
Abstract
Objective:
To evaluate the efficacy of the Flinders Program™ of chronic condition management on alcohol use, psychosocial well-being and quality of life in Vietnam veterans with alcohol misuse.
Method:
This 9-month wait-list, randomised controlled trial used the Alcohol Use Disorders Identification Test (AUDIT) score ≥ 8 as the entry criterion. Intervention veterans received the Flinders Program plus usual care and controls received usual care. The primary outcome measure was AUDIT score at baseline, 3, 6 and 9 months. Secondary measures included quality of life, alcohol dependence (DSM-IV), anxiety and depression. All measures were repeated at variable trial end dates between 9 and 18 months in the intervention group.
Results:
Randomisation resulted in 46 intervention and 31 control participants. Intent-to-treat analyses showed AUDIT scores improved significantly from baseline to 9-month follow-up (p = 0.039) in the intervention group compared to control group. The control group had 1.46 times the risk of alcohol dependence than the intervention group at 9 months (p = 0.027). There were no significant differences between groups for secondary measures. Within-group analyses showed that both groups significantly improved in AUDIT (p < 0.001), anxiety and depression (p < 0.01), anger (p < 0.001), and post-traumatic stress (p < 0.01). Improvements in AUDIT (p < 0.001) and alcohol dependence were maintained in the intervention group to 18 months.
Conclusions:
Use of the Flinders Program in addition to usual care resulted in reduced alcohol use, reduced alcohol dependence, and global clinical improvement in Vietnam veterans with risky alcohol behaviours and chronic mental health problems. The findings demonstrate that the Flinders Program provides a structured framework for delivering self-management support, case management and coordinated care for people with chronic conditions. This clinical approach has the potential to bridge the gap between physical and mental illness service delivery for people with long-term conditions in Australia.
Introduction
Nearly one in five Australians is affected by a mental illness in any 1 year. Approximately 20% of men and 13% of women are hazardous or at-risk alcohol drinkers, with 5% of men and 2% of women being alcohol dependent (Pead et al., 2005). Alcohol use is a significant issue for the veteran community, with dependence being a common problem among veterans with a mental health disability (Department of Veterans’ Affairs, 2001; O’Connor and Simmons, 2002; Pead et al., 2005). The level of co-morbidity between alcohol and physical and mental disorders among veterans is high. For veterans with alcohol dependence, total treatment costs are estimated to be 50% higher than for other veterans with disabilities (O’Connor and Simmons, 2002).
Over the last decade concerns about the emerging crisis in chronic disease prevalence and cost to the Australian community led the Council of Australian Governments to establish the National Chronic Disease Strategy (NCDS) (NHPAC, 2006) and the Australian Better Health Initiative (ABHI) (Commonwealth of Australia, 2008), which aim to prevent and improve the management of chronic diseases in Australia. In the NCDS, depression is identified as a significant co-morbidity, and mental health is included as one of the National Health Priorities (AIHW, 2008) alongside diseases such as diabetes, cardiac and respiratory disorders. [In this paper, we use ‘chronic conditions’ to refer to both chronic physical diseases and mental disorders.]
Education of health professionals (HPs) in ways to better support patients’ self-management of their chronic conditions is one of the five elements of the ABHI (Commonwealth of Australia, 2007). The Flinders Program of chronic condition management provides a way of implementing key elements of the ABHI by integrating self-management support with chronic disease or condition management using cognitive behavioural principles for cycles of care planning, review and monitoring to facilitate patient behavioural change (Battersby et al., 2007a). The Flinders Human Behaviour and Health Research Unit developed the Flinders Program (FP) from the finding in the South Australian HealthPlus coordinated care trial that assessment of a person’s self-management knowledge, behaviours and barriers was the key to determining who needed coordinated care, and that targeted self-management support could assist the patient to achieve improved health outcomes (Battersby and SA HealthPlus team, 2005; Battersby et al., 2003). The FP is not a stand-alone intervention; rather, it is a clinician-initiated process aiming to tailor interventions to meet the person’s needs whilst simultaneously motivating the patient to achieve their medical, psychosocial or lifestyle risk factor goals. The HP is trained to act as coach and coordinator of the person’s services over a 12-month period. Evidence for the acceptability and effectiveness of the FP has been found in patients with a range of chronic mental and physical disorders (Battersby et al., 2000, 2001, 2008; Crotty et al., 2009; Harvey et al., 2008; Lawn et al., 2007, 2009).
Because the FP was designed as a generic process for both medical and psychiatric conditions, it was thought to be a suitable intervention for Vietnam veterans with risky alcohol behaviours who were known to have complex co-morbidities including post-traumatic stress disorder (PTSD), depression and alcohol-related physical complications. The Department of Veterans’ Affairs (DVA) developed Alcohol Practice Guidelines (Pead et al., 2005) and self-help materials such as The Right Mix—Your Health and Alcohol initiatives (Department of Veterans’ Affairs, 2003) for use by HPs and veterans to reduce alcohol use. An additional impetus for the study was the need to identify an evidence-based method of self-management support for veterans that could be integrated with primary and secondary care.
The aim of this randomised controlled trial (RCT) was to determine whether the FP coupled with evidence-based usual care from existing resources could improve alcohol use and health outcomes for Vietnam veterans with alcohol-related chronic conditions compared to usual care.
Methods
Recruitment and participants
This 9-month, wait-list, randomised controlled trial was conducted in the Adelaide metropolitan area and used an opt-in design with Vietnam veterans (veterans) being informed about the study through their HPs, Veterans and Veterans Family Counselling Service (VVCS), Repatriation General Hospital Daw Park, Vietnam veteran ex-service organisations, and the media. Interested veterans rang the project telephone number and the research officer conducted a telephone screening interview to determine participant eligibility. Eligibility criteria included: being a Vietnam veteran, living within the geographical area of the southern, western, central and eastern Adelaide divisions of general practice, having an Alcohol Use Disorders Identification Test (AUDIT) score ≥ 8 (indicating risky drinking), having a chronic condition, absence of a debilitating physical or mental condition which would prevent participation in the study, and being eligible for Veteran medical benefits. Recruitment occurred over a 15-month period. Approval to conduct the study was granted by the Department of Veterans’ Affairs Human Research Ethics Committee and the Repatriation General Hospital Research and Ethics Committee.
