
Abstract
Objective:
To examine longitudinal associations between mental health and welfare receipt among working-age Australians.
Method:
We analysed 9 years of data from 11,701 respondents (49% men) from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. Mental health was assessed by the mental health subscale from the Short Form 36 questionnaire. Linear mixed models were used to examine the longitudinal associations between mental health and income support adjusting for the effects of demographic and socio-economic factors, physical health, lifestyle behaviours and financial stress. Within-person variation in welfare receipt over time was differentiated from between-person propensity to receive welfare payments. Random effect models tested the effects of income support transitions.
Results:
Socio-demographic and financial variables explained the association between mental health and income support for those receiving student and parenting payments. Overall, recipients of disability, unemployment and mature age payments had poorer mental health regardless of their personal, social and financial circumstances. In addition, those receiving unemployment and disability payments had even poorer mental health at the times that they were receiving income support relative to the times when they were not. The greatest reductions in mental health were associated with transitions to disability payments and parenting payments for single parents.
Conclusions:
The poor mental health of welfare recipients may limit their opportunities to gain work and participate in community life. In part, this seems to reflect their adverse social and personal circumstances. However, there remains evidence of a direct link between welfare receipt and poor mental health that could be due to factors such as welfare stigma or other adverse life events coinciding with welfare receipt for those receiving unemployment or disability payments. Understanding these factors is critical to inform the next stage of welfare reform.
Introduction
Mental health (MH) and well-being is not only a central issue for population health (Jenkins, 2001), but also an important issue to consider when developing and evaluating mainstream social and economic policy (Goldman et al., 2008). For example, MH is a significant barrier to workforce engagement (Butterworth, 2003b; Danziger and Seefeldt, 2003) and it has been well documented that common mental disorders, such as depression and anxiety, are over-represented among welfare recipients relative to the prevalence in the broader community (Butterworth, 2003a; Butterworth, 2003b; Coiro, 2001; Ford et al., 2010). Vulnerability is particularly heightened among single mothers (Butterworth, 2003c) and people who are unemployed or economically inactive (Brown et al., 2012; Kessler et al., 1987a; Kessler et al., 1987b; Rodriguez et al., 2001), such as those unable to work due to disability and sickness (Butterworth et al., 2011a). Understanding the drivers and consequences of poor MH among adults of working age is therefore germane to the design and implementation of effective social security and welfare systems. This is particularly the case for welfare-to-work programmes that promote active workforce participation rather than passive welfare receipt.
The welfare or social security system in Australia is funded directly from general government revenue and provides income support to individuals who lack adequate financial resources. Benefits are tightly targeted at a highly disadvantaged population with strict income and asset tests determining eligibility. Further, uniform payments for all recipients, regardless of their work history or past earnings, makes Australia one of the most redistributive welfare systems in the Organisation for Economic Cooperation and Development (OECD) (Whiteford, 2010). Over the past decade, the welfare system in Australia has undergone considerable reform intended to encourage active workforce participation (Brown, 2011), balancing participation requirements with individual abilities. These reforms have been guided by the principle of mutual obligation (Saunders, 2002) and motivated, in part, by a view that passive welfare receipt fosters a culture of dependency (Mead, 2000) that can erode self-esteem and psychological well-being, and may potentially span generations (McCoull and Pech, 2000). This is also the principle underpinning recent changes to eligibility criteria for parenting payments for single parents (Akerman and Rout, 2013). However, despite a decade of welfare and MH reform during a period of relative economic prosperity within Australia, the MH disparity between income support recipients and non-recipients has remained stable (Butterworth et al., 2011a; Butterworth et al., 2011b).
There are a variety of explanations for the association between MH and income support. MH selection explanations suggest that people with MH problems are at increased risk of welfare dependency, and so welfare receipt may be a consequence of poor MH or mental illness. Alternatively, the association may reflect underlying personal characteristics and social factors that may predispose individuals to increased risk of both poor MH and welfare reliance (Dohrenwend et al., 1992; Kessler et al., 1987a; Kessler et al., 1988; Muntaner et al., 2004). Others have argued that receipt of welfare payments fosters a sense of helplessness and demoralisation, which may be directly responsible for poorer MH (Mead, 2000). Previous cross-sectional studies have demonstrated that the poorer MH of those receiving student, parenting or other miscellaneous payments is explained by socio-demographic variables, physical disability and financial hardship, whereas welfare receipt remained an independent predictor of poorer MH for recipients of disability pensions, unemployment benefits and mature age payments (MAPs) (Butterworth, 2003b; Butterworth et al., 2004). However, as cross- sectional data precludes the modelling of antecedent– consequent relations, the causal pathways between welfare receipt and MH could not be directly established in these studies. Further, cross-sectional data are not able to elucidate the impact of intra-individual variation in welfare receipt on MH, so it is not clear how the relationship between MH and income support changes over time.
Therefore, the purpose of this study was to contrast these explanations by investigating longitudinal associations between MH and welfare receipt in Australia through the analysis of 9 years of follow-up data from a nationally representative household panel survey. We built models with an extensive range of covariates to quantify the extent to which the association between income support receipt and MH reflects confounding or underlying characteristics. For example, the association could reflect a common underlying effect of social disadvantage and limited level of human capital, predisposing individuals to greater risk of both welfare receipt and poor MH (e.g. education, family background, housing tenure and employment). Additionally, the association could reflect personal circumstances and major life events that are strongly related to MH and a basis for eligibility for support payments (e.g. change in marital status and physical limitations). Other confounding factors may not be directly responsible for welfare receipt, but the greater prevalence of these characteristics among welfare recipients and their association with MH may account for the elevated rates of MH problems among welfare recipients (e.g. lifestyle behaviours such as smoking and alcohol consumption). Finally, consistent with current public debate about the adequacy of unemployment payments, the association could directly reflect the contemporaneous economic circumstances of welfare recipients (e.g. financial hardship and household income). A number of the factors examined are directly amenable to policy responses, and thus, generate key knowledge for policymakers. In addition, we also used longitudinal data to differentiate within-person and between-person effects of income support on MH. This allowed us to control for unobserved factors and assess time-specific effects of income support on MH. Finally, we considered how transitions to and between categories of income support predict changes in MH.
