
Abstract
Objective:
People with psychiatric diseases have a severely increased risk for physical morbidity and premature death from physical diseases. The aims of the study were to investigate the occurrence of cardiovascular diseases (CVD), diabetes (DM) and obesity in schizophrenia and depression in three different geographical areas – Asia (Japan), Africa (Nigeria) and Western Europe (Switzerland, Germany and Denmark) – and to search for possible transcultural differences in these correlations, which would also reflect the differences between low-income areas in Africa (Nigeria) and high-income areas in Europe and Japan.
Method:
Patients with International Classification of Diseases (ICD-10) F2 diseases (schizophrenia spectrum disorders) and F3 diseases (affective disorders) admitted to one Nigerian, one Japanese, two Swiss, two German and six Danish centres during 1 year were included. Physical diseases in accordance with ICD-10 were also registered. Psychiatric and physical comorbidity were calculated and standardized rate ratio incidences of background populations were our primary measures.
Results:
Incidence rate ratios were increased for both CVD, DM and overweight in both F2 and F3 in all cultures (Western Europe, Nigeria and Japan) within the same ranges (however, the Japanese results should be interpreted conservatively owing to the limited sample size). Overweight among the mentally ill were marked in Nigeria. A parallelism of the incidence of overweight, CVD and diabetes with the occurrence in background populations was seen and was most marked in overweight.
Conclusions:
Overweight, CVD and DM were increased in schizophrenia spectrum disorders and affective disorders in all three cultures investigated (Western Europe, Nigeria and Japan). Lifestyle diseases were also seen in Nigeria and Japan. The results from this study indicate that cultural background might be seen as an important factor in dealing with lifestyle diseases among people with a severe mental illness, as it is in the general population.
Keywords
Introduction
Since the publication of the Harris and Barraclough (1998) article 14 years ago, it has been common knowledge that physical illness is more common among patients with a psychiatric disorder than in the general population. In a review published in 1999, nearly 50% of psychiatric patients had a significant medical illness (Goldman, 1999). The mortality rate is also higher, with severe mental illness shortening the average life expectancy by 12–20 years (Goldman, 1999; Lambert et al., 1996; Simpson and Tsuang, 1996). Mortality is increased from both natural and unnatural causes in all major diagnostic groups (i.e. schizophrenia, depression and mania) (Simpson and Tsuang, 1996). The World Health Organization (WHO) annual reports describe individuals with severe mental illness as having a higher risk of serious infectious diseases, such as HIV and hepatitis B and C (Rosenberg et al., 2001). The aetiology of the excess of disease and mortality is multifactorial and may be caused by the mental disorder itself or the influence on daily life functions caused by the disorder (De Hert et al., 2011a; Fleischhacker et al., 2008; Harris and Barraclough, 1998). Medical comorbidity varies from dental problems and problems with eyesight, to obesity, arterial hypertension, heart disease and diabetes (Dixon et al., 1999).
Patients with schizophrenia have the highest rate of comorbid physical conditions, but many of these illnesses are misdiagnosed or undiagnosed (Goldman, 1999; Jeste et al., 1996). It is known that patients with a severe mental illness receiving treatment for a comorbid physical illness are under-represented in clinical settings, as found in the CATIE study and a European study covering 12 countries (De Hert et al., 2009a).
Schizophrenia is a life-shortening illness with a 20–30% shorter life expectancy than the general population and a mortality rate twofold higher (Fleischhacker et al., 2008; Goldman, 1999). Suicide and traumatic injuries are among the causes, but a high rate of undetermined causes of death is also found. A proportion of mortality in schizophrenia may also be associated with the side effects of antipsychotic medication (De Hert et al., 2009b; Ücok and Gaebel, 2008).
The diagnostic profile of physical illnesses reported for patients with schizophrenia is similar to the background population, but illnesses occur at a younger age to that reported for the general population who are, on average, 12 years older (Jeste et al., 1996). Poor physical health negatively influences the quality of life of individuals with schizophrenia (von Hausswolff-Juhlin et al., 2009). A large number of patients with schizophrenia is diagnosed with substance abuse, particularly cigarette smoking. Patients with first-episode psychoses use three to four times more substances than the general population and have an increased risk of physical illness associated with substance use (Mazzoncini et al., 2010). In addition, this group also has a high frequency of obesity and is more likely to develop non-insulin-dependent diabetes (NIDDM; type 2) (Fleischhacker et al., 2008; Goldman, 1999). With regard to treatment, there is an increased focus on the need for an awareness of the influence of antipsychotics on mortality rates – cardiac mortality, in particular (Correll and Nielsen, 2010; De Hert et al., 2011a, 2011b).
A high prevalence of physical illness has been reported, with 71% of comorbid cases reported in first-episode depression patients and 89% of comorbid physical conditions reported in recurrent depression cases (Geli et al., 2011).
Depression is suggested to be a risk factor for developing coronary heart disease independent of lifestyle factors (Janszky, 2007). Bipolar disorder-like depression has been found to be associated with an increased risk of metabolic syndrome, where both lifestyle and the disorder itself may account for premature mortality (Taylor and MacQueen, 2006). It has been found that mental stress in itself is a risk factor for developing cardiovascular disease (CVD) (Nippon DATA80 Research Group, 2006). Symptom severity in depression is associated positively with the prevalence of metabolic syndrome, aggravated independently by tricyclic antidepressant treatment (van Reedt Dortland et al., 2010).
Cultural diversity
Most studies of the distribution of comorbid conditions have been carried out in Western Europe and North America. However, some studies from developing countries suggest that cultural diversity may be important factors; for example, limited access to healthcare in some areas and risk factors related to traditional ways of living when comorbidity is considered (Harris and Barraclough, 1998; Leucht et al., 2007). Cultural background may also reflect differences in income level as an important predictor for the risk of physical illness and the possibility of receiving treatment, particularly when suffering from a mental illness (Craig and Mindell, 2008).