Randomisation, allocation concealment and blinding
The research officer (RO) allocated the eligible veterans to intervention or control by drawing an envelope from one of 20 concealed packets each containing 10 envelopes. Prior to commencement of the recruitment phase the study administrative officer (AO) used the complete randomisation method (Friedman et al., 1998; Raphael, 2000) to provide a computer-generated list of numbers from 1 to 200 based on a sequence of 1:1 (intervention: control), coded on individual pieces of paper in concealed envelopes within a series of packets (numbered sequentially). The AO was blind to the eligibility interview and randomisation allocation conducted by the RO, who was blinded to the randomisation sequence. The veterans receiving the FP were aware of their allocated arm, as were the registered nurses who conducted the FP and the independent psychiatrists who saw the veterans; however, the outcome data were collected and entered by the AO who was blind to the allocation, and the data were analysed independently by DS.
Procedure
Two registered nurses shared the research nurse (RN) position and conducted the FP with intervention veterans at offices within the Department of Psychiatry, Flinders University. Each RN had a nursing degree and postgraduate qualifications, with over 10 years of primary care nursing experience. One had 12 years of drug and alcohol experience, but neither had mental health qualifications. Each RN was a certified provider of the FP and supervised in terms of consistency of delivery by the RO, who was also certified to provide the FP. Three independent psychiatrists, who were not known to the veterans, conducted psychiatric assessments and rated global clinical severity and improvement.
During the first visit, the RN obtained written consent for the study and baseline measures were collected. The RN conducted a Flinders care plan assessment with the intervention veteran and prepared a draft care plan for review by the psychiatrist. Both intervention and control participants were assessed by the independent psychiatrist and psychiatric diagnoses were made. The psychiatrist sent a letter to the general practitioner (GP) for both groups in which he/she documented the diagnoses – and for the control veterans, the case was summarised and recommendations of a medical nature made which did not include self-management advice. Where risk to the veteran or others was identified, the RN or psychiatrist contacted the appropriate medical (GP) or psychiatric service for an immediate response.
For the intervention veterans, the psychiatrist made recommendations for the draft care plan. The veteran was provided with a copy of the draft care plan and was asked to discuss this with his/her GP who would finalise the care plan. Intervention veterans were seen by the RN at 1, 3, 6 and 9 months, and contacted by telephone at 4½ and 7½ months to review their progress and provide coaching to achieve their goals. The RN acted as navigator to assist the veteran to access health services and coordinate their care when necessary. The RNs used the Alcohol Practice Guidelines (Pead et al., 2005) and self-help materials such as The Right Mix—Your Health and Alcohol (Department of Veterans’ Affairs, 2003) as well as information about medications to educate the veterans about safe drinking and self-management of alcohol use. If the RN and veteran identified that the veteran could benefit from learning self-management skills, such as action planning and problem solving, attendance at the Stanford Chronic Disease Self-Management group Program (SCDSMP) was included on the care plan. Partners were also invited to attend. The SCDSMP was delivered jointly by the RO and a veteran peer leader who had completed a 4-day training program.
The control group completed questionnaires by mail at 3 and 6 months, then at 9 months they were seen by the RN to complete another set of questionnaires, were reviewed by the independent psychiatrist and were offered the FP and the SCDSMP. At 9 months, the intervention group completed questionnaires, were reviewed by the independent psychiatrist and were invited to continue follow-up for another 9 months. The psychiatrists had no role in the veterans’ management during the intervention period. The intervention group were then administered outcome assessments by the RN and psychiatrists at 18 months or earlier for veterans whose follow-up period was limited by later recruitment into the study.
Intervention
The intervention had multiple components consisting of the FP, usual care, the Alcohol Practice Guidelines (Pead et al., 2005) and self-help materials such as The Right Mix—Your Health and Alcohol, and the option to participate in the SCDSMP (Stanford School of Medicine, 2011). The intervention was conducted over 9 months.
Flinders Program: The aim of the FP is to engage the veteran in his/her own care by providing a structured clinical process for a HP to use that will motivate the veteran to change his/her behaviour and achieve long-lasting medical and psychosocial goals. The FP begins with the veteran completing the Partners in Health (PIH) questionnaire, a 14-item 0–8 Likert scale assessment of self-management, knowledge, shared decision making, symptom management, adherence to medical management, impact of the condition(s) and lifestyle behaviours. The HP conducts the Cue and Response (C&R) interview with the veteran using open-ended questions to explore the same 14 items as the PIH. This process leads to the veteran and HP deciding which of the 14 issues require intervention. The HP and veteran then identify the veteran’s main (life) Problem and set a medium-term (6–12 months) Goal (P&G). The output of these assessments is a set of issues documented on the care plan, which the veteran and HP agree will require their combined action over the following 12 months. At follow-up visits the HP monitors the outcomes of the care plan using the PIH and P&G scores, assisting the veteran to achieve his/her goals using motivational and problem-solving approaches and assisting with coordination and navigation of the health system (FHBHRU, 2011).
Alcohol Practice Guidelines (Pead et al., 2005) and self-help materials such as The Right Mix—Your Health and Alcohol included a booklet and materials that provided information on how to measure the amount of alcohol consumed, and steps to reduce alcohol use.
SCDSMP: The aim of the SCDSMP (Stanford School of Medicine, 2011) is to build the person’s self-efficacy to perform the tasks of role, disease and emotional management. The course is delivered in a 6-week group format conducted weekly over 2.5 hours. The SCDSMP teaches skills in problem-solving, decision-making, resource utilisation, managing the patient–provider partnership, action planning and emotional management. The course is led by peers or health professionals who receive 4 days of training.
Usual care
Usual care was available from public and private medical and mental health services, hospitals, GPs, Drug and Alcohol Services of South Australia, Alcoholics Anonymous, and VVCS. Services provided included crisis intervention, alcohol-related education and counselling, pharmacological interventions, and cognitive behavioural and group programs (e.g. PTSD, anger, depression and relationship management). Both intervention and control groups were able to access these services, with the intervention group identifying the services through the care planning process.
Outcome measures
Baseline age, sex, marital status, education, employment, self-reported co-morbid physical conditions and psychiatrist-diagnosed mental disorders diagnosed by the independent psychiatrist were recorded.
Alcohol Use Disorders Identification Test (AUDIT), a measure of hazardous and harmful alcohol consumption. The AUDIT is a self-report, non-diagnostic, 10-item questionnaire where final scores range from 0: abstainer, < 8: low-risk alcohol use, ≥ 8: risky or harmful alcohol use, ≥ 13: alcohol dependence is likely. The scale has specificities and sensitivities superior to other self-report screening measures and good test–retest reliability and internal consistency (Hawthorne et al., 2004; Reinert and Allen, 2002).
Assessment of Quality of Life (AQoL) is an Australian-developed, self-report, health-related quality of life instrument consisting of 15 questions, 12 of which contribute to a utility index covering elements of independent living, social relationships, physical senses and psychological well-being. Validation studies of the AQoL report excellent psychometric properties (Hawthorne and Osborne, 2005; Hawthorne et al., 1999).
