
Abstract
Objective:
To evaluate the suitability and acceptability of computerised cognitive behaviour therapy (CCBT).
Method:
Participants were patients who had been referred to a secondary care service in the usual manner, and then offered participation in a randomised controlled trial comparing the efficacy of CCBT with a control condition (waitlist) for patients with a current primary diagnosis of generalised anxiety disorder, panic disorder or social phobia. Data were collected regarding the recruitment and retention of patients, and patient ratings (anchored Likert scales) of treatment credibility, treatment satisfaction, treatment acceptability and telephone support.
Results:
A total of 1141 referrals were received by the secondary care service. Of the 1141, 748 (66%) were not suitable for the study, 178 (16%) declined to participate and 127 (11%) were not contactable. Therefore, of the 1141 patients referred to the secondary care service, only 88 patients (8%) were eligible and consenting for the study. The single most common reason for patients not being suitable for the study was that the referral was urgent. In a clinical setting where CCBT could be used alongside clinical management, many of these patients may have been suitable for CCBT. Of the patients randomised to treatment (n = 40), 65% completed treatment. Drop-out rates were not significantly different across diagnostic groups. The single most commonly cited reason for not completing treatment was ‘too busy’. Patient ratings of treatment were typically favourable (credibility, satisfaction, acceptability and telephone support).
Conclusions:
CCBT was typically rated favourably by patients referred to a secondary care service and randomised to treatment. However, only a small minority of patients was eligible and consenting for the trial. Therefore, while CCBT may be an acceptable treatment, its suitability for secondary care settings remains unclear.
Introduction
A growing body of literature supports the efficacy of computerised cognitive behaviour therapy (CCBT) (Andrews et al., 2010; Green and Iverson, 2009; Griffiths and Christensen, 2006; Kaltenthaler et al., 2006; Przeworski and Newman, 2006; Spek et al., 2007; Titov, 2007). Computerised cognitive behaviour therapy is cost effective and has the potential to make effective treatment available to more people (Cavanagh and Shapiro, 2004; Kaltenthaler et al., 2002; McCrone et al., 2004; Titov, 2007). Within the anxiety disorders field, CCBT has been included in the NICE clinical guidelines for the management of anxiety in adults in primary, secondary and community care (NICE, 2004).
However, concerns have been raised regarding barriers to the uptake of CCBT (Waller and Gilbody, 2009), and the need for studies evaluating the acceptability of computerised approaches within Australasian populations has also been previously noted (Titov, 2007). While a meta-analysis found that computer therapy for anxiety (and depressive) disorders was acceptable (Andrews et al., 2010), this analysis was published prior to recent studies involving participants in secondary care settings with anxiety disorders (Bell et al., 2012; Bergström et al., 2010; Hedman et al., 2011). ‘Secondary care’ here refers to treatment provided by a specialist service to which a patient has been referred by another health care provider, most commonly a primary care provider such as a general practitioner. By definition, patients accepted into a secondary care service are more severely unwell, impaired, complex and/or have treatment-resistant difficulties (Bell et al., 2012). Therefore, it is important that the suitability and acceptability of CCBT within secondary care settings is examined. Benefits were found for CCBT in a naturalistic, uncontrolled study of eight sessions of CCBT in a specialist CBT centre in the UK (Learmonth et al., 2008).
Two studies have recently evaluated CCBT for anxiety disorders (panic disorder and social anxiety) in secondary care settings (psychiatric care) and found positive benefits for CCBT (Bergström et al., 2010; Hedman et al., 2011). However, these studies have included a substantial proportion of participants who were self-referred, in addition to participants who were referred by their physician. In the study by Bergström and colleagues, approximately one-third of participants were self-referred, and in the study by Hedman and colleagues approximately three-quarters were self-referred.
In a previous paper (Bell et al., 2012), we report the results of a randomised controlled trial comparing the effectiveness of CCBT versus a control condition (waiting list) for patients with a current primary anxiety disorder (generalised anxiety disorder (GAD), panic disorder or social phobia) who were referred to a secondary care setting (specialist anxiety service) in the usual manner by either general practitioners or mental health clinicians. No participants were self-referred.