Ethnic groups are composed of people who may or may not share the same ethnicity but do share common cultural characteristics, including history, beliefs, values, food and entertainment preferences, religion and language (Bhugra and Becker, 2005; Bhugra et al., 2011). Those entities composing an ethnic group are important factors when analysing the epidemics of a disease and discussing the influence of lifestyle on the course of a physical or mental disease (Mirzaei et al., 2009). As cultural habits change over a long period of time, these may influence the pattern of disease from one period of time to another – which is known as epidemiological transition (Gillum, 1996). This phenomenon is also recognizable in developing countries but over a shorter period of time, such as the sub-Saharan countries where increased levels of acculturation, urbanization and affluence might influence the pattern of diseases to change from communicable diseases to non-communicable diseases (e.g. CVD) through a population’s adaption to another lifestyle (in particular, the shift from carbohydrates being the main food stuff to a high intake of saturated fat) (Yano et al., 1978). As those conditions are to be taken into account when considering general health problems, they may be even more important in patients with mental disorders. There are some studies which show that the gap between people with severe mental illness and the general community with regard to mortality has worsened in recent decades, with the highest standard mortality rate found in developed countries. This may be explained by the decrease in mortality among the general population in developed countries (Saha et al., 2007).
Aims of the study
The aims of the study were to investigate the occurrence of CVD, diabetes and obesity in schizophrenia and depression in three different cultures – Asia (Japan), Africa (Nigeria) and Western Europe (Switzerland, Germany and Denmark) – and to explore possible transcultural differences in these correlations.
Materials and methods
The study was carried out during a 1-year period in mental healthcare centres in Denmark, Germany, Switzerland, Nigeria and Japan.
All individuals received into treatment over the period of investigation were invited. Those who were re-admitted were only included at their first admission in the 1-year study period. During the assessment interview and physical examination, the patients’ physical and mental health statuses were assessed according to the WHO International Classification of Diseases (ICD-10) (WHO, 1992). Patients were assessed again at discharge. If hospitalized for more than 3 months, a follow-up assessment was carried out after 3 months of hospitalization. The assessments were made according to routine clinical practice at the participating centres and treatment was administered as usual. Based on these findings, both psychiatric and somatic diagnoses were recorded accordingly. Diagnoses of mental disorders were made according to the ICD-10 criteria for ‘Schizophrenia and other psychotic disorders’ (F2) and ‘Affective disorders’, including depression and bipolar disorders (F3). Diagnoses of CVD and diabetes were made according to the ICD-10 criteria for ‘Heart failure’, ‘Ischemic heart disease’, ‘Angina pectoris’ (either present or was present earlier) and ‘Hypertension’, information for which was obtained from the patient files (which included a list of drugs) and during physical examinations and para-clinical tests, including the taking of blood samples, which was in accordance with ‘treatment as usual’. We also monitored the patients’ cultural backgrounds as being of ‘Local nationality’, ‘Western Europe/North America’, ‘Other areas’ and ‘Unknown’. The first of the centres began recruiting patients in 2003, while the last of the centres ended the inclusion of patients in 2005.
Statistical analysis
Initially, the prevalence rates of CVD, diabetes and overweight [body mass index (BMI) > 25] in individuals with either an F2 or F3 ICD-10 diagnosis were calculated for Denmark, Germany, Switzerland, Nigeria and Japan. The prevalence rate ratios were age-standardized directly by diagnosis and country, with the general age distribution of the corresponding country as standard. Finally, the prevalence ratios were calculated with 95% confidence intervals (CIs).
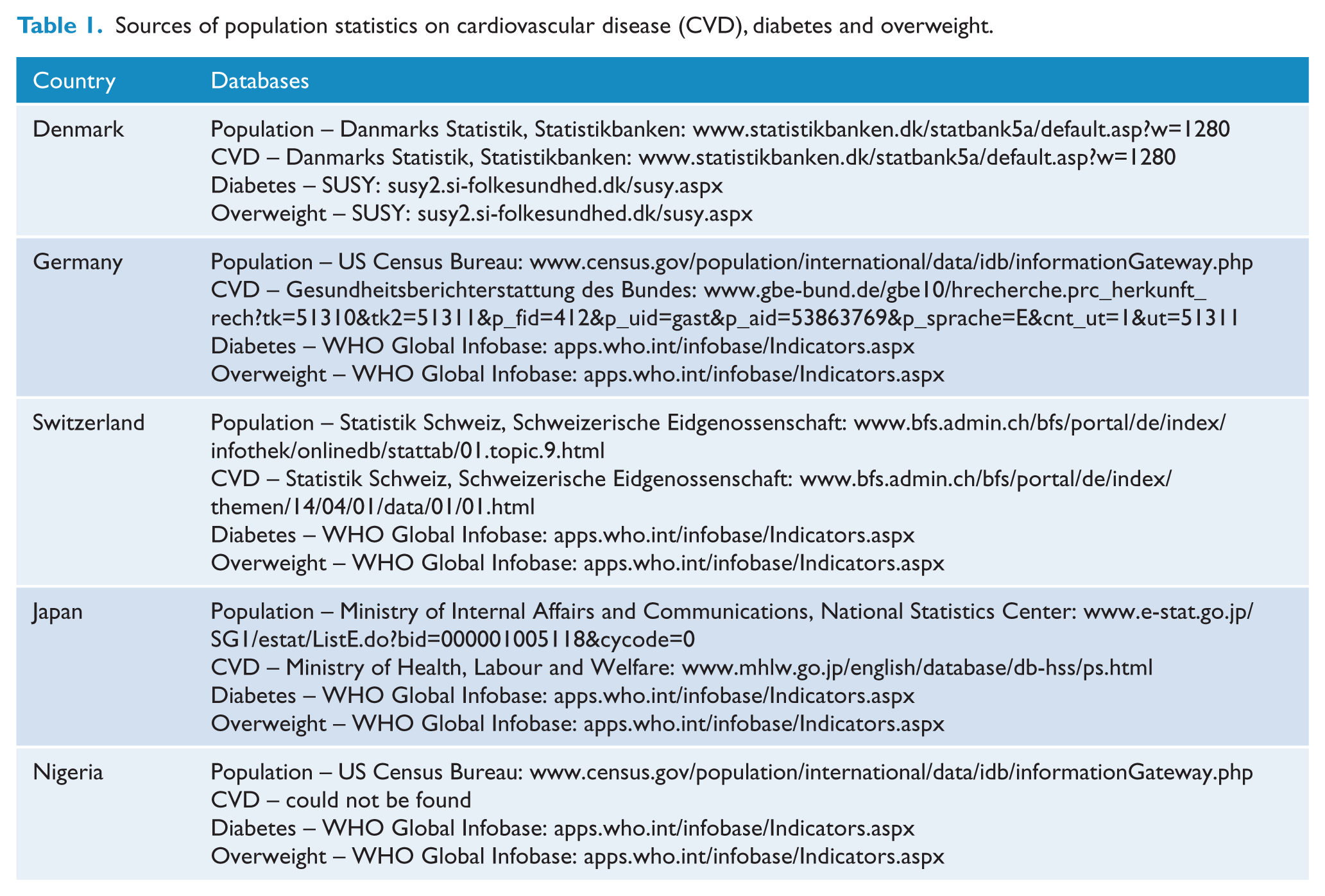
Populations and statistics on CVD, diabetes and overweight were obtained from the databases as shown in Table 1.