Hospital Anxiety and Depression Scale (HADS) is a self-report, 14-item, self-assessment instrument comprising of two subscales for detecting states of depression and anxiety (Bjelland et al., 2002; Hawthorne et al., 2004).
Post-Traumatic Stress Disorder checklist – Military (PCL-M) version is a self-report questionnaire based on the Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R) symptoms of PTSD (Hawthorne et al., 2004; Weathers et al., 2001).
Dimensions of Anger Reactions Scale (DARS) is a self-report measure of anger directed towards others. Previous studies have indicated DARS is a psychometrically strong measure, and potentially useful for the evaluation of anger in PTSD (Hawthorne et al., 2004).
Abbreviated Dyadic Adjustment Scale (ADAS) is a self-report measure of marital/cohabiting relationships (Hawthorne et al., 2004; Sharpley and Rogers, 1984; Spanier, 1976).
Partners in Health (PIH) scale is a self-report, 14-item questionnaire which assesses six principles or attributes of the person’s self-management which are based on the Centre for Health Advancement definition of self-management (Battersby et al., 2003). The PIH total score was used in the intervention group to measure change in self-management over time. The 12-item version has been shown to have good internal consistency and construct validity (Petkov et al., 2010).
The Problems and Goals (P&G) approach is derived from behavioural psychotherapy (Fox and Conroy, 2000; Richards and McDonal, 1990), with the problem most important to the veteran and medium-term (6–12 month) goal statements developed collaboratively with the veteran using a semi-structured interview.
The independent psychiatrists used the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (American Psychiatric Association, 2000) to identify psychiatric diagnoses, and the Clinical Global Impressions (CGI) of change questionnaire (National Institute of Mental Health, 1970) to measure overall changes in severity of illness and global improvement.
Sample size and statistical analysis
Calculation of sample size was based on the AUDIT as the primary outcome measure using data from a previous Australian study that showed a mean (SD) AUDIT score of 13.96 (10.41) in Vietnam veterans (Evans et al., 2003). To attain 80% power for a two-sided alternative hypothesis using a t-test to compare the two treatment groups at follow-up, we required 138 participants (69 per group) to detect a mean difference of five units with medium effect size. Accounting for an attrition rate of 10% would bring the total sample size required to 152.
A between-group comparison of the intervention group and control group was performed for the 9-month intervention period. Data were analysed for the two periods of the study: baseline to 9 months (intervention period), and 9 months to 18 months (intervention group follow-up). Some intervention participants who entered the study towards the end of the recruitment period were unable to complete 12 or 18 months of follow-up. All statistical analyses were conducted using Stata 10.0 (Stata Statistical Software, College Station, TX, USA). Both intent-to-treat (ITT) and as-treated (AT) analyses were performed. Where results did not differ between the two methods; only the ITT results are presented. A Type 1 error rate of alpha = 0.05 was used in all analyses to test for statistical significance.
The AUDIT and AQoL measures were collected at baseline, 3, 6 and 9 months for both groups and follow-up at 12 and 18 months for the intervention group. The PIH measures were collected at baseline, 9 and 18 months for the intervention group. Linear mixed modelling (LMM) was used to quantify change over time for these repeated measures with more than two time points. Covariates for AUDIT and AQoL were treatment group, baseline outcome value, time in continuous form, and a time by group interaction term. A quadratic term for time was also tested to allow for potential non-linear effects where rates of change in outcome measures slowed down over time with a levelling-off effect. LMM takes into account the inter-individual differences in intra-individual change with repeated responses and uses all the available data on each subject (West et al., 2007).
The PTSD, HADS, DARS and ADAS measures were collected at baseline and 9 months for both groups and at a follow-up of 18 months for the intervention group. An analysis of covariance (ANCOVA) was performed to compare outcomes at 9 months between the two groups. To check for potential bias of available data, missing values were imputed using best-subset regression. As results using the marginally larger imputed samples did not differ from those of the available data, non-imputed measures were used in the final models. Effect sizes were calculated for within-group changes between baseline and 9 months for AUDIT, AQoL, PTSD, HADS, DARS and ADAS outcome measures using paired sample t-tests and Cohen’s d (Dunlap et al., 1996; Matthey, 1998).
To assess the effects on alcohol dependence at 9-month follow-up when adjusting for baseline, we used a generalised linear model where outcome was distributed as a binomial. Findings are reported as risk ratios to enable a more clinically meaningful interpretation. To assess for change in rates of diagnosis in the intervention group from baseline and 9 months to 18 months, an exact symmetry test was used for each 2 × 2 contingency table. The CGI ratings at 9 months were compared between groups using a Mann–Whitney test to calculate an effect size and precision (95% confidence interval).
Results
Recruitment and baseline results
The flow of participants through each stage of the study is presented in Figure 1. Of the 77 veterans enrolled and consented into the study, 46 commenced the intervention protocol and 31 commenced the control protocol. Intervention group participants and their partners were also invited to participate in the SCDSMP course. Twenty-two (48%) veterans and 15 of their partners chose to participate. Baseline characteristics for intervention and usual care participants are presented in Table 1.
