et al., 2008) was described as “very good”, one (Gilchrist et al., 1995) was described as “good”, two studies (Cougle et al., 2005; Steinberg and Russo, 2008) were classified as “fair”, and four were not included in the AMRC review because of concerns about study quality.
Data analysis and hypothesis testing
The analyses from the studies described in Table 1 were classified into five outcome domains: anxiety, depression, alcohol misuse, illicit drug use/misuse, and suicidal behaviours. Each domain contained at least two odds ratios from independent analyses. To increase the precision of the re-appraisal, pooled odds were estimated for each domain. In this analysis, we have not combined the pooled estimates for different outcomes to produce an estimate of the overall increase or decrease in mental health problems for women having abortion. The principal reason for this decision was that the data came from overlapping and non-independent analyses using data derived from four studies. The non-independence of the pooled estimates poses complex problems for combining these estimates to produce an estimate of the overall association between abortion and mental health outcomes.
The selected ORs for each outcome domain were first log transformed and then pooled using a weighted average of the study specific effects. Pooling was initially conducted using a random-effects model of the form: Pooled B=Σj wj Bj/Σj wj, where Bj=ln(ORj) is the natural logarithm of the OR for study j; wj=1/(sj2+ t2) is a study-specific weight representing the estimated inverse variance of the study specific parameter Bj under a random-effects model; sj2 is the estimated sample specific variance of Bj, and t2 is an estimator of between studies variance derived using the general method of moments (DerSimonian and Kacker, 2007). The standard error of the pooled parameter was given by SE(B)=1/(Σj wj)½. The pooled OR and corresponding 95% CI were calculated in the usual manner by exponentiation, exp(B±1.96 SE(B)). To avoid the pooling of non-independent results in the situation where two studies in a given outcome domain reported AORs based on analysis of essentially the same data set, the pooled results were calculated using only the study reporting the lowest AOR. This follows the practice in the AMRC review (National Collaborating Centre for Mental Health, 2011).
The meta-analysis for each domain was checked for between study heterogeneity using Cochran’s Q test (Huedo-Medina et al., 2006). In all cases there was no evidence of significant between study heterogeneity, suggesting that fixed-effects models were adequate for pooling the data. However, because the Q test can lack statistical power to detect true between-study heterogeneity when the meta-analysis includes only a small number of studies (Huedo-Medina et al., 2006), the reported findings were based on the random-effects analyses. Comparison of pooled estimates from fixed-effects and random-effects models showed these to be very similar suggesting that the choice of estimation method was not critical.
To test for beneficial effects of abortion, in all cases one-tailed tests of the research hypothesis AORi <1 were conducted, where AORi is the pooled odds ratio for the ith outcome domain. For completeness, the analysis also included the results of conventional two-tailed tests of significance of the pooled AORi.
To ensure a complete coverage of the limited literature on this topic, in the first stage of the analysis, all studies were considered in the review (Table 1). To control for study quality, the data were re-analysed using: (a) all studies rated fair or better by the AMRC review; and (b) those studies rated as good or very good by the AMRC review (National Collaborating Centre for Mental Health, 2011).
Results
AORs for the linkages between abortion and mental health outcomes
Table 2 shows estimates of the AORs between abortion and the mental health outcomes reported in eight papers based on four studies. Results are grouped into five outcome domains and for each domain an estimate of the pooled AOR and confidence interval is given. The table reports the probability level associated with the test of the one-tailed hypothesis AOR <1 (p1) and the conventional two-tailed test of association (p2). Inspection of Table 2 yields the following conclusions:
Odds ratios and pooled odds ratios for the association between abortion and mental health.