Methods
Sample
We report analyses of data drawn from nine waves of the Household, Income and Labour Dynamics in Australia (HILDA) Survey. Extensive details of the HILDA Survey design have been previously published (Wooden and Watson, 2007; Wooden et al., 2002), so we provide a brief description of the survey features directly relevant to this study. HILDA is a nationally representative longitudinal household panel survey with a multistage sampling design that shares similarities with other national panel surveys such as the British Household Panel Survey, the Canadian Survey of Labour and Income Dynamics and the German Socio-Economic Panel. Interviews have been conducted annually since the year 2001, with data provided by each household member aged 15 years and older via a personal interview and a self-completion questionnaire. The personal interview collects information on general household characteristics and composition, socio-demographics and sources of income for each individual. The self-completion questionnaire collects information on personal characteristics and attitudes, including measures of general health and well-being, lifestyle behaviours, life events and financial stress.
HILDA has maintained good retention of the wave 1 sample, with response and retention rates comparable to other national panel surveys. A wave 1 response rate of 66% of households and 61% of individuals resulted in an initial sample of 7682 households and 13,969 individuals. The wave 2 response rate was 86.8%, and in subsequent waves the response rates have been consistently above 90%, resulting in the retention of 66% of wave 1 respondents at wave 9. Higher levels of attrition have been reported for participants who are younger, of Aboriginal or Torres Strait Islander origin, single, unemployed, of non-English speaking background, or working in low-skilled occupations. The HILDA Survey was approved by the Faculty of Business and Economics Human Ethics Advisory Committee at the University of Melbourne.
Although HILDA augments its sample at each wave to include new household members, to remain comparable with the reference population of Australian residents in 2001, we restricted our analyses to the original wave 1 respondents who returned the self-completion questionnaire, which included the measure of MH, and from waves in which they were of working age (men aged 15–65 and women aged 15–60). As we included respondents who failed to participate in all nine waves for our analyses, the sample was an unbalanced panel. Respondents who returned to the study after a period of non-participation were also retained for the analyses.
Measures
Mental health
The outcome measure analysed in this study was the MH subscale from the Short Form 36 (SF-36) questionnaire (Ware, 2000; Ware and Gandek, 1998). The SF-36 is a 36-item self-completion measure with eight subscales that are designed to give a multidimensional assessment of health status over the previous 4 weeks, covering physical, psychological and social functioning, as well as symptoms and limitations arising from poor health. Scores on each of the eight subscales range between 0 and 100, with higher scores reflecting better health or higher levels of functioning. The SF-36 has sound psychometric properties and has been validated for use as a measure of mental and physical health inequalities in HILDA (Butterworth and Crosier, 2004). The SF-36 MH subscale consists of five items that assess symptoms of anxiety and depression (Rumpf et al., 2001). It is considered an effective screening tool for identifying mood disorders in the general population (Gill et al., 2006) and is commonly used as a general measure of MH in psychiatric epidemiological research. Although there is no universally accepted clinically meaningful difference on the MH subscale, a difference of three points on the norm-based (T-score) scale has been suggested to reflect a minimal important difference (Ware et al., 2007) and a difference of four or more on the unstandardised scale has been characterised as indicating a moderate effect (Contopoulos-Ioannidis et al., 2009).
Income support status
In line with previous analyses of welfare receipt in Australia, we defined seven income support groups that reflect the purpose of the payment and the current circumstances of recipient (Table 1). Those who did not report receiving any government benefits, pensions or allowances were defined as No income support. Respondents who were neither married nor in a de facto relationship and reported receiving parenting benefits were defined as Parenting Payment Single (PPS), while respondents who were married or in a de facto relationship and reported receiving parenting benefits were defined as Parenting Payment Partnered (PPP). Respondents on Aboriginal Study Assistance (Abstudy), non-Aboriginal Study Assistance (Austudy) and full-time students receiving Youth Allowance were classified as recipients of student payments. Respondents who were not partaking in full-time study and were in receipt of Newstart or Youth Allowance were classified as recipients of unemployment payments. Respondents on either Disability Support Pension or Sickness Allowance were classified as recipients of disability payments. Respondents on Mature Age Allowance, Mature Age Partner Allowance, Widow Allowance, Partner Allowance, Service Pension, War Widow Pension, Wife Pension and Department of Veterans Affairs (DVA) disability pensions were classified as recipients of MAPs. Many of these MAPs are no longer available for new applicants. Finally, respondents reporting receipt of special benefits, Carer Payment or Carer Allowance or undisclosed payment types were classified in a miscellaneous payment group (other). Where respondents reported multiple payment types, they were categorised in the income support group that best characterised their current circumstances. This was determined by prioritising in the following order: MAP study, disability, unemployment, PPS, PPP, other, none.
Criteria for each of the seven income support groups and their corresponding benefit, pension and allowances.

Closed to new applications and phased out during the study. Abstudy: Aboriginal Study Assistance; Austudy: non-Aboriginal Study Assistance; FT: full-time; N/A: not applicable.
Covariates
Socio-demographic variables included age, gender, marital status (married or de facto, single or never married, divorced or separated, and widowed), housing tenure (currently renting, not currently renting) and educational achievement (early school-leaver, completed high school, post-secondary non-tertiary, and tertiary). Temporal variables were constructed in both linear and categorical formats. Linear temporal variables included age at baseline, mean-centred at 37 years and time-defined by years in study. Their categorical variable constructions included 10-year age groups and time as year of study. Parental occupation was coded according to the Australian and New Zealand Classification of Occupation taxonomy (Australian Bureau of Statistics, 2006) and used as a proxy for socio-economic position in early life/childhood disadvantage. Work history was calculated as the proportion of years spent in employment since first leaving full-time education. Lifestyle factors included smoking status (non-smoker, former smoker, current smoker) and alcohol consumption (currently abstaining, two or fewer standard drinks consumed in a session, and more than two standard drinks consumed in a session). The coding of alcohol consumption was in line with current Australian National Health and Medical Research Council (NHMRC) guidelines (NHMRC, 2009). The Physical Functioning subscale of the SF-36 was used as a measure of physical health and was centred at a score of 80.
Financial status variables included measures of financial hardship and equivalised income. Financial hardship was defined by the number of positive responses to seven items that asked if respondents had experienced any of the following events over the past 12 months due to a shortage of money: could not pay utility bills; asked for financial assistance from friends or family; could not pay mortgage or rent on time; pawned or sold possessions; were unable to heat home; went without meals; or asked for help from community/welfare organisations. Household equivalised income was estimated using the OECD modified scale to control for variations in household size and composition (Australian Bureau of Statistics, 2012; Hagenaars et al., 1994). Equivalised income was centred at AUD$21,000 and top-coded at AUD$125,000; these figures corresponded with the median equivalised income and the 99th percentile for the year 2006 respectively. Negative equivalised household income was coded as zero. All covariates except for age at baseline, gender and parental occupation were time-varying, reflecting individual circumstances at each wave.