Sources of population statistics on cardiovascular disease (CVD), diabetes and overweight.
The study was approved by local science ethical committees. Their instructions for how patients should be included were followed. Owing to ethical reasons, data on those not participating could not be collected.
Results
Table 2 shows the participants distributed according to participating centre diagnoses (ICD-10 F2 and F3), the type of clinical setting and mean age.
Patients included through admission to treatment setting in 1 year.
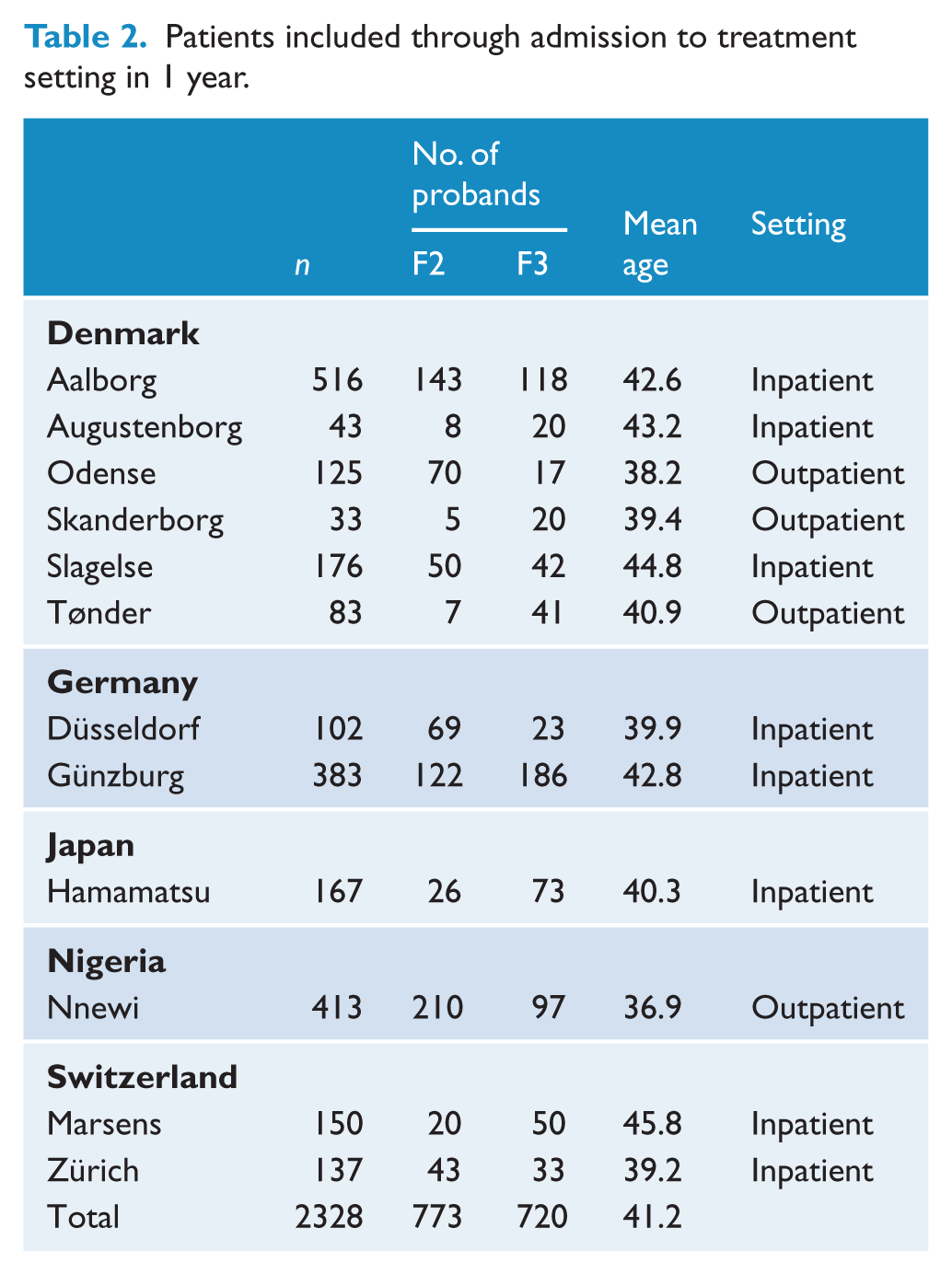
Figure 1 shows the prevalence of CVD in the general and F2 populations, where it can be seen that the prevalence of CVD is high in Japan. The rate ratio does not differ between the European centres, but is significantly higher in the Japanese centre. As Nigerian data for the general population are not available, the rate ratio cannot be calculated.