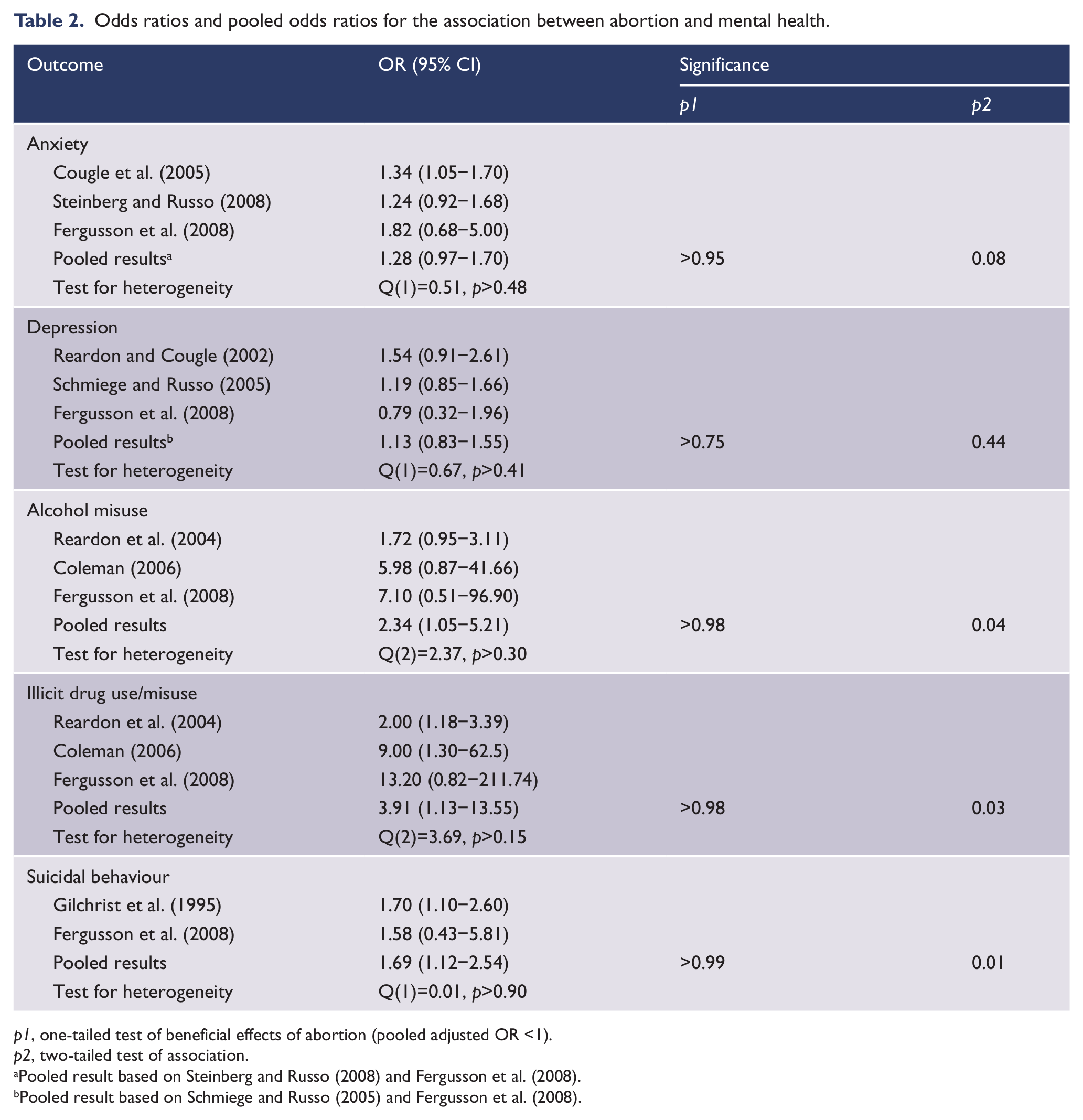
p1, one-tailed test of beneficial effects of abortion (pooled adjusted OR <1).
p2, two-tailed test of association.
Pooled result based on Steinberg and Russo (2008) and Fergusson et al. (2008). bPooled result based on Schmiege and Russo (2005) and Fergusson et al. (2008).
Anxiety: Three studies report estimates of association between abortion and anxiety, with two studies (Cougle et al., 2005; Steinberg and Russo, 2008) being analyses of the same data. Observed AORs ranged from 1.24 to 1.82, with the pooled AOR being 1.28 (95% CI 0.97−1.70; p2<0.10). The one-tailed test of the hypothesis of beneficial effects of abortion shows that this hypothesis is not supported by the evidence (p1>0.95).
Depression: Three studies report estimates of the association between abortion and depression with two studies being analyses of the same data (Reardon and Cougle, 2002; Schmiege and Russo, 2005). Observed AORs ranged from 0.79 to 1.54, with the pooled AOR being 1.13 (95% CI 0.83−1.55; p2>0.40). The one-tailed test of the hypothesis of beneficial effects of abortion shows that this hypothesis is not supported by the evidence (p1>0.70).