Analyses
A series of linear mixed models with random intercepts were used to test for predictors of MH scores. Residual plots confirmed that the assumptions of linear regression were met. Initial unadjusted analyses modelled the seven dummy coded indicators of income support payment as time-varying predictors. Variables were then added sequentially to the unadjusted model in the following blocks:
Model 1 included time in study and socio- demographic variables (age and gender). We compared results across models that included age and time as linear or categorical variables.
Model 2 added variables reflecting socio-economic position and human capital, including highest educational attainment, parental occupation, housing tenure, and time in full-time employment.
Model 3 added marital status.
Model 4 added physical function subscale scores from the SF-36.
Model 5 added lifestyle behaviours of smoking status and alcohol consumption.
Finally, model 6 added financial status variables of equivalised income and financial hardship.
To test if the relationship between welfare receipt and MH differed between age groups and gender, interaction terms between these covariates and each income support payment type were included in subsequent models. Also, because some payments types predominate in particular age groups and may have varying impacts at different life stages, model 6 was rerun, stratified by 10-year age groups.
To distinguish between overall differences between respondents and individual variation over time in MH as a function of income support, model 5 was extended to include between-person and within-person effects of payment type (Curran and Bauer, 2011). In this model, income support was partitioned into time-invariant variables identifying respondents who were ever in receipt of a particular payment at any time during the data collection, and time-varying variables reflecting occasion-specific indicators of currently receiving income support. The reference categories for these analyses were respondents never in receipt of income support, and times when not in receipt of payments.
A final set of analyses employed random effect models to examine how transitions to particular welfare payments from no income support, switching between income support payment types and remaining on a particular payment type, predicted change in MH scores from the prior wave. These analyses followed the same model building procedure as the first set of analyses with the addition of lagged MH scores (centred at 75). We defined three sub-samples by the basis of their payment transitions over subsequent waves – for example, transitioning to payment, switching between payments, remaining on payment – and tested the models separately for each sub-sample. All analyses were conducted using the statistical software Stata 11 (StataCorp LP, College Station, Texas, USA).
Results
Descriptive characteristics of the baseline sample are shown in Table 2; there were 11,701 respondents (49% men) with a mean age of 38 (SD = 13.1). There were 242 respondents who identified as Aboriginal or Torres Strait Islander and 1695 respondents reported a non-English speaking background. At baseline, 71% of respondents were employed, 5% were unemployed and 24% were not in the labour force. At baseline, the MH score had a mean of 73.3 (SD = 17.5) with negative skew (-0.97). The mean MH scores for each income support payment from 2001 to 2009 are shown in Table 3. A total of 4146 (35.4%) respondents reported receiving some form of income support on at least one occasion over the 9-year period and 56.1% of these (i.e. 19.9% of the sample) were on income support on every occasion that they participated in the study. Note that the proportion of respondents who were on income support on every available wave may be inflated due to greater attrition among income recipients. Relative to those not receiving income support, the risk of later attrition was higher among participants receiving disability (odds ratio (OR) = 1.32, SE = 0.18, p = 0.04) or unemployment payments (OR = 1.48, SE = 0.19, p < 0.01), even after adjusting for the effects of age, gender, education and time in study. Attrition predominantly followed a monotone missing data pattern; respondents who missed one follow-up wave typically did not participate in future waves, however, 15.4% of respondents with missing wave data did return at a later wave. Overall, 5642 (48.2%) respondents participated in all nine waves with a further 1069 (9.1%) respondents missing on only one occasion.
Baseline sample profile by income support group (N = 11,701).
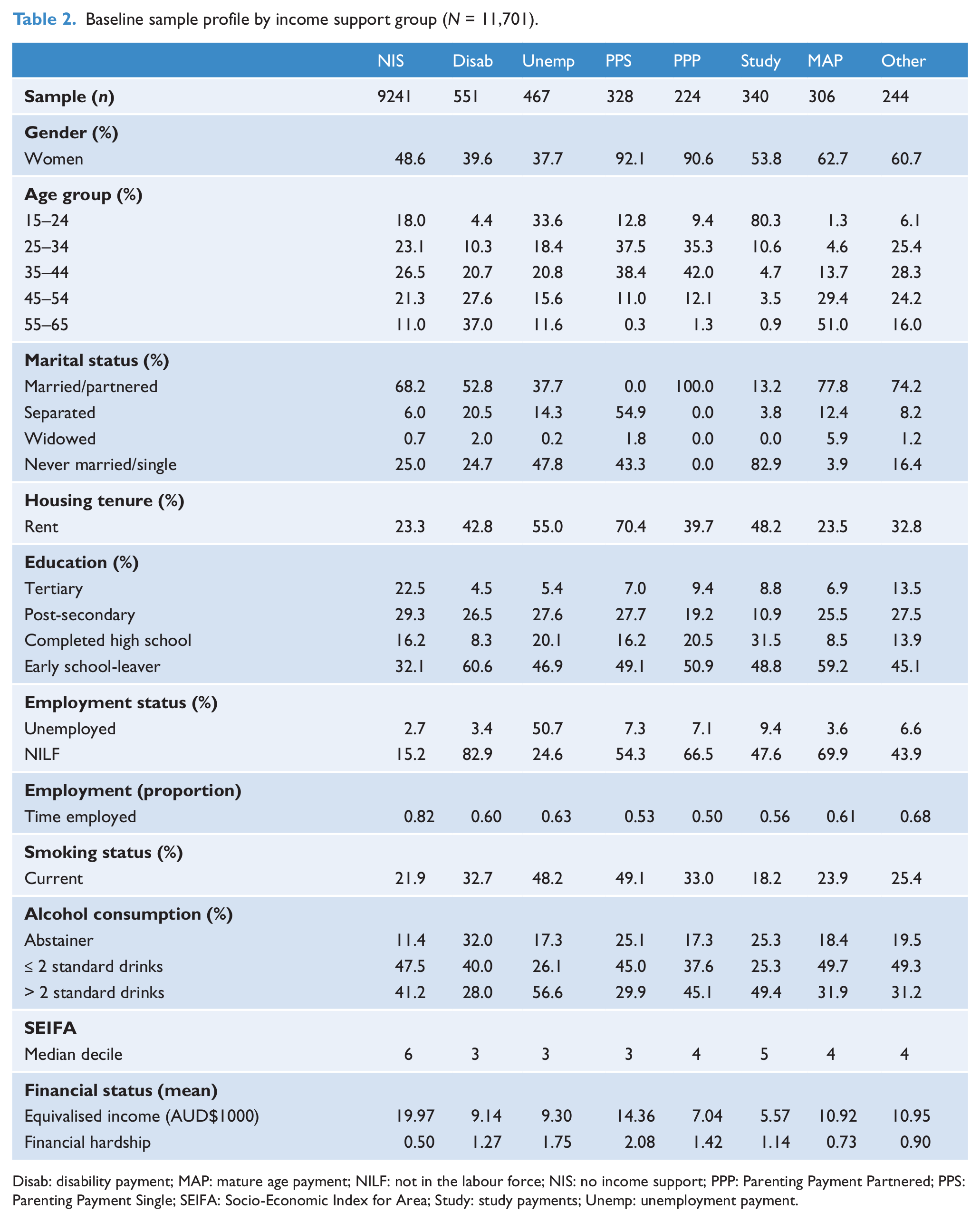
Disab: disability payment; MAP: mature age payment; NILF: not in the labour force; NIS: no income support; PPP: Parenting Payment Partnered; PPS: Parenting Payment Single; SEIFA: Socio-Economic Index for Area; Study: study payments; Unemp: unemployment payment.