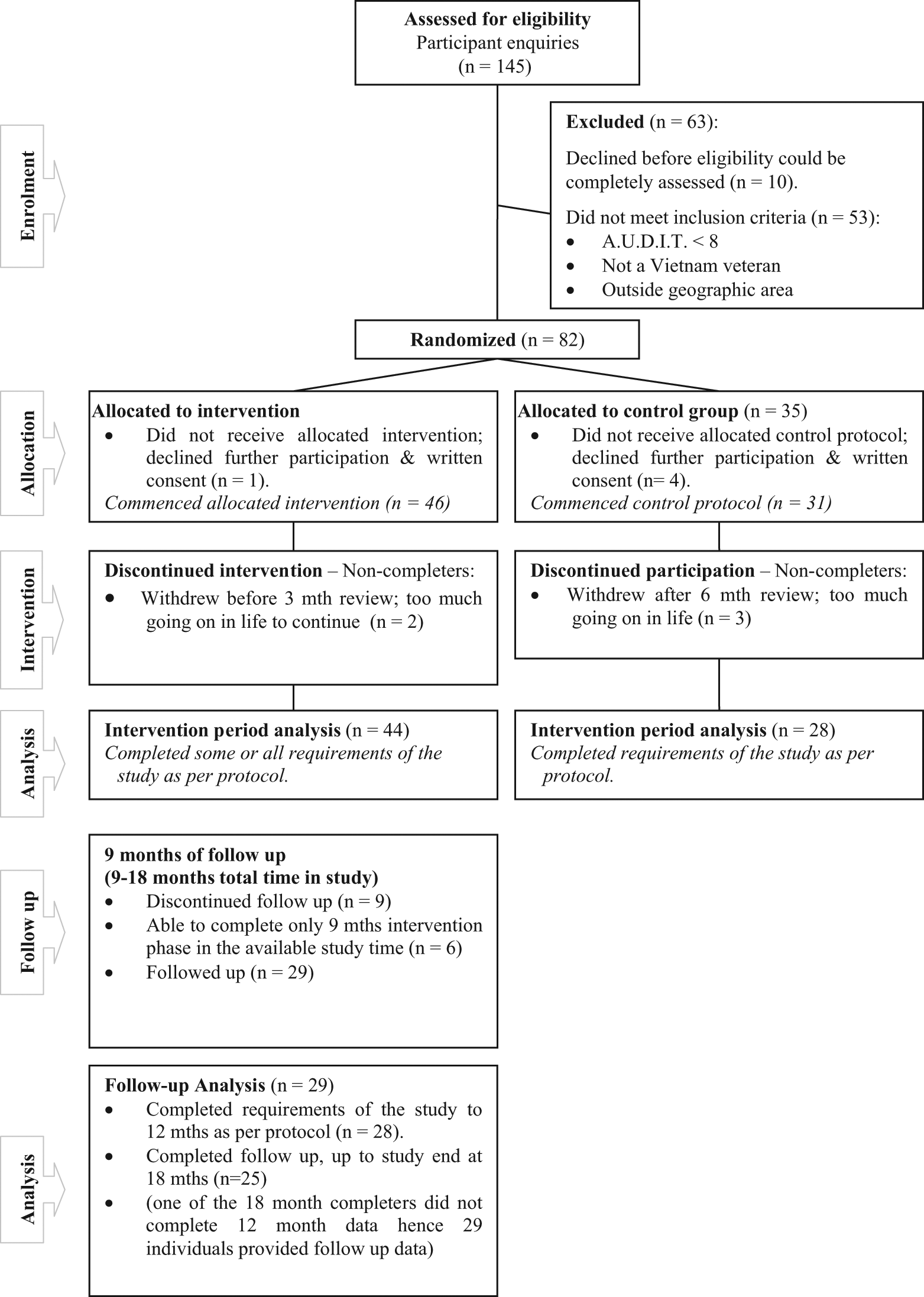
Participant flow chart: RCT analysis of intervention and control groups from baseline to 9 months and follow-up analysis of intervention group from baseline to 18 months. (RCT: randomised controlled trial.)
Baseline characteristics for participants in the control and intervention groups.
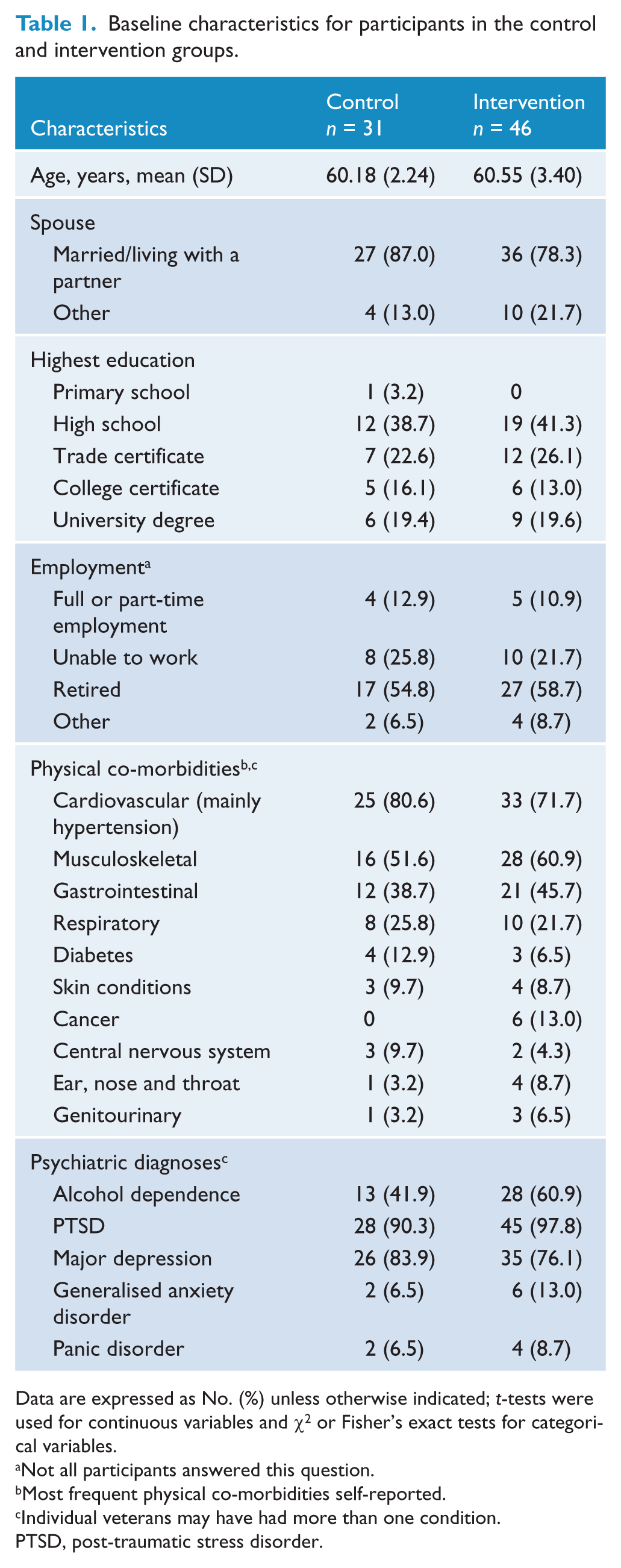
Data are expressed as No. (%) unless otherwise indicated; t-tests were used for continuous variables and χ2 or Fisher’s exact tests for categorical variables.
Not all participants answered this question.
Most frequent physical co-morbidities self-reported.
Individual veterans may have had more than one condition.
PTSD, post-traumatic stress disorder.
AUDIT and DSM-IV differences between and within groups
There was a significant group by time interaction for the primary outcome AUDIT scores where the intervention group decreased (improved) significantly more than the control group by, on average, 0.32 for every additional month from baseline to 9 months (95% CI −0.62 to −0.02; p = 0.039) when adjusting for baseline scores. Figure 2 presents observed AUDIT means and 95% confidence intervals for the ITT analysis. Within-group analyses showed a significant reduction (improvement) with a large effect size (d = 0.90) for the intervention group and an improvement with a medium effect size (d = 0.74) for the control group (Table 2).