Alcohol misuse: Three studies reported estimates of the association between abortion and alcohol misuse. Observed AORs ranged from 7.10 to 1.72, with the pooled AOR being 2.34 (95% CI 1.05−5.21; p2<0.05). The one-tailed hypothesis of beneficial effects of abortion shows that this hypothesis is not supported by the evidence (p1>0.98).
Illicit drug use/misuse: Three studies report estimates of the association between abortion and illicit drug use/misuse. Observed AORs ranged from 13.20 to 2.00, with the pooled AOR being 3.91 (95% CI 1.13−13.55; p2<0.05). The one-tailed test of beneficial effects of abortion shows that this hypothesis is not supported by the evidence (p1>0.98).
Suicidal behaviour: Two studies report estimates of the association between abortion and suicidal behaviour. Observed AORs ranged from 1.58 to 1.70, with the pooled AOR being 1.69 (95% CI 1.12−2.54; p2<0.01). The one-tailed test of beneficial effects of abortion shows that this hypothesis is not supported by the evidence (p1>0.99).
The effects of study quality on conclusions
To examine the extent to which variations in study quality led to changes in the conclusions drawn above, a number of re-analyses of the data in Table 2 were conducted. These re-analyses included:
Limiting the analysis to studies included in the AMRC review. This resulted in the exclusion of the studies based on the NLSY (Reardon and Cougle, 2002; Reardon et al., 2004; Schmiege and Russo, 2005; Coleman, 2006). This reduced the analysis to pooled AORs for two outcome domains (anxiety and suicidal behaviour). This analysis shows:
For both outcome domains, one-tailed tests showed an absence of beneficial effects of abortion (all p1>0.95).
Pooled AORs showed marginally significant increases in rates of anxiety (AOR 1.28, 95% CI 0.97−1.70, p2<0.10) and significant increases in suicidal behaviour (AOR 1.69, 95% CI 1.12−2.54, p2<0.01) for women having abortion.
The analysis was then restricted to the studies rated as good or very good in the AMRC report (National Collaborating Centre for Mental Health, 2011). These studies reported a single common outcome of suicidal behaviour, with a pooled AOR of 1.69 (95% CI 1.12−2.54; p1>0.99; p2<0.01). This finding does not support the hypothesis of beneficial effects (p>0.99) but is consistent with the conclusion that abortion may be associated with modest increases in risks of suicidal behaviours.
Finally, the AMRC review (National Collaborating Centre for Mental Health, 2011) also reported a re-analysis of the Gilchrist et al. (1995) study in which they compared the outcomes of those refused abortion for an unwanted pregnancy with the outcomes of those given an abortion. These estimates were available for suicidal behaviours. Combining these results with the findings from Fergusson et al. (2008) yielded an AOR of 0.95 (95% CI 0.36−2.51). The one-tailed test of the positive effects of abortion was non-significant (p>0.90).
Summary
For all analyses considered, there was no evidence to suggest that rates of mental health problems were lower in women having abortion than in comparison groups of women having unwanted pregnancy. This conclusion held for all studies, all authors, and all outcomes considered, irrespective of variations in study quality using the standards applied in the AMRC review (National Collaborating Centre for Mental Health, 2011).
There was suggestive but not completely consistent evidence of modestly elevated rates of mental health problems in women having abortion compared with women having unwanted or unintended pregnancy. These findings were particularly evident for alcohol and illicit drug use but were also evident for anxiety disorders and suicidal behaviours for analyses using an unwanted or unintended comparison. These findings were not observed in AMRC analyses (National Collaborating Centre for Mental Health, 2011) which used those who were refused abortion in the Gilchrist et al. (1995) study as a comparison group.
Discussion
In this paper, we have conducted a re-appraisal of the evidence reported in the Coleman (2011) and AMRC (National Collaborating Centre for Mental Health, 2011) reviews. The focus of this assessment was upon examining the extent to which abortion had beneficial outcomes by reducing the mental health risks of unwanted or unintended pregnancy. This analysis focussed on five outcome domains using data from 14 analyses, reported in eight publications based on four studies. The principal finding of this analysis was that there was no evidence for any outcome domain that the provision of abortion was associated with significant reductions in mental health risks. This conclusion held when the data were re-analysed to take into account measures of study quality. The findings are also consistent with all major reviews of this topic that have concluded either that: abortion is unrelated to mental health outcomes (Charles et al., 2008; American Psychological Association, 2008; National Collaborating Centre for Mental Health, 2011) or is associated with increases in risks of mental health problems (Coleman, 2005, 2011). No review has concluded that abortion has beneficial consequences by mitigating the mental health risks of unwanted pregnancy. A recent study by Munk-Olsen and colleagues (2011) concluded that the relative risks of mental disorders amongst those having an abortion were similar before and after abortion while risks of mental disorders increased in those having first births. However, this study did not directly compare the mental health risks of those having abortion with an equivalent group of women coming to term with unwanted or unintended pregnancy. To date, there is no direct evidence showing that women having abortion are at lower risk of mental health problems than equivalent groups of women coming to term with unwanted or unplanned pregnancy.