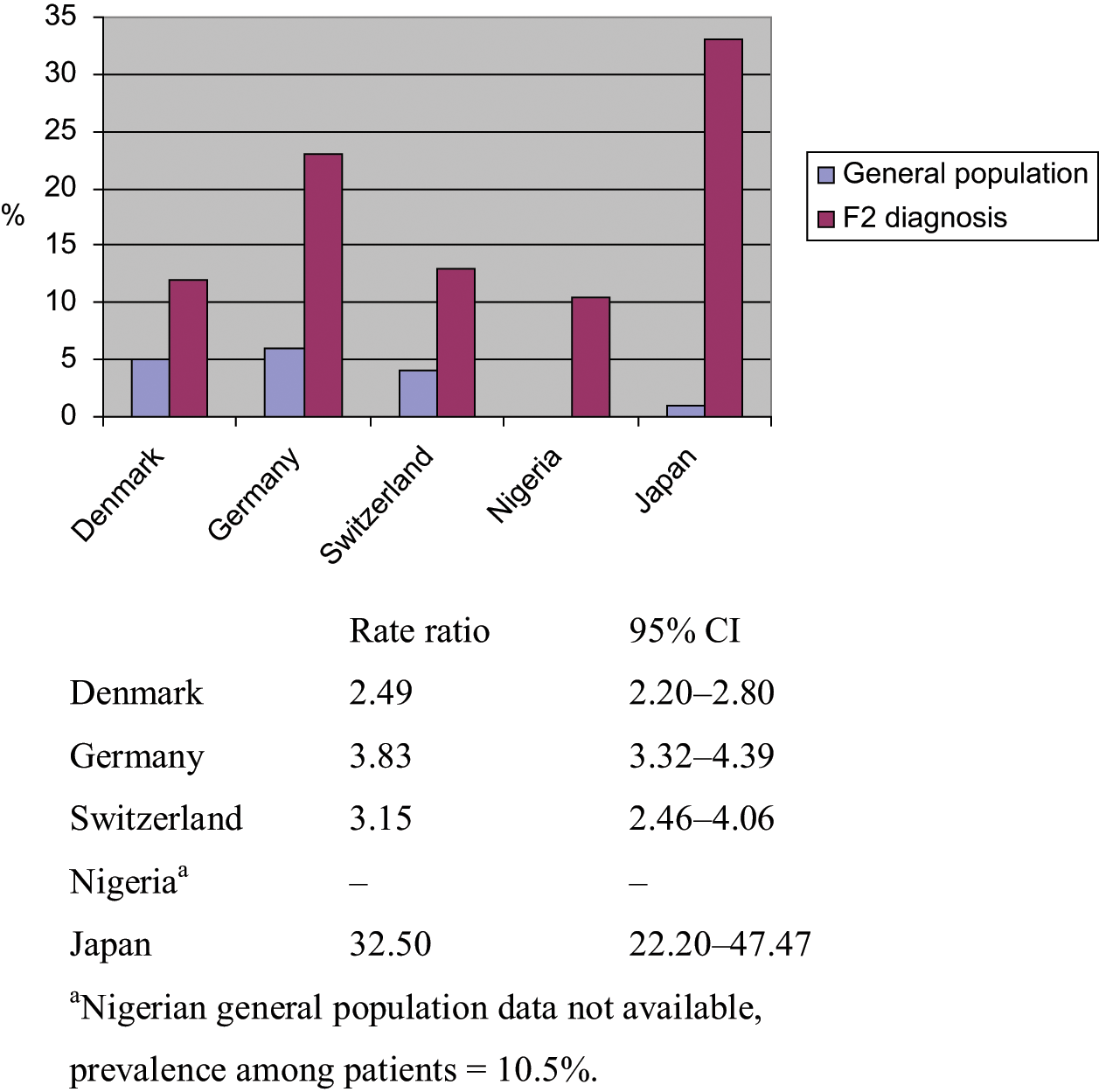
Standarized prevalence of CVD in diagnostic group F2.
The prevalence of diabetes in the general and F2 populations is shown in Figure 2. There is no significant difference between the three European and the African centres. Data were too few for the Japanese centre for performing a rate ratio. For the remaining centres, the rate ratios are within the same range.