Mean and standard deviations (SDs) for SF-36 Mental Health scores by type of income support and year of observation.
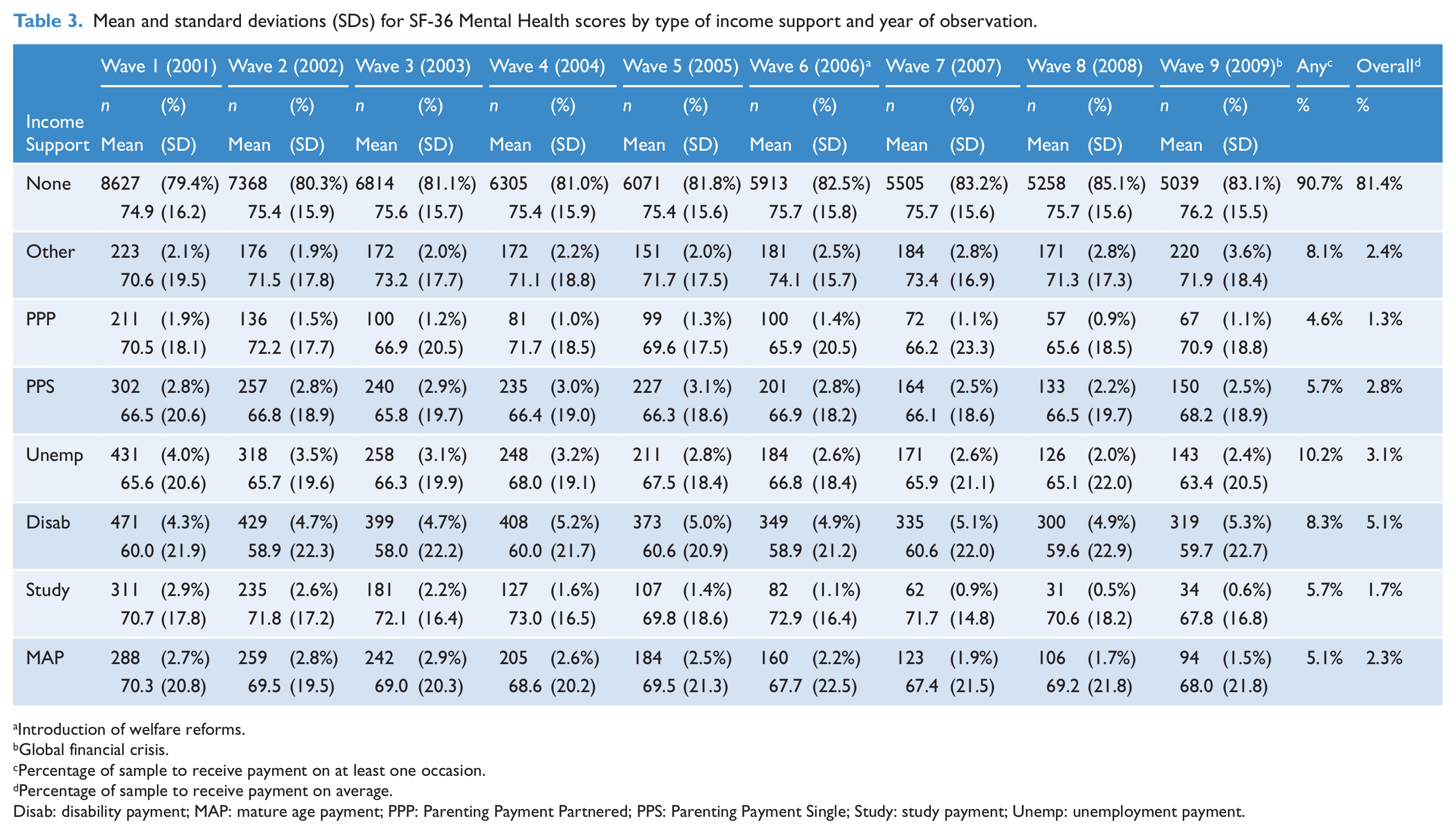
Introduction of welfare reforms.
Global financial crisis.
Percentage of sample to receive payment on at least one occasion.
Percentage of sample to receive payment on average.
Disab: disability payment; MAP: mature age payment; PPP: Parenting Payment Partnered; PPS: Parenting Payment Single; Study: study payment; Unemp: unemployment payment.
Longitudinal data from 11,036 respondents were analysed, with an average of 5.7 observations per respondent. At each successive wave, there were considerably fewer participants receiving study payments and MAPs. This was most likely a result of the closure of MAPs to new recipients and the ageing of the cohort across time (with student payment recipients moving into the workforce or out of full-time study, and MAP recipients no longer of working age). The proportion of the sample on unemployment benefits halved throughout the duration of the study, whereas the proportion of the sample on disability payments was relatively stable. The overall proportion of respondents receiving income support decreased at wave 6, although the proportion of respondents receiving miscellaneous payment types increased after wave 6. There also appeared to be a slight increase in the number of respondents on income support payments in wave 9 (p < 0.01).
The unadjusted model indicated that all income support payment types were associated with lower scores on the SF-36 MH subscale (i.e. poorer MH). However, only receipt of disability, unemployment, and MAPs remained reliable predictors after adjusting for demographic variables, socio-economic position, marital status, physical health, lifestyle behaviours and financial status (Table 4). The association between student payments and MH was explained by markers of socio-economic position (model 2), whereas the association of parenting (single and partnered) and other payments with MH was explained by financial hardship and equivalised income (model 6). Post-hoc analyses revealed that marital status also explained the association between student payments and MH. Overall, respondents in receipt of disability payments had the lowest MH scores followed by those on unemployment payments. Although there were no substantive differences between models that included age and time as either linear or categorical variable constructions, we report results from models with linear age due to their parsimony and more optimal model fit [linear Bayesian information criterion (BIC) = 500651; categorical BIC = 500717].