Because of the highly controversial nature of this topic, it is useful to consider a number of possible limitations of the study and responses to these.
It could be suggested that the paper lacks novelty and is largely a restatement of what is already known. It is correct that the statistical review in Table 2 is not original and is a restatement of evidence previously reviewed. However, the originality of the paper lies with the process of linking this research evidence to an important research question regarding the mental health benefits of abortion. This research question has substantial policy and clinical significance but has been given limited attention in the existing literature.
It may also be suggested that the studies reviewed contain multiple problems research design, analysis and interpretation that prevent any clear conclusions from being drawn. In comparison to the ideal of testing the mental benefits of abortion using a randomized controlled trial, it is clear that existing observational studies provide only limited and potentially flawed evidence on the mental health consequences of abortion. However, this observation does not impugn the validity of the conclusion that: at the present time there is no credible scientific evidence demonstrating that abortion has mental health benefits.
In addition, it could be suggested that the comparisons made in the study between those having abortion and those having unwanted or unintended pregnancy do not provide an appropriate test of the mental health effects of abortion. A better comparison would be between those having abortion and those refused abortion. In addressing the research question, we have taken the approach used by the majority of the reviews of the mental health consequences of abortion (Bradshaw and Slade, 2003; Charles et al., 2008; American Psychological Association, 2008; National Collaborating Centre for Mental Health, 2011) by comparing those having abortion with those coming to term with unwanted or unintended pregnancy. Further, to our knowledge, the only study that has compared those having abortion with those refused abortion is the re-analysis of Gilchrist et al. (1995), conducted by the AMRC review. This re-analysis found that, for a number of outcomes (psychotic illness, non-psychotic illness, self harm), those refused abortion fared worse than those provided with abortion, with this difference being statistically significant (p<0.01) for psychotic illness. This evidence suggests the possibility that further studies making such comparisons could demonstrate positive benefits for abortion. However, at the present time the evidence is far too limited to conclude that abortion reduces any mental health risks of unwanted or unintended pregnancy.
Finally, it may also be suggested that the integrity of the review is compromised by the inclusion of studies from authors well known for their pro-life views. Given the relatively small number of studies in this area and the controversial nature of the area, it was our view that the most even-handed approach to reviewing the evidence was to include all studies comparing the mental health outcomes of those having abortion with comparison series of women coming to term with unwanted or unintended pregnancy. Further, it is clearly demonstrable that the study conclusions regarding the absence of benefit of abortion are not influenced by study selection factors. Specifically, irrespective of ratings of study quality, the data in Table 2 show that there is no evidence of beneficial consequences of abortion for: all studies; all authors and all outcomes. Of the 14 ORs reported in Table 2, 13 are greater than 1 and in all cases the one-tailed hypothesis of beneficial consequences of abortion is strongly rejected. Whether or not certain studies are included or excluded from the review does not change these conclusions.
In summary, while there may be grounds for concern that the evidence reviewed does not adequately test the research hypothesis, these problems of evidence quality do not impugn the validity of the main study conclusion that at the present time there is no credible evidence to support the research hypothesis that abortion reduces any mental health risks associated with unwanted or unplanned pregnancy that come to term. This situation may reflect the fact that existing studies have not adequately tested the hypothesis, or that the hypothesis is not correct, or both.
These conclusions have important, if uncomfortable, implications for clinical practice and the interpretation of the law in those jurisdictions (England, Wales, Scotland, Australia, New Zealand) which require abortion to be authorized on medical grounds. In these jurisdictions, the great majority of abortions are authorized on mental health grounds (Statistics New Zealand, 2003; South Australian Abortion Reporting Committee, 2008; Department of Health, 2011). The present re-analysis suggests that, currently, there is no evidence that would support this practice. While it remains possible that abortion may mitigate any adverse effects of unwanted or unintended pregnancies, the available evidence does not support this conclusion.