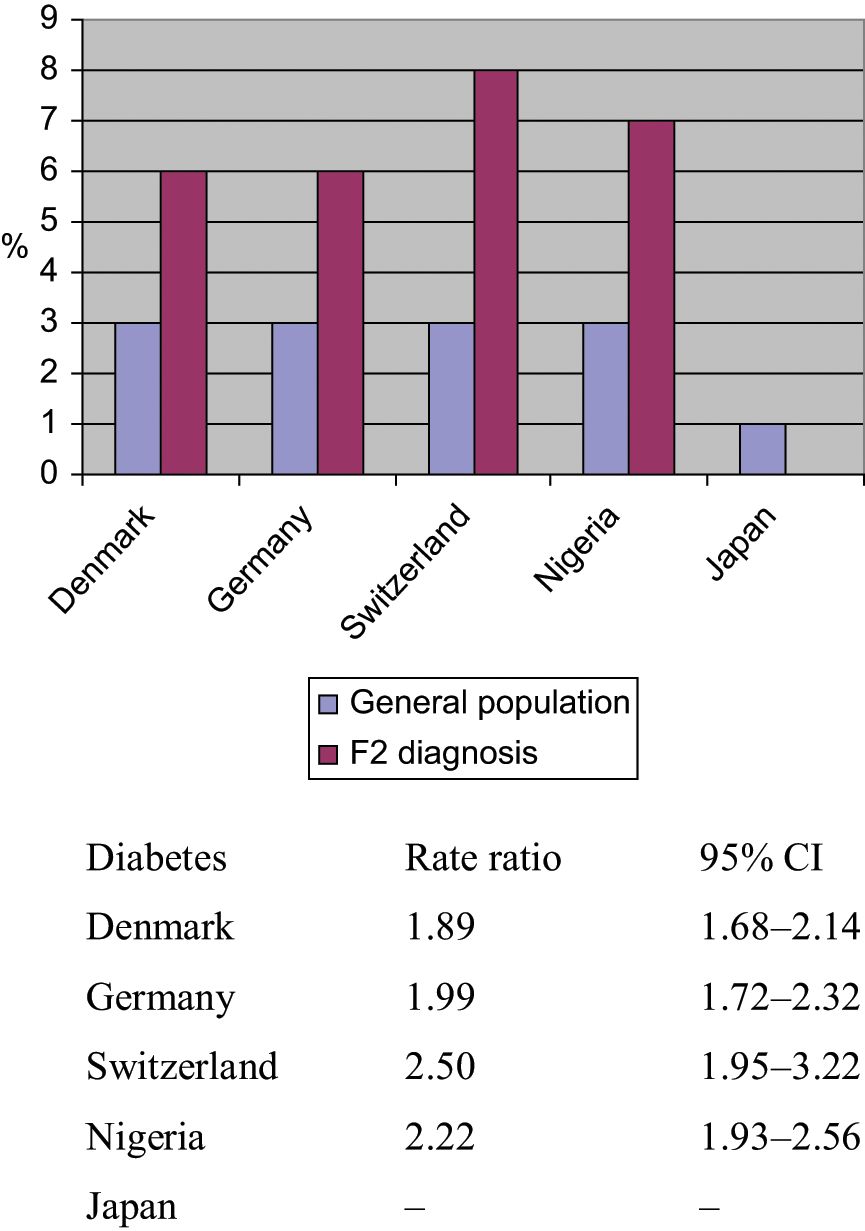
Standardized prevalence of diabetes in diagnostic group F2.
The prevalence of overweight in the five centres is shown in Figure 3. The rate ratios for the Danish and Nigerian centres are the highest and are lowest for Germany, Switzerland and Japan. No significant differences are shown. Nigerian data are for females only. Despite the standardized rate ratio, the risk for overweight is doubled in patients with an F2 diagnoses in Denmark and Germany, and is increased by approximately 65% in Nigeria; however, the rate ratio is within a narrow range (1.60–1.79) for all five countries. This indicates that overweight follows the general population, with an approximate increase of 60–80% compared with the national general population.
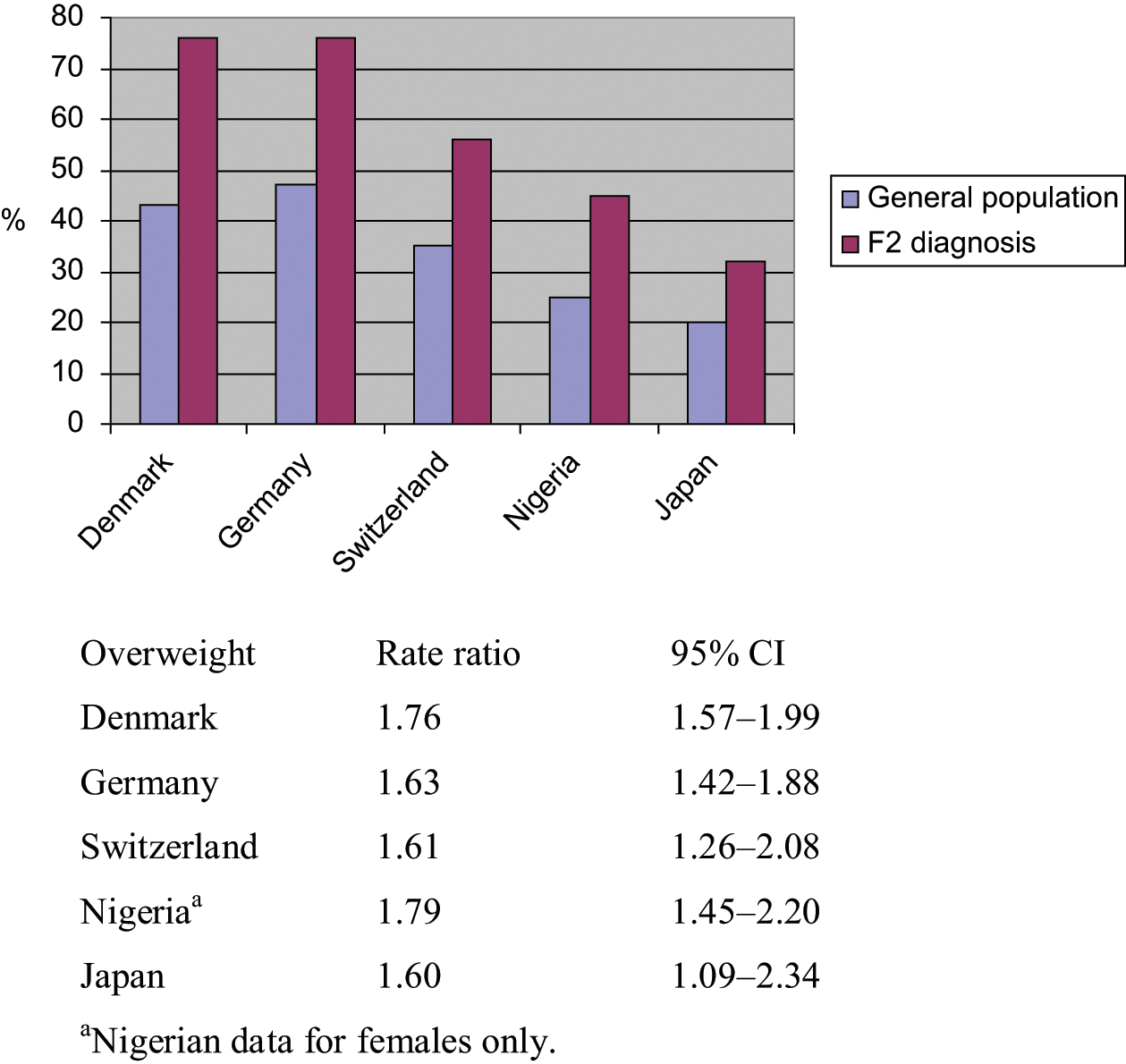
Standardized prevalence of overweight in diagnostic group F2.