Effects of income support on the SF-36 Mental Health subscale estimated by linear mixed models (n = 11,036).
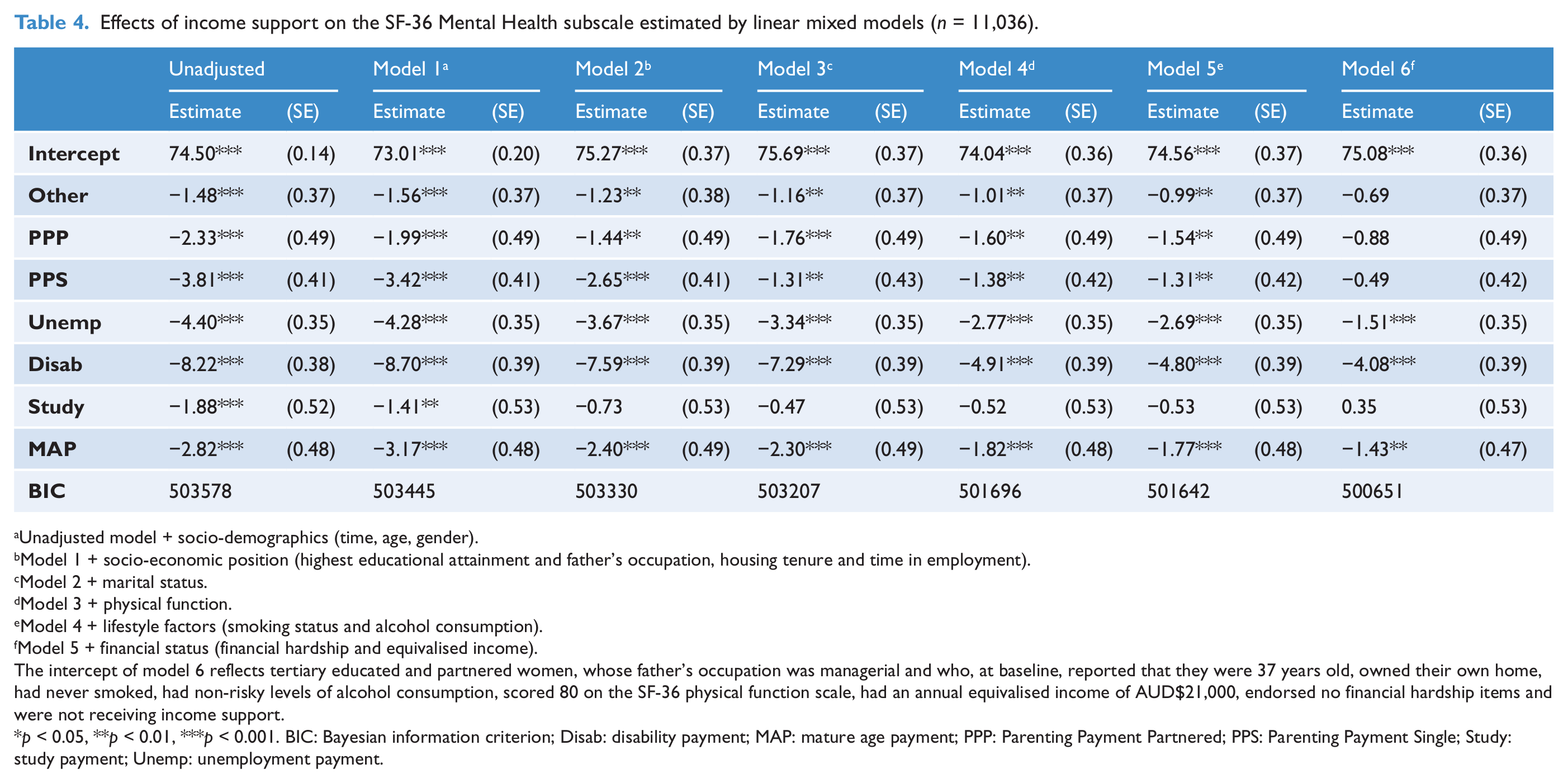
Unadjusted model + socio-demographics (time, age, gender).
Model 1 + socio-economic position (highest educational attainment and father’s occupation, housing tenure and time in employment).
Model 2 + marital status.
Model 3 + physical function.
Model 4 + lifestyle factors (smoking status and alcohol consumption).
Model 5 + financial status (financial hardship and equivalised income).
The intercept of model 6 reflects tertiary educated and partnered women, whose father’s occupation was managerial and who, at baseline, reported that they were 37 years old, owned their own home, had never smoked, had non-risky levels of alcohol consumption, scored 80 on the SF-36 physical function scale, had an annual equivalised income of AUD$21,000, endorsed no financial hardship items and were not receiving income support.
p < 0.05, **p < 0.01, ***p < 0.001. BIC: Bayesian information criterion; Disab: disability payment; MAP: mature age payment; PPP: Parenting Payment Partnered; PPS: Parenting Payment Single; Study: study payment; Unemp: unemployment payment.
Covariates
Model 6 indicated that lower MH scores were more likely to be observed among respondents who were women, older, not partnered, either reported their father to be a machine operator or of no occupation, were currently renting, had spent less time in employment since leaving full-time education, were current smokers, reported either risky levels of alcohol consumption or alcohol abstention, poor physical functioning, estimated to have lower annual equivalised income and reported greater levels of financial hardship. The effects of mother’s occupation were not included in the reported analyses as they did not contribute over and above the effects of father’s occupation.
Gender- and cohort-specific effects
There were no significant interactions between gender and welfare receipt; however, there were significant interactions between the 10-year age group and income support type. As these interaction terms indicated that results were not consistent across all ages, sensitivity analyses were conducted by stratifying model 6 by the 10-year baseline age groups. These analyses revealed disability payments were independent predictors of lower MH scores for older age groups including those aged 35–44, 45–54 and 55–65 but not for younger cohorts aged 15–24 or 25–34. Similarly, receipt of unemployment payments independently predicted lower MH only among those aged 35–44 and those aged 55–65. However, receipt of MAPs was only associated with lower MH scores among younger recipients aged 45–55. Among those aged between 15–24 and 25–34 at baseline, the association between MH and receipt of either unemployment payments or disability payments was explained by financial hardship and equivalised income.