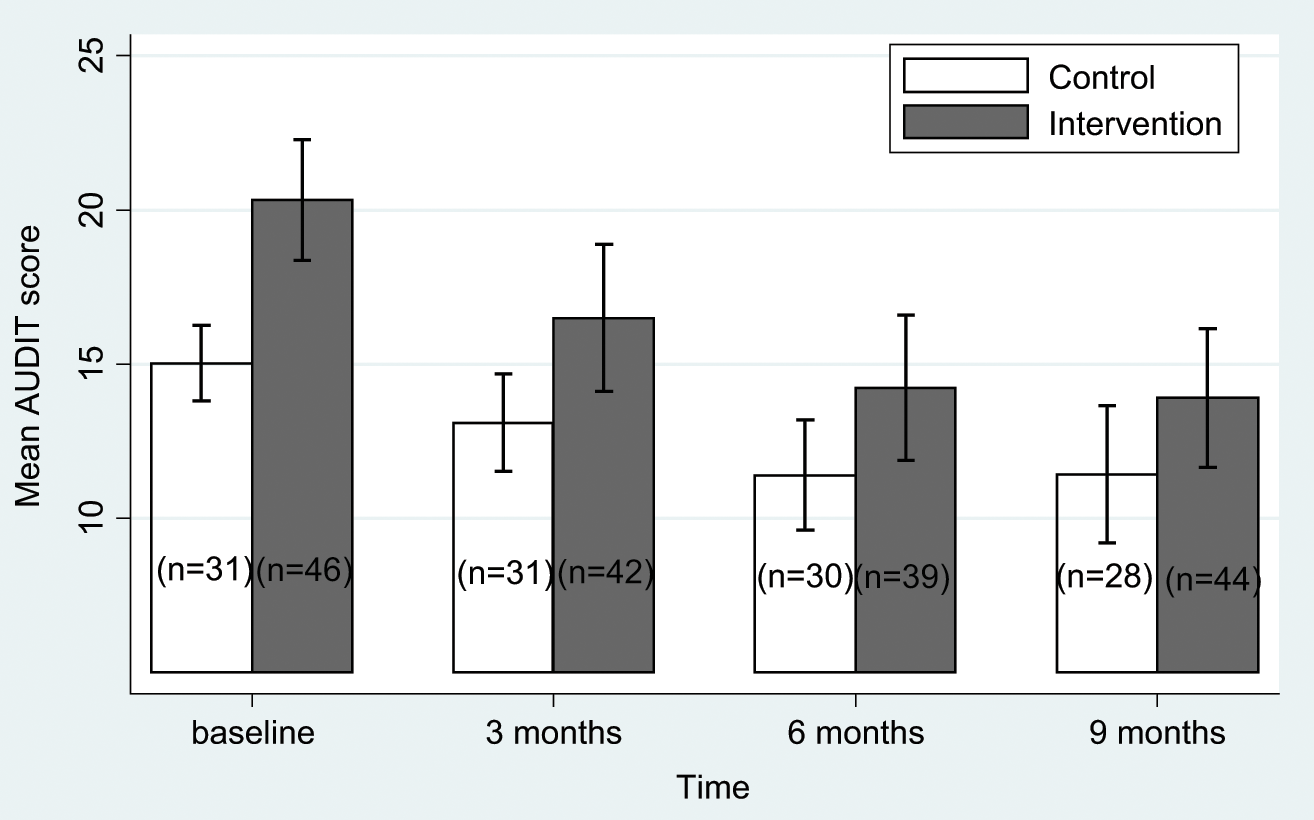
Intent-to-treat analysis: mean AUDIT scores with 95% confidence intervals as a function of treatment group. Lower scores indicate improvement (i.e. a reduction) in alcohol hazardous drinking or dependence. (AUDIT: Alcohol Use Disorders Identification Test.)
Analysis of covariance examining changes on measures at baseline and 9 months and effect sizes (d) for intervention and control groups a .
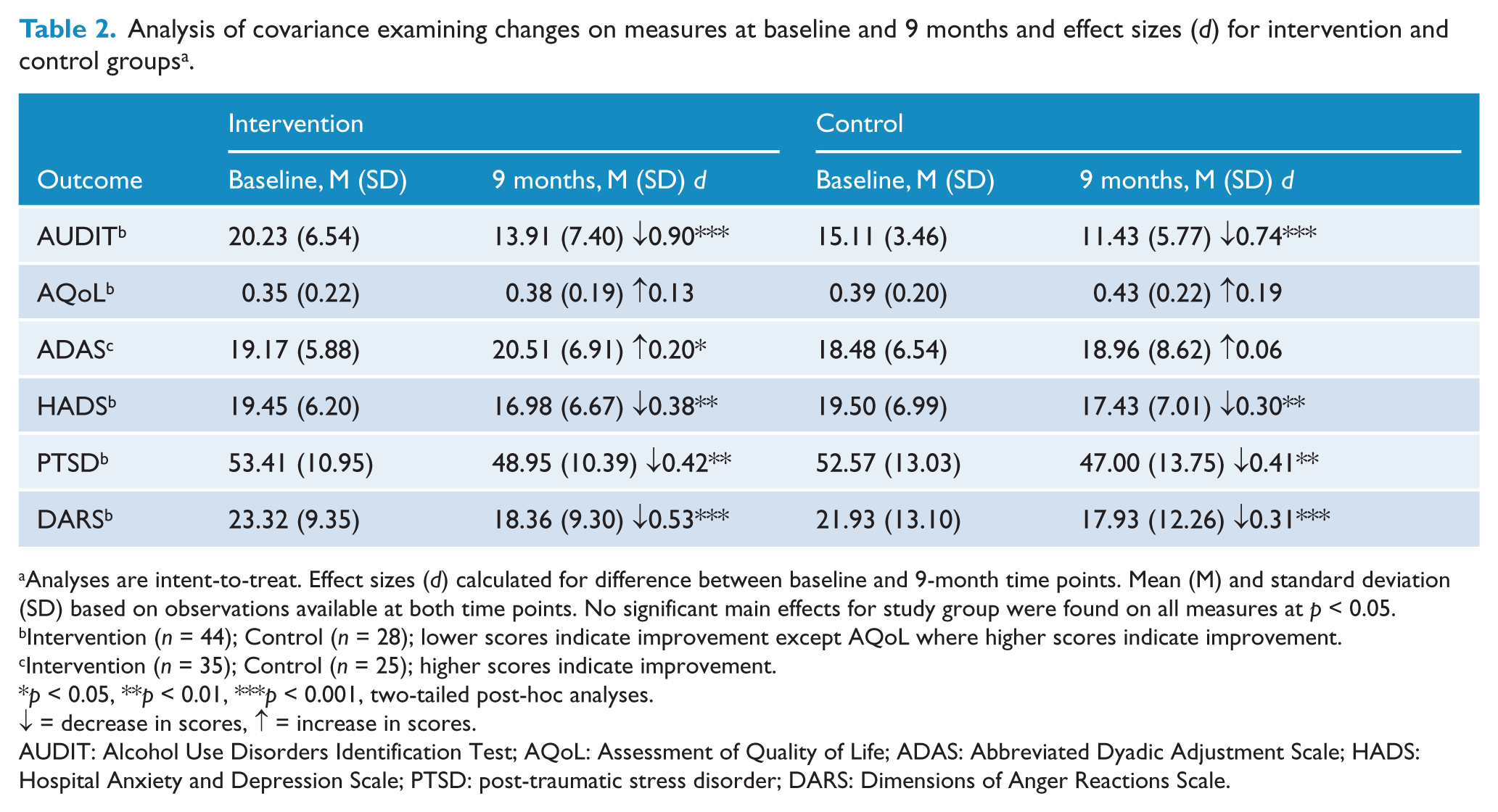
Analyses are intent-to-treat. Effect sizes (d) calculated for difference between baseline and 9-month time points. Mean (M) and standard deviation (SD) based on observations available at both time points. No significant main effects for study group were found on all measures at p < 0.05.