We found that patients randomised to CCBT reported significantly less symptomatology than patients randomised to the control condition on approximately half of the self-report primary measures (the Work and Social Adjustment Scale; Mundt et al., 2002) and approximately half of the secondary measures at both 12 and 24 weeks: the Liebowitz Social Anxiety Scale (Safren et al., 1999), the Penn State Worry Questionnaire (Meyer et al., 1990), the Generalized Anxiety Disorder Inventory (Argyropoulos et al., 2007) and the Fear Questionnaire (Marks and Mathews, 1979). Effect sizes were moderate. The reader is referred to the original outcome paper for more details (see Bell et al., 2012).
In the present paper, we evaluate the suitability and acceptability of CCBT amongst these patients. Specifically, we examine the recruitment and retention of patients, and patient ratings of treatment credibility, treatment satisfaction, treatment acceptability and telephone support.
Method
Overview
This randomised clinical trial was conducted in collaboration with The Anxiety Disorders Unit, a publicly funded, specialist, outpatient anxiety service in Christchurch, New Zealand. Patients were referred to The Anxiety Disorders Unit in the usual manner. Patients who had a current, primary diagnosis of GAD, panic disorder or social phobia were potentially eligible to participate in the trial. Following screening and clinical assessment, suitable patients were offered participation in the trial while waiting to be assessed by The Anxiety Disorders Unit (usual wait-time approximately 9 months for non-urgent referrals). Eligible and consenting trial participants were randomised to either CCBT (Andrews, 2005) or waitlist. The latter involved remaining on the waiting list to be seen by The Anxiety Disorders Unit, as would normally have occurred. An end assessment (12 weeks) and a follow-up assessment (24 weeks) were conducted for all participants in the clinical trial.
Recruitment
Participants were consecutive patients who had been referred in writing to The Anxiety Disorders Unit by general practitioners and mental health clinicians between June 2006 and November 2008. At the time of referral, referrers were not aware that suitable patients would be offered participation in the present study, in addition to care from The Anxiety Disorders Unit. Therefore, participants were not pre-selected for suitability for the trial by the referrer.
Eligibility criteria
Participants were required to be aged between 18 and 65 years of age, to have access to a computer and the internet, be sufficiently competent with the English language and reading to be able to manage the requirements of the programme, and to have a current DSM-IV primary diagnosis (American Psychiatric Association, 1994) of GAD, panic disorder with or without agoraphobia or social phobia. Patients were not eligible for the trial if the referral was urgent or if their current primary diagnosis (DSM-IV) (American Psychiatric Association, 1994) was obsessive compulsive disorder (OCD), specific phobia or post- traumatic stress disorder (PTSD), as the computerised treatment programme (Andrews, 2005) did not provide programmes for these disorders. Patients were also not eligible for the trial if they had a current diagnosis of psychotic illness, bipolar I disorder, or alcohol/drug dependence, if they had active suicidal ideation, if they were currently receiving cognitive behaviour therapy (CBT), if they had commenced or changed dose of psychotropic medication in the last 6 weeks, or if they had a medical disorder that made participation in the trial unwise, such as disabling cardiac or respiratory disorders or serious neurological disorders.
Procedure
Referral and initial screening process
All referrals to The Anxiety Disorders Unit were reviewed by clinicians (CB, HC) at a standard clinical triage meeting. Patients were excluded if the referral letter indicated that the patient met one or more of the exclusion criteria. Following these exclusions, potentially suitable participants were sent a letter providing them with information about the trial, and asking them to contact the study coordinator if they wished to have no further contact regarding the study. Patients who had not opted out of the study were then telephoned by the research coordinator and invited to participate in a screening interview. The purpose of this interview was to identify the presence of any exclusion criteria, and to establish that it was likely that inclusion criteria would be met. Patients who appeared to be suitable for the study were then offered an assessment with a clinician (FC, CB, HC), either in the participant’s home or at our research offices, depending on participant preference.