Figure 4 shows the prevalence of CVD in the general population and among F3 probands. As with CVD in the F2 group, a severely increased occurrence of CVD in F3 patients is seen within the same range in all the countries. However, because of a low prevalence of CVD in the general Japanese population, the Japanese CVD rate ratio is significantly higher.
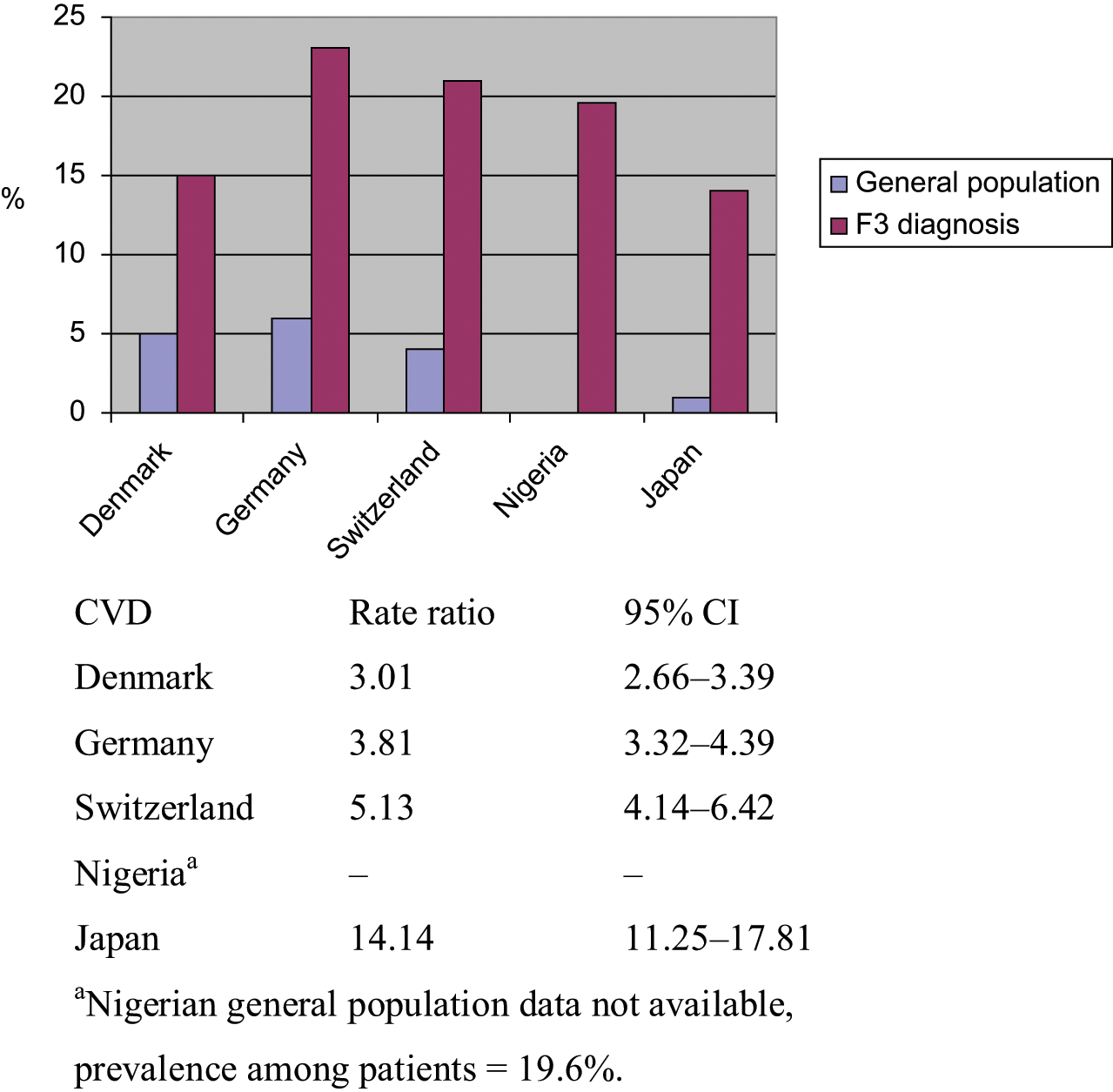
Standardized prevalence of CVD in diagnostic group F3.
Diabetes in the general population and in diagnostic group F3, where the rate ratio is lowest for Denmark and Japan (Denmark being significantly lower than Germany and Nigeria, and Japan being significantly lower than Germany and Nigeria), is shown in Figure 5.