Intervention (n = 44); Control (n = 28); lower scores indicate improvement except AQoL where higher scores indicate improvement.
Intervention (n = 35); Control (n = 25); higher scores indicate improvement.
p < 0.05, **p < 0.01, ***p < 0.001, two-tailed post-hoc analyses.
↓ = decrease in scores, ↑ = increase in scores.
AUDIT: Alcohol Use Disorders Identification Test; AQoL: Assessment of Quality of Life; ADAS: Abbreviated Dyadic Adjustment Scale; HADS: Hospital Anxiety and Depression Scale; PTSD: post-traumatic stress disorder; DARS: Dimensions of Anger Reactions Scale.
Results for DSM-IV diagnosis of alcohol dependence using a generalised linear model showed that control group participants, after adjusting for baseline, had 1.46 times the risk of alcohol dependence at the 9-month follow-up than intervention group participants (95% CI 1.04–2.04; p = 0.027). In the intervention group, alcohol dependence decreased over time with 25 out of 39 (64%) of the veterans identified as alcohol dependent at baseline, significantly decreasing to 16 out of 39 (41%) at 9 months (p = 0.004). In the control group, there was no change in alcohol dependence from baseline to 9 months, with 13 out of 27 (48%) identified as alcohol dependent at both time points.
Differences between and within groups for secondary outcome measures
After adjusting for baseline scores there was no significant difference between intervention and control group in AQoL score changes over time (p = 0.14). Findings from an ANCOVA for secondary outcome measures conducted at baseline and 9 months are presented in Table 2. There were no significant differences between intervention and control groups on all outcome measures at 9 months when controlling for baseline scores.
Within-group analyses were conducted for secondary measures to assess direction and magnitude of change, respectively, from baseline to 9 months (Table 2). There were significant effects for time in both groups with a reduction (improvement) on HADS, PTSD and DARS scores. There was a significant increase (improvement) with a small effect size on the ADAS for the treatment group but not the control group. A medium effect size was found for the DARS in the intervention group and small effect sizes for the remainder of measures with significant main effects for time.
For CGI scores at 9 months the likelihood of a veteran assigned to the intervention group having a better outcome than a veteran assigned to the usual care group was assessed using a Mann–Whitney test. For CGI-S (severity of illness scale) there was no significant difference between the two groups (p = 0.894). For CGI-I (improvement scale) the probability of a veteran in the intervention group having a lower score (improvement) than the control group at 9 months was 73.9% (95% CI: 62% to 85.7%; p = 0.001).
Follow-up results for the intervention group
Follow-up periods ranged from 0 to 9 months (9–18 months = total time in study) for the intervention group, depending on time of recruitment into the study. There was a significant decrease (improvement) for the primary outcome AUDIT scores of, on average, 0.98 for every additional month for both intervention period and follow-up at 12 and 18 months (95% CI −1.24 to −0.73; p < 0.001). For secondary outcome measure AQoL, there was no significant change in scores for the intervention period and follow-up at 12 and 18 months (p = 0.599). Within-group analyses indicated a significant effect for time, with an improvement for AUDIT, AQoL, HADS and PTSD scores between baseline and 18 months (Table 3). For DSM-IV diagnosis of alcohol dependence there was a further non-significant decrease from 16 out of 39 (41%) at 9 months to 8 out of 23 (35%) at 18 months (p = 1.00).
Effect sizes (d) for differences between baseline and 18 months and between 9 months and 18 months intervention group scores.
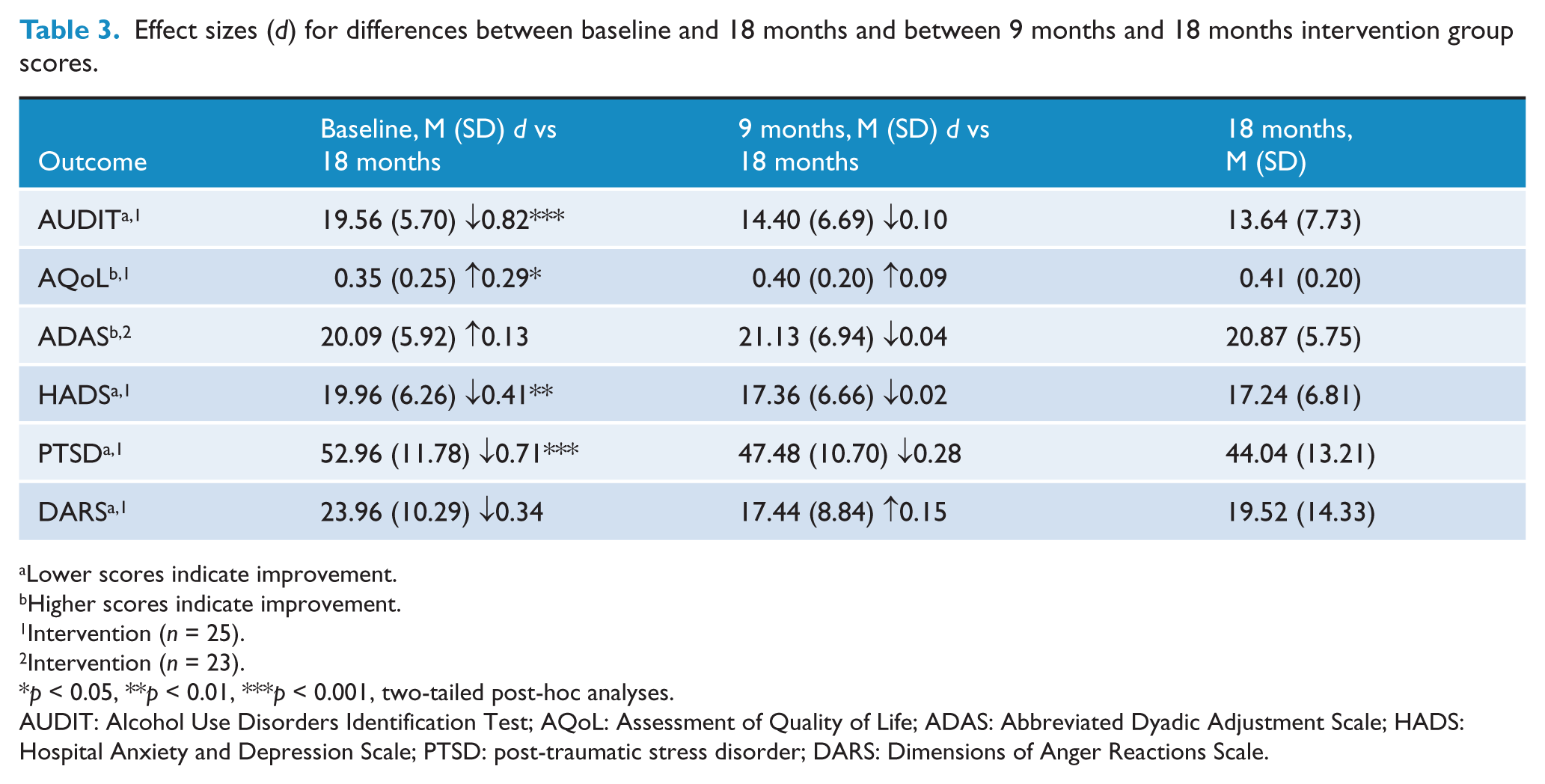
Lower scores indicate improvement.