Structured clinical assessment and consent
A structured clinical assessment was conducted with agreeable participants to determine eligibility for the study, and to ascertain which anxiety disorder was the current, primary problem (GAD, social phobia or panic disorder). Participants who met inclusion and exclusion criteria provided written informed consent.
Randomisation
Eligible and consenting participants were randomised to either CCBT or waiting list. Randomisation was done using a stratified block design for the primary diagnosis (GAD, social phobia or panic disorder). The stratified randomisation list was generated by a statistician, not involved in implementation of the study. For social phobia the allocation was in permuted blocks. The allocation list and envelopes containing the allocations were held by the clinical research unit coordinator, who was not involved directly in implementation of the study. This ensured that the clinicians and the study coordinator, who were involved in assessment and enrolment, were not biased in the enrolment process. Subjects were randomised in a 1:1 ratio to the computerised programme and waitlist.
Baseline neuropsychological and self-report questionnaires
Following randomisation, all participants in the trial were given a battery of self-report questionnaires to complete over the next week, and an appointment was made for baseline neuropsychological testing to be conducted (details will be published elsewhere). Neuropsychological testing was conducted (half-day duration) and the self-report questionnaires were collected.
Treatment
Participants who had been randomised to CCBT were given their individualised computer code to enable them to access CCBT at the completion of their neuropsychological treatment. The research coordinator spent time with patients to ensure that they understood how to access the treatment programme, and answered any questions that patients had about practical aspects of using the programme.
Patients randomised to CCBT were provided with treatment via the CLIMATE programme (Andrews, 2005). This treatment programme was developed specifically for an Australasian population and utilises cognitive behavioural principles that have been shown to be effective in the treatment of anxiety disorders. This structured, interactive programme provides four to six CBT sessions (GAD = four; panic = six; social phobia = six). Homework is an integral feature of the programme for all disorders. Patients were instructed to complete the programme within 12 weeks. The programme requires a reading age of 11 years and no prior computer experience. ‘Treatment completion’ was defined as having completed three of the four treatment sessions for the GAD group, and four of the six treatment sessions for the panic and social phobia groups.
Telephone support
Participants who had been randomised to CCBT were phoned briefly every 2 weeks while they were receiving treatment. The primary purpose of this contact was to ensure that they were not having difficulties accessing CCBT, and to encourage on-going participation. Participants who had been randomised to waitlist were also briefly contacted every 2 weeks over this period of time, to control for contact.
All calls to participants followed a pre-determined written structure. This included establishing rapport, asking them how they were, identifying any problems they were having participating in the trial, and encouraging on-going participation in the trial. The structure and content of these calls was the same for both the treatment and the control groups, except that questions about the treatment programme were omitted for the control group. Despite this, the duration of the calls was roughly similar (approximately 5 minutes). All participants were contacted briefly every 2 weeks over the 12-week initial phase, regardless of whether they were in the treatment group or the control group (i.e. a total of six times).
End and follow-up assessments
An end assessment (12 weeks) and a follow-up assessment (24 weeks) were conducted for all participants in the clinical trial. Following receipt of the final self-report questionnaires at follow-up assessment, all patients were given $150 in recognition of the time spent participating in the study.
Measures
Clinical assessment
At baseline, all patients participated in a structured clinical interview assessing the presence of DSM-IV Axis I disorders (American Psychiatric Association, 1994).
Treatment credibility at baseline (1–7)
At baseline, patients randomised to CCBT completed anchored Likert scales (1–7) asking the following: How logical does treatment seem to you? How useful does treatment seem to you? How confident are you that this treatment will be successful? How confident would you be in recommending this treatment to a friend with similar difficulties? How likely do you think you are to complete the computer sessions and homework? These Likert scales were chosen because we wanted to assess how credible CCBT was in our local context, and these Likert scales have been used in a range of treatment trials conducted at the Clinical Research Unit.
Treatment ratings at end assessment (0–8)
At the end assessment, patients randomised to CCBT completed anchored Likert scales (0–8) assessing the following areas. These Likert scales had either been used in other treatment trials in the Clinical Research Unit (overall treatment satisfaction ratings), or were developed to assess aspects of treatment specific to CCBT (the acceptability of this approach, the usefulness and role of telephone support, and reasons for not completing treatment). Specific items were developed following examination of the literature, informal feedback from patients and discussion amongst the investigators.