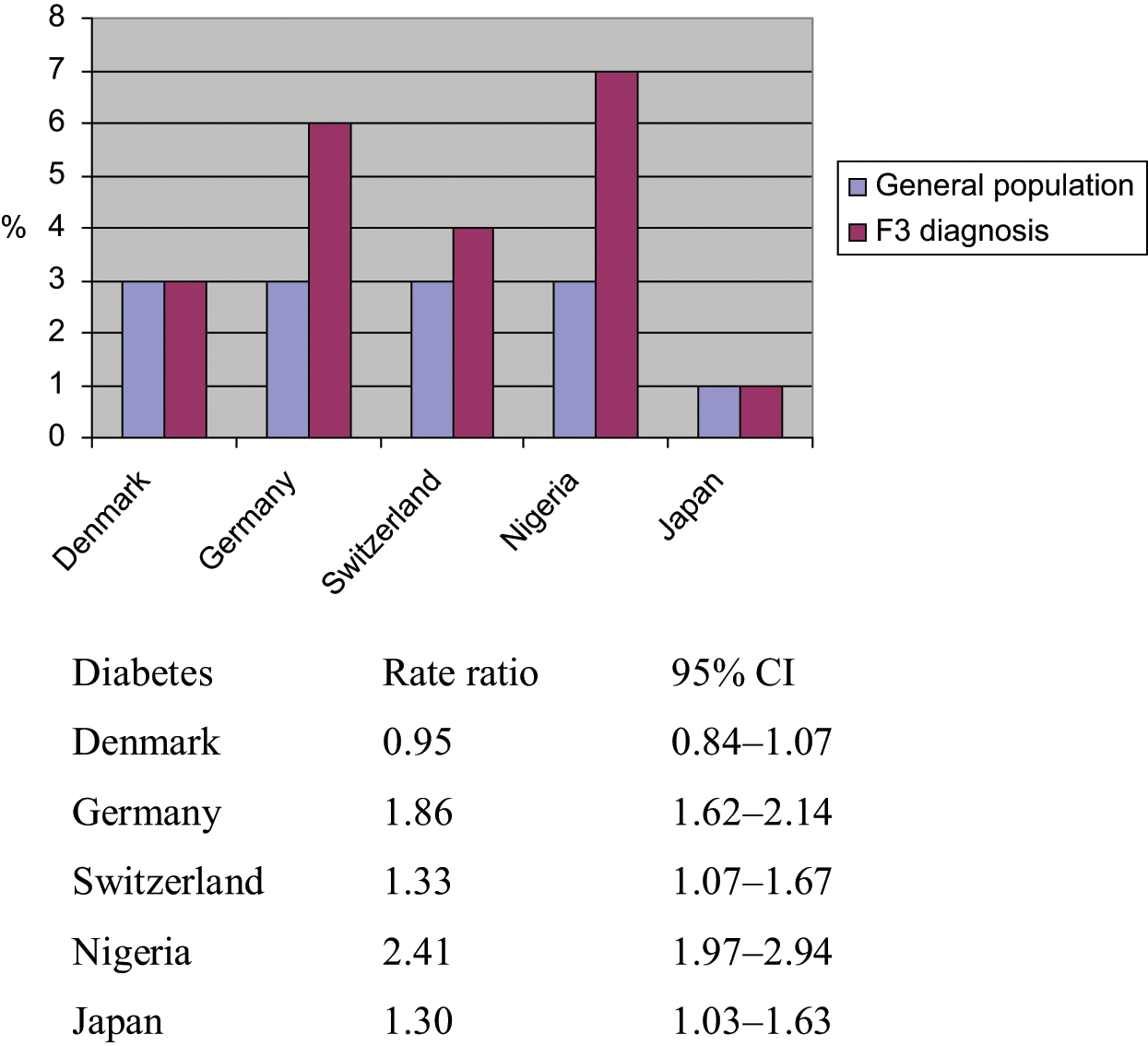
Standardized prevalence of diabetes in diagnostic group F3.
Overweight in the general population and diagnostic group F3 is presented in Figure 6. The lowest rate ratio is seen in the Swiss and the Japanese samples. The results for Japan, Switzerland and Denmark, which are within the same range, are significantly lower than for Germany.
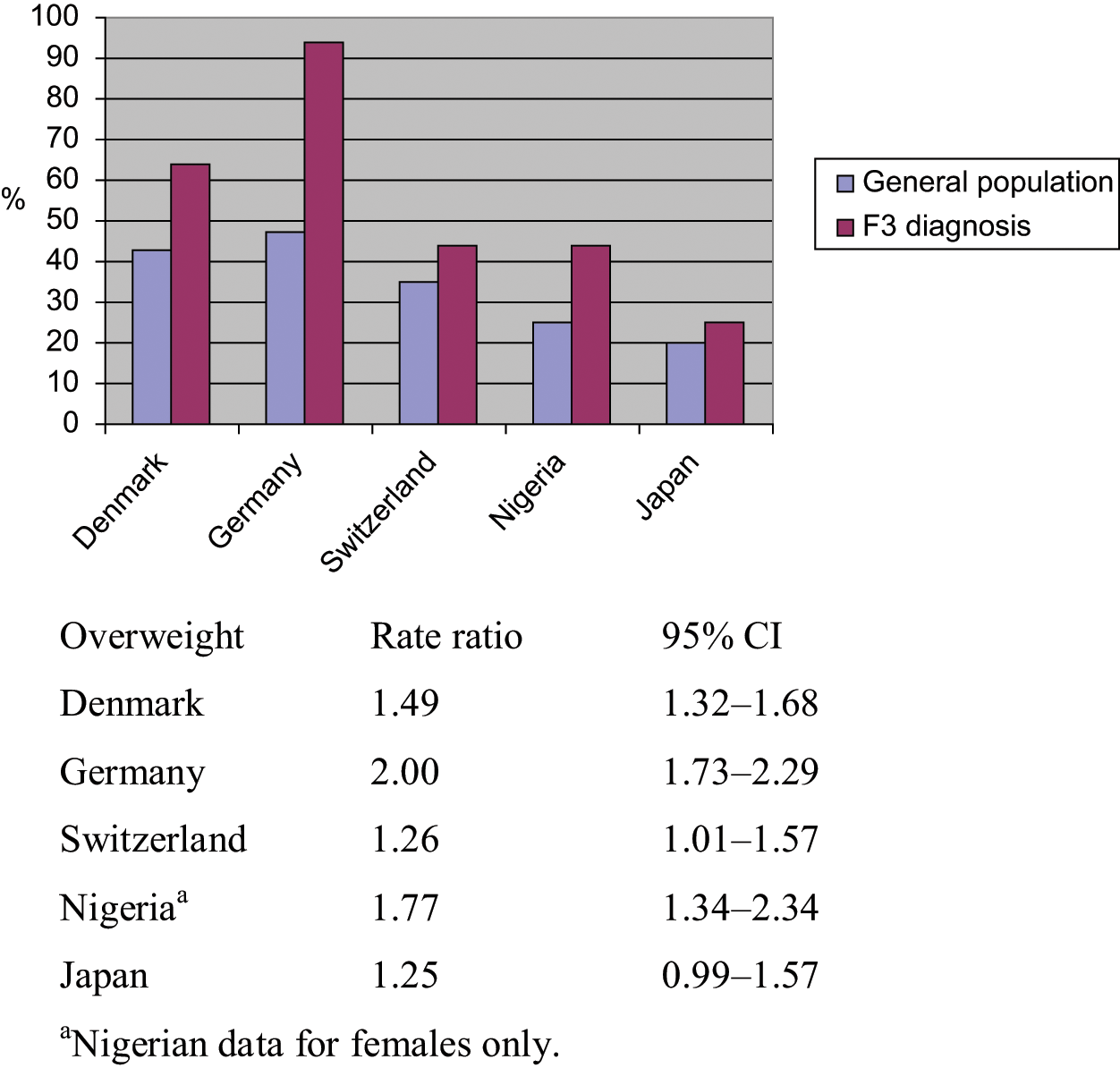
Standardized prevalence of overweight in diagnostic group F3.