Within-person and between-person effects
The results of two models testing within-person (currently receiving income support) and between-person (ever receiving income support) effects are presented in Table 5. The first model adjusted for age, gender and time in study, whereas the second model additionally included all current socio-demographic, lifestyle, physical function and financial status variables. The age, gender and time-adjusted model indicated that respondents who were ever in receipt of disability payments, unemployment payments, PPS and MAPs had poorer MH than those who never received these payments, and that these respondents had even poorer MH at the times at which they were receiving these payments. Between-person effects were attenuated but remained significant in the full multivariate adjusted analysis, but within-person effects remained significant only for disability and unemployment payments. The contemporaneous association between PPS and MAPs with MH was explained by marital status.
Effects of currently and ever receiving income support on the SF-36 Mental Health subscale estimated by linear mixed models (n = 11,031), adjusted for socio-demographics, socio-economic position, lifestyle factors, physical function and financial status.
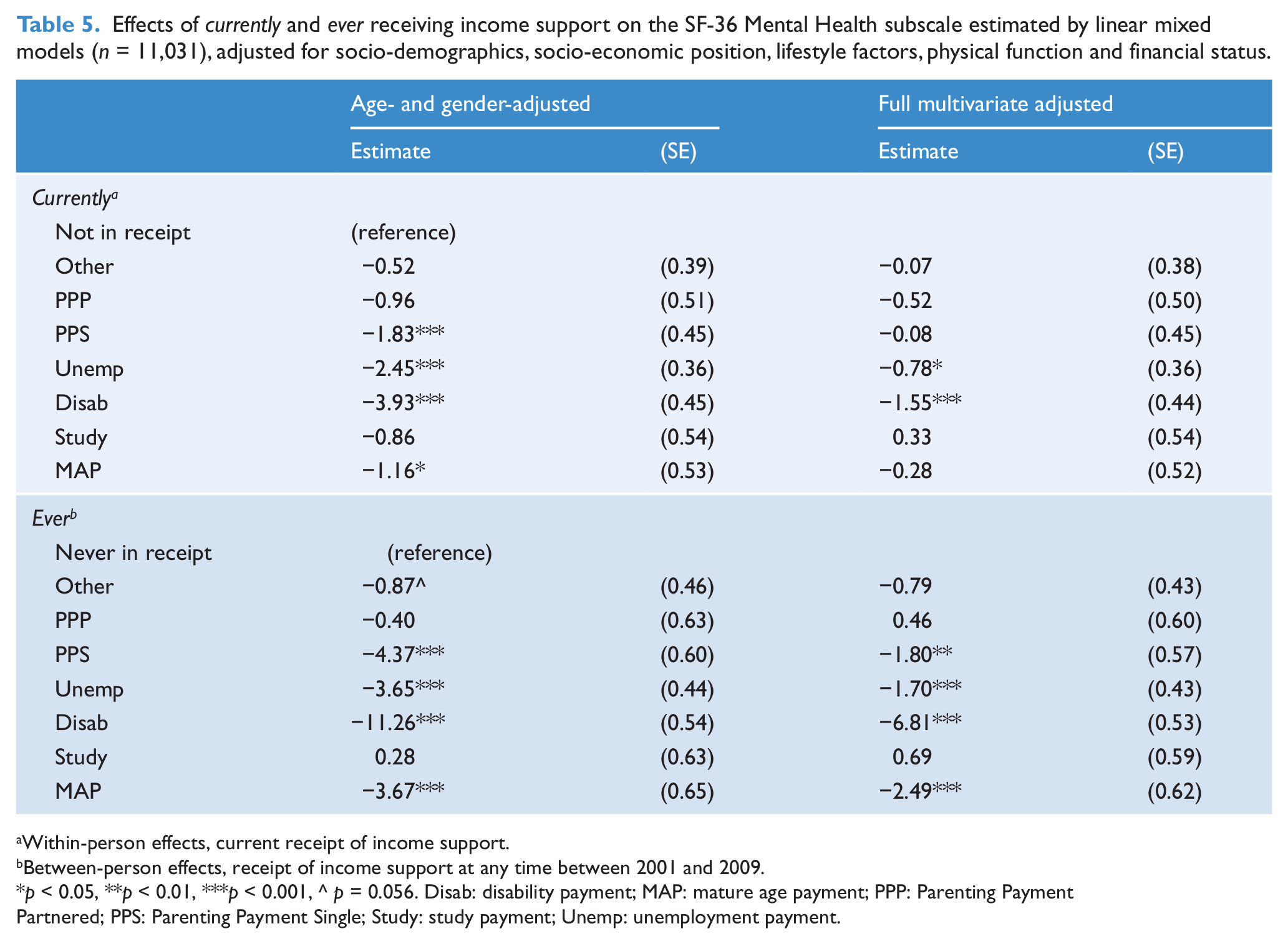
Within-person effects, current receipt of income support.
Between-person effects, receipt of income support at any time between 2001 and 2009.
p < 0.05, **p < 0.01, ***p < 0.001, ^ p = 0.056. Disab: disability payment; MAP: mature age payment; PPP: Parenting Payment Partnered; PPS: Parenting Payment Single; Study: study payment; Unemp: unemployment payment.
Income support transitions
To test if income support transitions predicted differences in MH scores, we identified three sub-samples that were defined by their income support status across adjacent waves. The effects of transitioning to an income support payment, switching between income support payments and remaining on a particular income support payment, are shown in Table 6. These estimates are adjusted for lagged MH scores, as well as current socio-demographic, lifestyle, physical function and financial status variables. For respondents not in receipt of income support the previous year, transitions onto disability payments (β = -3.95) or PPS (β = -2.03) were associated with greater reductions in MH than those who remained off payment. Respondents who switched from any other payment type to either a PPS (β =-3.65) or a disability payment (β =-3.23) were estimated to a greater reduction in MH compared to those who transitioned off income support. Respondents who transitioned from any other payment type to a student payment appeared to have increased MH scores, but this association was not statistically significant (β = 2.45). Finally, remaining on disability payments (β = -1.46) or MAPs (β = -2.10) predicted a greater reduction in MH compared to those who remained on no payment.
SF-36 mental health subscale scores predicted by switching between income support payments, transitioning to income support payments and remaining on a specific income support payment.