Overall treatment satisfaction (0–8)
How satisfied were you with this treatment? How effective do you think this treatment was? Would you recommend this treatment to somebody else?
Acceptability of computerised treatment approach (0–8)
How acceptable did you find it to receive treatment via a computer? How much of this treatment did you complete? How enjoyable did you find this program? How applicable was this program to your particular anxiety disorder?
Telephone support (0–8)
How useful did you find the telephone support? How much of the program would you have completed without telephone support?
Reasons for not completing the treatment package (0–8)
The following possible reasons for finding it difficult to complete the treatment programme were rated: too busy, problems with computer accessibility, limited computer skill, lacking motivation, the thought of it made me too anxious, I was getting better without the programme, it was all too much, the homework was too difficult, and it didn’t seem relevant to my particular problem. All patients randomised to treatment were asked to complete this scale, even if they had been identified as having ‘completed’ treatment, as patients did not need to complete 100% of sessions to be classified as having completed treatment (see below).
Data analysis
This study primarily utilizes descriptive statistics. Where differences between the diagnostic groups were evaluated, chi square was used for dichotomous measures and one-way analysis of variance was used for continuous measures. Significance was determined using p < 0.05.
Trial registration
The trial was registered with the Australasian Clinical Trials Registry (ACTRN012606000349549), and was approved by the Upper South B Regional Ethics Committee, Christchurch, New Zealand (URB/06/05/039).
Results
Patient flow
Figure 1 shows the flow of patients through the study. A total of 1141 referrals were received by The Anxiety Disorders Unit. In total, 748 (66%) were not suitable for the study, 178 (16%) declined to participate and 127 (11%) were not contactable. Therefore, of the 1141 patients referred to The Anxiety Disorders Unit, only 88 patients (8%) were eligible and consenting for the study. Unfortunately, a changeover with the computer software caused major disruption for five patients, resulting in them needing to be withdrawn from the study. Therefore, 83 eligible and consenting patients entered the study.
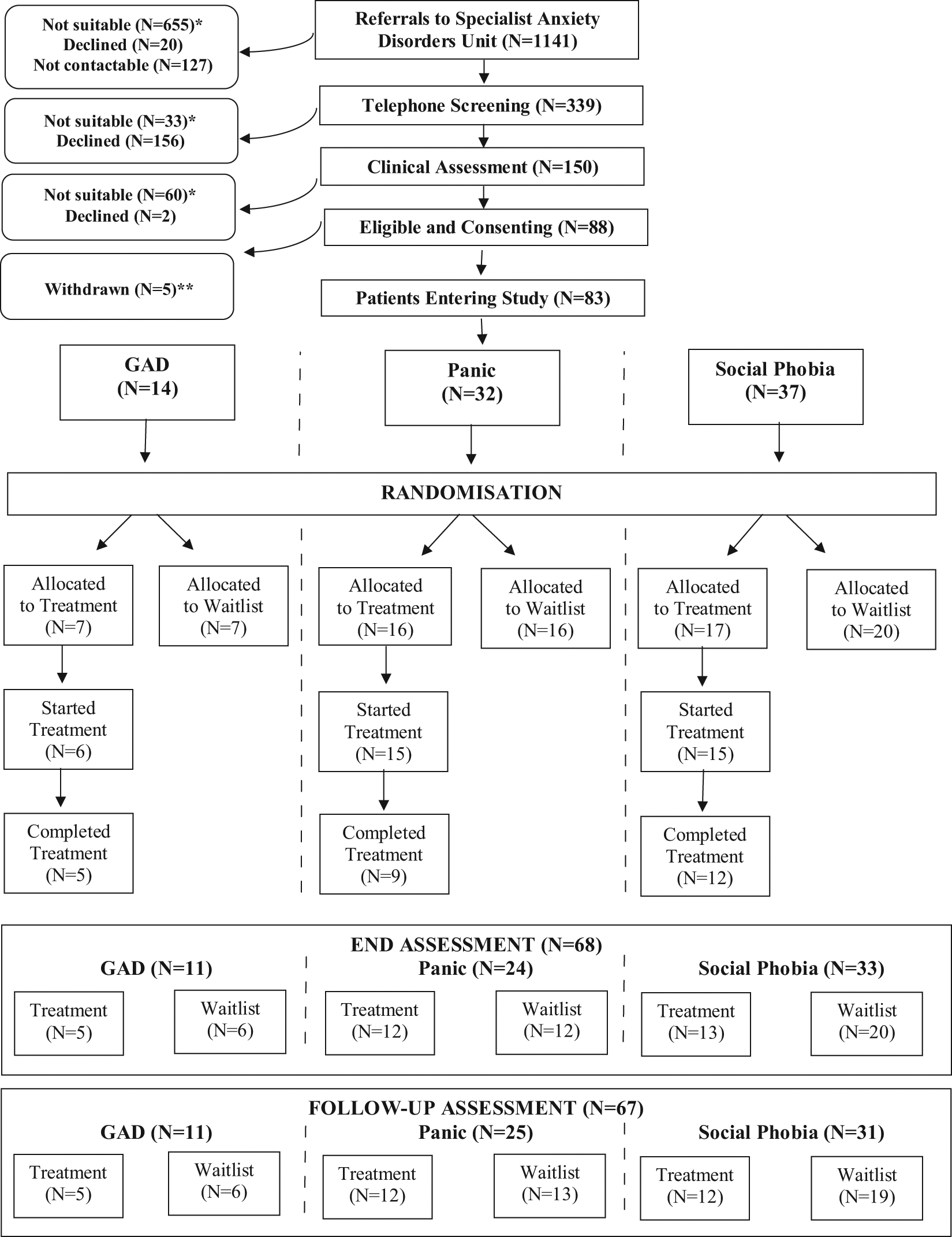
Schematic showing patient flow through the study.