In turn, this conclusion suggests an urgent need to revisit both clinical practice and the law in those jurisdictions in which mental health grounds are the principal criteria for recommending and authorizing abortion. The history of abortion law and law reforms shows that this is likely to resurrect politically uncomfortable and socially divisive debates about access to legal abortion (Cica, 1998; Abortion Rights, 2003; Abortion Law Reform Association of New Zealand, 2011). It is probably awareness of these consequences that explains the almost complete lack of discussion of the evidence for therapeutic benefits of abortion in recent reviews of abortion and mental health. However, it is our view that the growing evidence suggesting that abortion does not have therapeutic benefits cannot be ignored indefinitely, and it is unacceptable for clinicians to authorize large numbers of abortions on grounds for which there is, currently, no scientific evidence. On the face of things, the most straightforward way of resolving these tensions between the law and clinical practice in jurisdictions that use health criteria as grounds for authorizing abortion is to extend these criteria to include serious threats to the social, educational, or economic wellbeing of the woman and her immediate family as legitimate grounds for authorizing abortion. This revision would more closely align the criteria for authorizing abortion with the multiple personal reasons (Broen et al., 2005; Finer et al., 2005) for which women seek abortion.
It could be argued that the lack of evidence of mental health benefits for abortion may be explained by problems of study quality including the selection of comparison groups, the measurement of outcomes, the control of confounding, and related issues (Kendall et al., 2012), as noted in previous reviews including that of the AMRC (National Collaborating Centre for Mental Health, 2011), the APA (American Psychological Association, 2008), and the review by Charles et al. (2008). For example, the majority of studies in this area have used unintended pregnancy for a comparison group. However, by no means all of those having unintended pregnancy will find these pregnancies unwanted. The use of an unintended pregnancy comparison could therefore obscure possible benefits of abortion. Some re-assurance about this matter can be found from the fact that the studies using an unwanted pregnancy comparison group (Schmiege and Russo, 2005; Fergusson et al., 2008) and the studies using unintended comparison groups (Gilchrist et al., 1995; Cougle et al., 2005; Coleman, 2006; Steinberg and Russo, 2008) produced generally similar AOR estimates. In all cases, Q tests found no evidence of significant between study heterogeneity in the AOR estimates.
However, these deficiencies in study design are not sufficient grounds for concluding that abortion has beneficial consequences, although they do suggest the need for further and better research into this topic. One of the interesting findings uncovered by this reappraisal is that all of the analyses which have examined this issue using comparison groups of women who come to term with unwanted or unintended pregnancy have been drawn from four studies, with three of these studies not being explicitly designed to research this topic. It is probably this lack of well-designed research more than anything else that explains the continuing controversies in this area. This situation has led to reviews of this topic drawing strong conclusions about the absence (American Psychological Association, 2008; Charles et al., 2008; National Collaborating Centre for Mental Health, 2011) or presence (Coleman, 2005, 2011) of associations between abortion and mental health using limited data from studies that were not designed to examine this topic.
A further finding of this review was that, contrary to the conclusions drawn in the APA report (American Psychological Association, 2008), the Charles et al. review (2008) and the AMRC review (National Collaborating Centre for Mental Health, 2011), there was suggestive evidence that abortion may be associated with small to moderate increases in risks of mental health problems with these increases being most evident for substance misuse. The exceptions to these findings were for depression and for comparisons involving women refused abortion with those provided with abortion. Because of the limitations of the existing data ( American Psychological Association, 2008; Charles et al., 2008; National Collaborating Centre for Mental Health, 2011; Kendall et al., 2012) and the highly controversial nature of this topic, it would be premature to conclude emphatically that this evidence is sufficient grounds for believing that abortion has adverse effects on mental health. Equally, however, the generally consistent evidence suggesting small to moderate increases in rates of anxiety, substance use problems, and suicidal behaviours does provide sufficient grounds for suggesting that further and better research is needed before strong conclusions can be ventured about this topic. Another area in which there is need for further research concerns the extent to which abortion has benefits for women and their immediate family in other areas of social, educational, and economic wellbeing. This research will be needed to evaluate the extent to which any change to the law along the lines outlined above produces positive outcomes for women seeking abortion.
Footnotes
Funding
This research was funded by grants from the Health Research Council of New Zealand, the National Child Health Research Foundation, the Canterbury Medical Research Foundation and the New Zealand Lottery Grants Board.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.