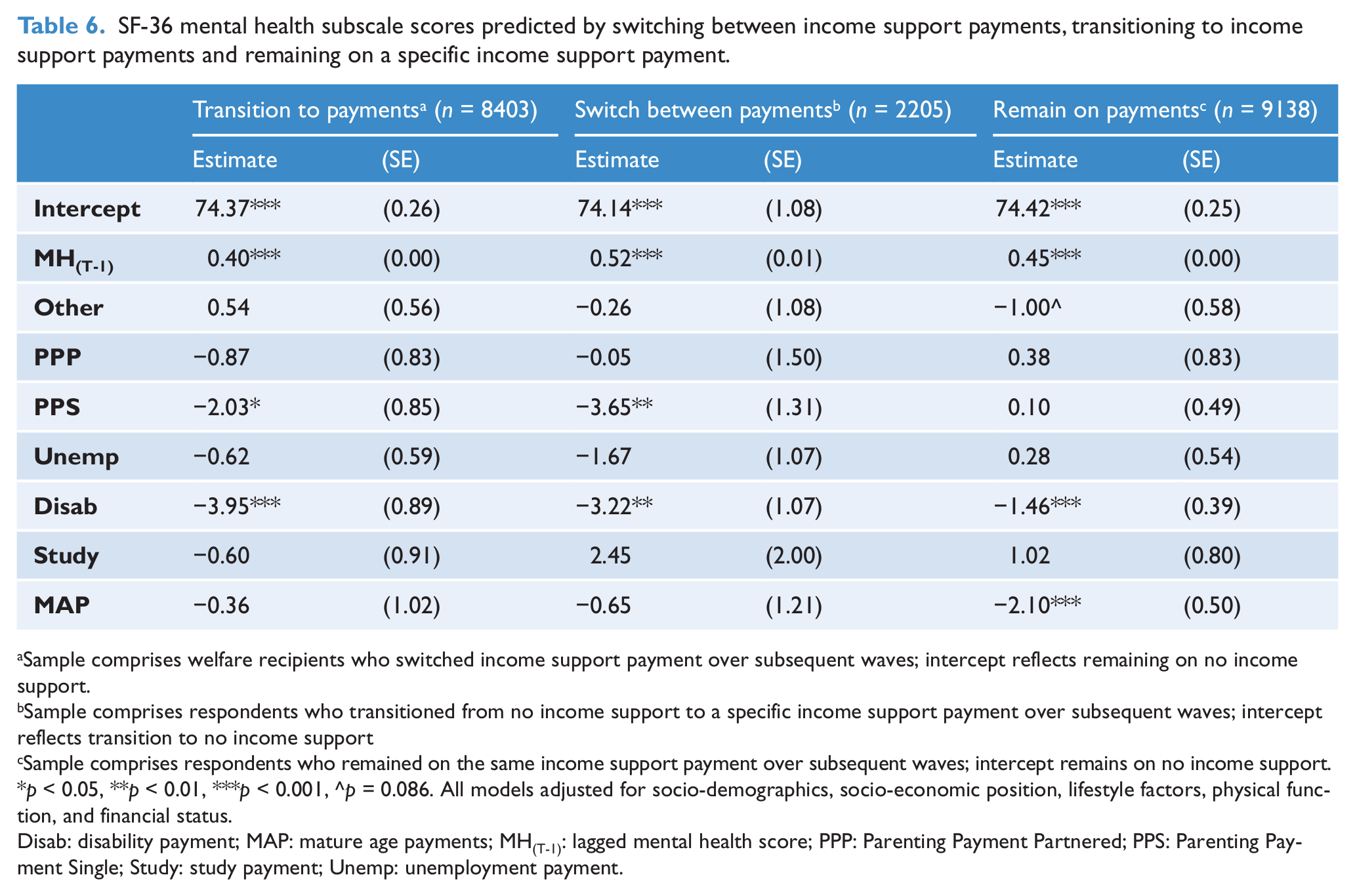
Sample comprises welfare recipients who switched income support payment over subsequent waves; intercept reflects remaining on no income support.
Sample comprises respondents who transitioned from no income support to a specific income support payment over subsequent waves; intercept reflects transition to no income support
Sample comprises respondents who remained on the same income support payment over subsequent waves; intercept remains on no income support.
p < 0.05, **p < 0.01, ***p < 0.001, ^p = 0.086. All models adjusted for socio-demographics, socio-economic position, lifestyle factors, physical function, and financial status.
Disab: disability payment; MAP: mature age payments; MH(T-1): lagged mental health score; PPP: Parenting Payment Partnered; PPS: Parenting Payment Single; Study: study payment; Unemp: unemployment payment.
Discussion
Previous research has documented that income support recipients are much more likely to experience poor MH than those not receiving welfare payments. Their poorer MH may represent a significant barrier to future workforce engagement and their chances of moving off payment. MH, therefore, should be a focus of employment and welfare policy. However, deciding on the most appropriate policy response does depend on the nature of the relationship between welfare receipt and MH. This study investigated whether the poorer MH of welfare recipients reflected their underlying vulnerability, whether welfare receipt was driven by their poor MH, or whether poor MH was a direct consequence of being on welfare payments. In doing this, we built models that controlled for an extensive range of potential confounders and mediators. We contrasted the overall MH of vulnerable individuals with their MH at the times they were in receipt of payment and we investigated the MH consequences of specific income support transitions.
All categories of income support were associated with increased risk of poor MH, but the MH profile of each payment type varied and explanations for the association also differed across payments. The key finding was that recipients of disability, unemployment and MAPs had poorer MH regardless of their personal, social and financial circumstances. It is also pertinent to note that recipients of unemployment and disability payments had poorer MH at times when they were receiving income support in comparison to times when they were not. Moreover, people who received disability, unemployment, MAPs and parenting payments for single parents at any point during the study period had poorer overall MH when compared to those who never received any income support, even at times when they were not reliant on payment. Despite this, the effects of welfare transitions were inconsistent. Change in MH was not reliably predicted by transitioning to, or remaining on, unemployment payments. In contrast, transitions to parenting payments for single parents and disability payments were associated with a decline in MH. Finally, unlike recent analyses of UK data (Ford et al., 2010), we did not find that welfare receipt had a greater MH burden on men than women.
The current results provide some support for explanations that the association between MH and welfare receipt reflects health selection and the effect of underlying factors. Welfare recipients had poorer MH, even at times they were not in receipt of payments, and change in MH did not correspond with transitioning to, or remaining on, unemployment payments. On the other hand, poorer MH among recipients of student payments was attributed to their socio-economic position and attainment of life-course milestones (marriage, housing tenure, full-time employment), whereas recipients of parenting payments and other miscellaneous payments, which included carer allowances, were more likely to have poorer MH as a result of increased financial strain. It is notable that these latter payments (student, parenting and carer payments) are designed to support people performing important social roles. The absence of direct effects of welfare receipt on MH may reflect a lack of stigma for these payment types.