Discussion
This study examined the prevalence of CVD, DM and overweight in the ICD-10 diagnostic groups F2 and F3 (WHO, 1992) in centres representing three different cultures – Western Europe, Africa and Japan – and compared prevalence to the background populations on a standardized basis. The main findings indicate a marked increase in the prevalence of CVD in all three cultures, and it was found among patients with affective disorders as well as among patients with schizophrenia spectrum disorders. Patients with schizophrenia spectrum disorders were markedly overweight compared with the background population. Finally, we found a marked excess of diabetes in the group of schizophrenia spectrum disorders. Overweight followed weight distribution in the background population. This parallelism is in accordance with the literature (Saito et al., 2000) however, we did not identify this phenomenon in CVD and diabetes, perhaps because of our rather limited samples. The causes for the excess of CVD, diabetes and overweight in the studied population are attributed, in particular, to lifestyle factors pronounced in mental disorders (Gillum 1996; Yano et al., 1978). Furthermore, possible general factors, such as genetic factors, behavioural mechanisms, dysregulation of the immune system and omega-3 fatty acid deficiency, explaining the high correlation between CVD and depression, have recently been reviewed by Stapelberg et al. (2011).
Lifestyle factors related to an increased prevalence of overweight, CVD and diabetes may be decreasing among higher-income groups in Western populations (Craig and Mindell, 2008), but not among low-income groups in which people with mental disorders are over-represented. The increased morbidity data shown in our study for Nigeria may indicate the presence of Western lifestyle diseases among Nigerian patients with mental disorders. Focus needs to be on the burden of somatic disease – particularly overweight in developing countries where income levels are not rising adequately; cultural habits and the transition to modern lifestyles, changing diets and patterns of transportation as urbanization is growing are also important factors. Cultural diversity and epidemiological transition are important factors in describing the problems mentioned above (Bhugra and Becker, 2005; Bhugra et al., 2011; Mirzaei et al., 2009). As overweight together with other lifestyle factors is an important risk factor in developing CVD among people with mental illness, as it is in the general population, it is to be foreseen that there will be a growing need for programmes focusing on those problems, especially in developing countries with limited access to medical care.
Some issues limit the conclusions that can be made from our study, in particular the lack of Nigerian background data on CVD. However, the Nigerian results on overweight and diabetes follow the same pattern as the Western centres. Furthermore, the limited size of the Japanese sample makes it difficult to draw conclusions from the Japanese results compared with Western Europe and Nigeria. Finally, the participating centres were not representative of their respective cultures.
Owing to the limited sample size, conclusions regarding Japan must be very conservative. Data on cultural backgrounds were only measured from the data obtained from the different centres located in the areas representing the cultures of Western Europe, Africa (Nigeria) and Japan, which also represent high- and low-income countries. The local samples of patients from a non-Western cultural background included in the Western Europe samples were too small to conclude on.
An analysis of obesity (BMI ≥ 30) was not performed because the sample was not of a size making it possible to gain sufficient power in the analysis, and, moreover, we would not have been able to include those patients who might have had a minor weight gain from, for example, antipsychotic treatment. Also, the non-availability of national data on the percentage of inhabitants with BMI ≥ 30 from all participating countries influenced the choice of dichotomizing point.
It should also be taken into consideration that we could not include data from non-participating patients as a result of ethical reasons; this may further add to the problems of interpreting the results from the small amount of Japanese data. However, none of the centres from the entire study reported serious concerns about the possible effect of patients who declined participation in the study.
In conclusion, we found an increased occurrence of CVD, diabetes and overweight in patients with affective disorders and schizophrenia spectrum disorders in centres representing Western Europe, Nigeria and Japan compared with background populations. Furthermore, the increased prevalence follows the population figure.
The prevalence of somatic illness in patients with a severe mental illness is seen to be parallel to the prevalence of somatic illness in the general population, reflecting cultural diversities.
Footnotes
Funding
Eli Lilly supported the planning meeting held in Aalborg, Denmark.
Declaration of interest
Povl Munk-Jørgensen received a non-conditioned educational grant form Eli Lilly (see above). Grants have been received previously from Wyeth, Lundbeck, Bristol-Myers Squibb, Janssen-Cilag, AstraZeneca and Servier, but are not connected to the present study. There is nothing to declare since October 2009.
Thomas Becker reports research funding (unrestricted research grants) to the Department of Psychiatry II, Ulm University for clinical trials and investigator-initiated trials from: Affectis Pharmaceuticals (D-Martinsried), AOK Bundesverband (D-Berlin), AstraZeneca (D-Wedel), DGPPN (Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde, D-Berlin), GlaxoSmithKline (D-Munich) and Robert-Bosch-Stiftung (D-Stuttgart).
The remaining authors have no interests to declare.