Higher scores indicate improvement.
Intervention (n = 25).
Intervention (n = 23).
p < 0.05, **p < 0.01, ***p < 0.001, two-tailed post-hoc analyses.
AUDIT: Alcohol Use Disorders Identification Test; AQoL: Assessment of Quality of Life; ADAS: Abbreviated Dyadic Adjustment Scale; HADS: Hospital Anxiety and Depression Scale; PTSD: post-traumatic stress disorder; DARS: Dimensions of Anger Reactions Scale.
Results from Flinders Program self-management measures
Results for total PIH scores showed a statistically significant decrease (improvement) at 9 months of 12.1 (95% CI: −15.1 to −9.0) and 18 months of 13.4 (95% CI: −17.0 to −9.80) when compared to baseline (p < 0.001). There was no significant improvement for 9 months versus 18 months (p = 0.469).
Results from the P&G assessment showed that from baseline to 9 months a total of 47 main life problems were identified by the intervention participants, with the most frequent being related to their psychological condition (46.8%; n = 22/47), followed by alcohol use (27.7%; n = 13/47) and relationships (12.8%; n = 6/47). A total number of 71 goals were identified, with the most frequent being related to alcohol use (28.2%; n = 20/71), relationships (16.9%; n = 12/71), fitness/exercise (15.7%; n = 11/71) and psychological (14.1%; n = 10/71).
Of the problems identified at first visit, 87.5% (n = 35) of veterans showed a significant reduction in severity from baseline to 9 months (p < 0.001), with 51.3% (n = 20) considering these problems solved at the end of the intervention period. Of the goals developed at first visit, 77.5% of veterans showed significant progress in achieving their goals from baseline to 9 months (p< 0.001), with 65% of goals being achieved at the end of the intervention period.
The cost of nursing time to conduct the FP over the 9 months in the intervention group was AUD$195 (SD AUD$52), associated with an average of 4 hours and 38 minutes (SD 1 hour 16 minutes) per veteran.
Discussion
This is the first RCT to be undertaken with Australian Vietnam veterans using a person-centred, generic, self-management care planning intervention to address issues related to alcohol misuse and co-morbid psychiatric and medical conditions. Findings using mixed modelling showed a significant improvement in the intervention group compared to the control group in the primary outcome AUDIT scores. This finding was supported by a reduction in the diagnosis of alcohol dependence in the intervention group from baseline to 9 months (64% to 41%; p = 0.004), which was maintained to 18 months (41% to 35%). Effect sizes showed there were no significant improvements in quality of life for either the intervention or control group over the 9 months; however, global improvement was greater in the intervention group than in the control group (p = 0.001). Although there was no difference between groups, there was a clinically significant improvement within both groups for HADS, PTSD and DARS, with a clinically significant improvement within the intervention group only for ADAS.
Enhancing motivation by addressing veteran-identified self-management tasks and problems and goals
With a complex intervention with multiple components we cannot determine which element or combination resulted in the changes. This reflects the real world of health care in which it is artificial to separate out interventions. Most veterans in the intervention group had previously accessed evidence-based usual care services (i.e. PTSD and anger groups, counselling, and alcohol and medical management). We can speculate that the FP had a major additional contribution as a priming process to initiate change and build confidence in the veteran by identifying his/her priorities and helping him/her to take responsibility for the actions required. In this way, success was shared and self-management supported. The motivational process began with assessment of the veteran’s self-management (knowledge of condition and treatment, decision making, adherence, coping, symptom and lifestyle management), not just of the medical or psychiatric problems but also the psychosocial issues using the PIH. Motivation was enhanced with the collaborative identification of issues to be addressed on the care plan through the C&R interview. The veteran then seemed more motivated to engage with other interventions when the P&G process identified life problems, set goals and made the commitment to action described on the care plan. Changes in self-management were reflected in improved PIH scores (p < 0.001). We can speculate that ‘changes in self-management’ was the mechanism by which changes in alcohol and other psychological variables occurred.
A number of systematic reviews have investigated the effect of case management and intensive case management (ICM) (with the case manager having no more than 20 cases) on people with mental health conditions and alcohol and other substance use. In comparison to standard care, case management and ICM were found to reduce hospitalisation, increase retention in care, and globally improve social functioning; however, it is unclear whether ICM has a larger degree of effect than less formal case management (Dieterich et al., 2010). Furthermore, there is no conclusive evidence that case management of this kind reduces drug and alcohol use (Hesse et al., 2007).
The finding in this study, that there was significant reduction in veteran-identified problems and significant progress towards achieving the veteran’s goals suggests that the problem and goal being prioritised ultimately led to changes in the target clinical alcohol problem. A critical element seemed to be the relationship established through use of the RN’s own skills but also through the FP itself, through use of the RN’s own skills, which provides a non-judgemental and structured process to explore complex issues. This was no doubt assisted by the nurse who acted as coach and educator. What kept veterans engaged was their increased awareness of the relationship between their personal and relationship issues and their use of alcohol, and having HPs who sought and valued a real, rather than rhetoric partnership with them. Once this trust in the partnership was developed, veterans were open to additional alcohol-related education and attending hospital and community services to address their problems. The combination of self-management support and disease or condition management was the key to sustainable outcomes. Consequently, the FP had a positive impact on alcohol-related behaviours. These results suggest that the FP is a powerful motivator for change.