However, an underlying disadvantage and general vulnerability did not fully explain the increased risk of poor MH among all groups of welfare recipients. There was evidence of a direct effect for those receiving disability and unemployment payments: they had poorer MH at the times they were in receipt of welfare, and this was not wholly explained by the underlying disadvantage. Thus, poor MH may be due to receipt of the payment itself, explained by the demoralising effects of welfare dependency, the stigmatising attitudes within society to welfare recipients or perhaps other unmeasured experiences that coincide with their time on payment.
Overall, receipt of disability payments had the strongest independent associations with MH. In recent times a greater proportion of recipients have qualified for disability support pensions by virtue of their mental illness (Department of Families Housing Community Services and Indigenous Affairs, 2011). This could be due to the greater openness about MH problems, greater financial incentives to receive disability-related income support over allowances or the fact that income support recipients with poor MH may be less able to meet the stricter mutual obligation work requirements associated with recent welfare reforms (Butterworth et al., 2011a). Interestingly, younger disability payment recipients were less likely to report poorer MH than older recipients, perhaps reflecting the broader recognition of the needs of younger people with disability and the greater support available in educational and workforce settings. The high rates of mental illness within disabled populations, coupled with increasing numbers of recipients reliant on disability payments, makes balancing the needs of people with disability a critical challenge for policy analysts. Greater policy focus on the needs of this group is needed as the Disability Support Pension is one of the largest items of government expenditure, and is under pressure to keep pace with rising living costs. These high expenditure costs are exacerbated as it is a long-term payment and few recipients move off payments to return to the workforce (Brown, 2011).
The effects of welfare receipt may vary across cohorts and be contingent on career progression and the current life stage of recipients. It is interesting to note that the impact of MAPs on MH was most pronounced among the middle-aged cohort, rather than older adults who were nearing retirement age. This could partly be due to the exclusion of women at the age of 60, but may also reflect the stigma associated with receipt of welfare payments at a time individuals are perceived to be at the height of their working life. Similarly, receipt of welfare payments was generally not associated with poorer MH among younger cohorts. One explanation for this finding is that it may be more socially acceptable for adults to receive income support as they approach retirement age or are in the early stages of their working life, and these internalised social norms could moderate the MH impacts of welfare receipt. This notion is consistent with findings from previous studies considering the MH impacts of workforce disengagement during the recent global financial crises (Sargent-Cox et al., 2011) and among older men as they approach retirement (Gill et al., 2006).
Our findings sit within a broader research agenda documenting strong links between social disadvantage and MH problems (Fryers et al., 2003; Muntaner et al., 2004). Emotional stress has been linked with reduced income and lower economic productivity, financial stress and unemployment (Barbaglia et al., 2012; Saunders, 1998). It has been argued that links between socio-economic position and MH reflect both contemporaneous factors and long-term effects from previous life stages (Muntaner et al., 2004). There was compelling evidence, across all payment types, that socio-economic disadvantage explained much if not all of the effect of welfare receipt on MH. These poor personal and social circumstances may also be the actual determinants of one’s eligibility for payment (e.g. relationship dissolution). One of the most obvious explanations for the poorer MH of welfare recipients is the financial insecurity and poverty associated with welfare receipt. Previous analyses of the Australian National Survey of Mental Health and Well-Being identified financial hardship as the strongest independent risk factor for depression among a number of indicators of socio-economic position (Butterworth, 2003c). Hardship and material disadvantage can result in limited access to essential daily consumables and services (Ferrie, 2001; Rodriguez et al., 2001) and thus be a barrier to social inclusion. This exclusion due to financial hardship may cause, maintain and reinforce mental illness (Butterworth et al., 2012). The present analyses found that financial status either entirely explained or partially mediated the poorer MH of welfare recipients. There is currently much discussion of the adequacy of payments such as the Newstart Allowance, the main unemployment payment in Australia, which has not increased in real terms since 1991 and has fallen below the poverty line during this period (Australian Human Right Commission, 2012).
One strength of the rich longitudinal data from HILDA is the ability to model time, history and environmental effects. This allows for the examination of changes in welfare policy and the influence the broader economic context. There was, for example, evidence of a decrease in the number of people on income support coinciding with major welfare reforms introduced in 2006, and some evidence of a (slight) increase in the number of respondents on income support payments in 2009, which corresponded with the timing of the global financial crisis. Future research should investigate the specific impacts of these events. It would be possible to employ a quasi-experimental research design in a naturalistic setting with the HILDA study to answer such questions.
We acknowledge a number of conceptual and methodological limitations to the findings of this study. We have not investigated clinically meaningful differences in the SF-36 MH scale. Our reliance on tests of statistical significance to assess links between MH and welfare receipt may be influenced by sample size and other sample characteristics. Also, we did not adjust for missing data or attrition and the longitudinal methods used precluded the use of wave- specific weights. The analyses presented here do not consider the reciprocal effects of MH on welfare receipt and so do not explicitly test causation explanations. Another issue we have not considered is the duration of welfare reliance. Rodriquez (2001) and colleagues reported that time in unemployment was an independent predictor of depression for men, but not women. Despite these limitations, this paper makes an important contribution to our understanding of the links between MH and income support. The strengths of this paper are the use of national longitudinal data and the adjustment of a broad range of possible confounding factors including childhood disadvantage, current physical functioning and lifestyle behaviours.
In summary, the association between welfare receipt and poor MH suggests welfare recipients may have reduced opportunities to participate in community life and thus avoid social exclusion. Factors underpinning this association may be contingent on the purpose of the payment and the circumstances of the recipient. Individuals on income support who are otherwise engaged in meaningful social roles, such as studying or parenting, seem to be at increased risk of poor MH because of a lack of security, financial strain and broader social disadvantage. In contrast, it appears that for those individuals who are unable to work, then there is a direct link between welfare receipt and poor MH. This could be due to other factors not examined here, such as welfare stigma, other adversity or life events. That there were independent effects of welfare receipt for disability and unemployment payments warrants further investigation. Further research is needed to disentangle the selection-causation effects between MH and income support, specifically identifying the circumstances in which welfare receipt leads to a sense of helplessness and despair, investigating the impact of welfare stigma on well-being, and conversely determining the extent to which poor MH is itself an antecedent of welfare receipt.
Footnotes
Funding
PB was funded by NHMRC fellowship 525410. This paper was funded by the Australian Research Council grant DP120101887 and uses unit record data from the HILDA Survey. The HILDA project was initiated and is funded by the Australian Government Department of Families, Housing, Community Services and Indigenous Affairs (FaHCSIA) and is managed by the Melbourne Institute of Applied Economic and Social Research (the Melbourne Institute). The findings and views reported in this paper, however, are those of the authors and should not be attributed to either FaHCSIA or the Melbourne Institute.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.