Person-centred care and adherence to chronic condition management
Engaging Vietnam veterans generally is not an easy task because many have PTSD, anxiety and depression, and trust issues related to institutional health care (Dunt, 2009). As a result, veterans may commence interventions and then disappear prior to completion or follow-up. The FP, with its absolute commitment to working in partnership with the veteran, addressing their health issues, setting specific, measurable, action-oriented goals, and then monitoring progress towards achieving these over the 9-month cycle of care, was shown to be a successful model for engaging, retaining and motivating this cohort of veterans towards a decrease in risky alcohol behaviours. Of the 46 veterans commencing the FP in the intervention group, 40 completed all of the 9-month intervention and assessment requirements, and 29 of a possible 38 were available for follow-up to 18 months, a low attrition rate for Vietnam veterans engaging with health services.
Implementing the Flinders Program
The components of chronic condition management utilised in this program consisted of: self-management assessment and care planning; medical and evidence-based management; monitoring, review and motivational support; self-management education; community services; coordination, and outcome measurement which is fed back to the client and workers. The FP can be commenced during discharge planning in private and public acute care services or it can be commenced in community settings such as the VVCS and general medical and mental health services. The Enhanced Primary Care, Chronic Disease and Mental Health Medical Benefits Scheme items can be used to conduct the Flinders self-management care planning process. While the research nurses in this study were general registered nurses who delivered the FP, a variety of HPs have been trained to deliver the FP, in a variety of settings (Battersby et al., 2001, 2003, 2007a, 2007b, 2008; Battersby and SA HealthPlus team, 2005; Crotty et al., 2009; General Practice Queensland, 2008; Harvey et al., 2008; Lawn et al., 2007, 2009; NSW Department of Health, 2006; Rowett et al., 2005; Urakalo et al., 2004). The average nursing cost of AUD$195 per veteran over the 9-month period demonstrates that using the FP is inexpensive and can be funded under the Enhanced Primary Care (EPC) item numbers. General practitioners are now funded to deliver coordinated care for veterans using the Flinders Program as part of the recently commenced Department of Veterans’ Affairs ‘Coordinated Veterans’ Care Program’ (Department of Veterans’ Affairs, 2011).
Limitations
Of 145 individuals who contacted the study, 63 were excluded and 82 agreed to enrol, just over half of the target sample size. Shortfall in recruitment numbers was in part due to funding, which limited the recruitment period to 15 months, and the opt-in recruitment approach, chosen because of concerns that veterans may be sensitive to issues of confidentiality if they were approached directly by the researchers. Further, should veterans have become aware that this study was funded by the DVA it may have created fears that personal information could adversely affect their entitlements. The possibility of being randomised to the control group may have also impacted on recruitment. Multiple recruitment methods were attempted, with the most successful being direct recommendation by the veterans’ treating specialist or GP. The reduced recruitment numbers meant that the study was underpowered to detect change in a number of measures; however, the primary outcome AUDIT measure showed significant change indicating the intervention has high potency in affecting alcohol use. It was notable that the control group improved in most outcome measures. This would be expected in an ‘opt-in study’ where the veterans had to be seeking help for their alcohol problems to contact the study office and combined with the ‘Hawthorne effect’ may have also influenced the ability of the intervention to show benefit over and above the control group. Use of the AUDIT was not supplemented by more objective measures of alcohol use; however, these ratings were supported by DSM-IV diagnosis and CGI scores based on psychiatric assessments.
One of the disadvantages of using the complete randomisation method is the possibility that at any point in the randomisation there could be an imbalance between the intervention and control groups. In this study, an imbalance did occur as randomisation was based on 200 participants with only 82 joining the study. The strict eligibility criteria of an AUDIT score ≥ 8 and a chronic condition, along with high ineligibility rates, resulted in a smaller than predicted sample size; hence by chance, at the point recruitment ceased, there was an imbalance in the intervention/control ratio. To account for the potential influence of this imbalance on treatment effect estimates, the primary statistical analyses were fully adjusted for baseline scores. An alternative randomisation method with varying block sizes to protect concealment would have ensured nearly equal group sizes.
Potential bias in the study could have resulted from the lack of blinded subjects and those administering the intervention and mostly self-reported measures; however, the questionnaire data were collected and entered by administrative staff who were blind to group allocation and statistical analysis was performed by a statistician blind to allocation. The independent psychiatrists were not blind to group allocation and their global ratings could have been influenced by this knowledge; however, their severity ratings indicated no difference between the two groups whilst the improvement ratings were clearly greater in the intervention group.
Conclusion
The FP has been used across a range of chronic conditions and diseases by HPs from a variety of disciplines and health services, working in partnership with the patient as the focus of care. It has now been shown to be effective in improving alcohol and related health outcomes in Vietnam veterans with risky alcohol behaviours and chronic psychiatric conditions. This study has demonstrated that the FP process of care planning based on self-management assessment engages the veteran in their own care, determines their medical and psychosocial needs, and provides a structured framework for delivering case management and coordinated care for people with chronic and complex conditions. This clinical approach has the potential to bridge the gap between physical and mental health service delivery in Australia.
Footnotes
Acknowledgements
The authors would like to thank the Department of Veterans’ Affairs officers Elaine Waddell and Jon Wauer for their support during the project. Our thanks go to the veterans, their partners, general practitioners, general practice staff, psychiatrists, the steering committee and project officers Amanda Carne and Anthea Williams for their valuable contribution to the study. For their contribution in assisting in the recruitment of Vietnam veterans, we thank the following organisations: the Adelaide metropolitan Divisions of General Practice (Southern, Eastern and Central, and Western divisions), Repatriation General Hospital, VVCS, Vietnam Veterans Association SA Branch, Vietnam Veterans Federation SA Branch, RSL, and Partners of Vietnam Veterans. We gratefully acknowledge the research nurses Jill Western and Barbara Oerman, and group facilitators Sarah Blunden and Pauline Kelly, along with peer facilitators Bert Henstridge, Ian Gully and Jim Fisher in leading the Stanford courses. In addition, we thank the independent psychiatrists Michael Warhurst, Yasna Petrunic and Conrad Newman for their valuable contribution to the project.
Funding
The study was funded by the Australian Department of Veterans’ Affairs.
Declaration of interest
As the developer of the Flinders Program Professor Battersby has a potential conflict of interest. He has no commercial interests in the Flinders Program.