The 83 patients who entered the study had a current primary diagnosis of either GAD (n = 14), panic disorder (n = 32) or social phobia (n = 37). Patients were then randomised to either CCBT or waitlist, within their diagnostic blocks (GAD: treatment = seven, waitlist = seven; panic: treatment = 16, waitlist = 16; social phobia: treatment = 17, waitlist = 20). Therefore, in total, 40 patients were randomised to treatment and 43 were randomised to waitlist. Of the 40 patients randomised to treatment, 26 (65%) completed treatment (GAD = 5/7; panic = 9/16; social phobia = 12/17).
At the end assessment, 68 (82%) of the original sample of 83 patients who entered the study participated in assessment (GAD = 11; panic = 24; social phobia = 33). Patients who did not attend the end assessment were approximately evenly divided between those who had been randomised to treatment and those who had been randomised to waitlist. Four patients who did not complete treatment participated in the end assessment.
At the follow-up assessment, 67 (81%) of the original sample of 83 eligible and consenting patients participated in assessment (GAD = 11; panic = 25; social phobia = 31). Patients who did not attend the follow-up assessment were approximately evenly divided between those who had been randomised to treatment and those who had been randomised to waitlist. Three patients who did not complete treatment participated in follow-up assessment.
Patient suitability
As stated previously, 748 of the original 1141 (66%) patients referred were not suitable for the study. Table 1 shows when patients were identified as not being suitable for the study, and provides a breakdown of the reasons why patients were not suitable. Table 1 also combines and summarizes data from when the referral was received, from telephone screening and from the clinical assessment, to show how commonly patients were excluded for various reasons. Most patients who were unsuitable for the study were identified at the outset, when their referral was initially received by The Anxiety Disorders Unit, most commonly because the referral was urgent (n = 219). These patients were judged by The Anxiety Disorders Unit to need face-to-face treatment sooner than the research protocol allowed. The service did not feel that it would be ethical to delay these patients’ face-to-face treatment from the service while they completed the research protocol.
Breakdown of reasons why patients were not suitable for the study and when these factors were identified.
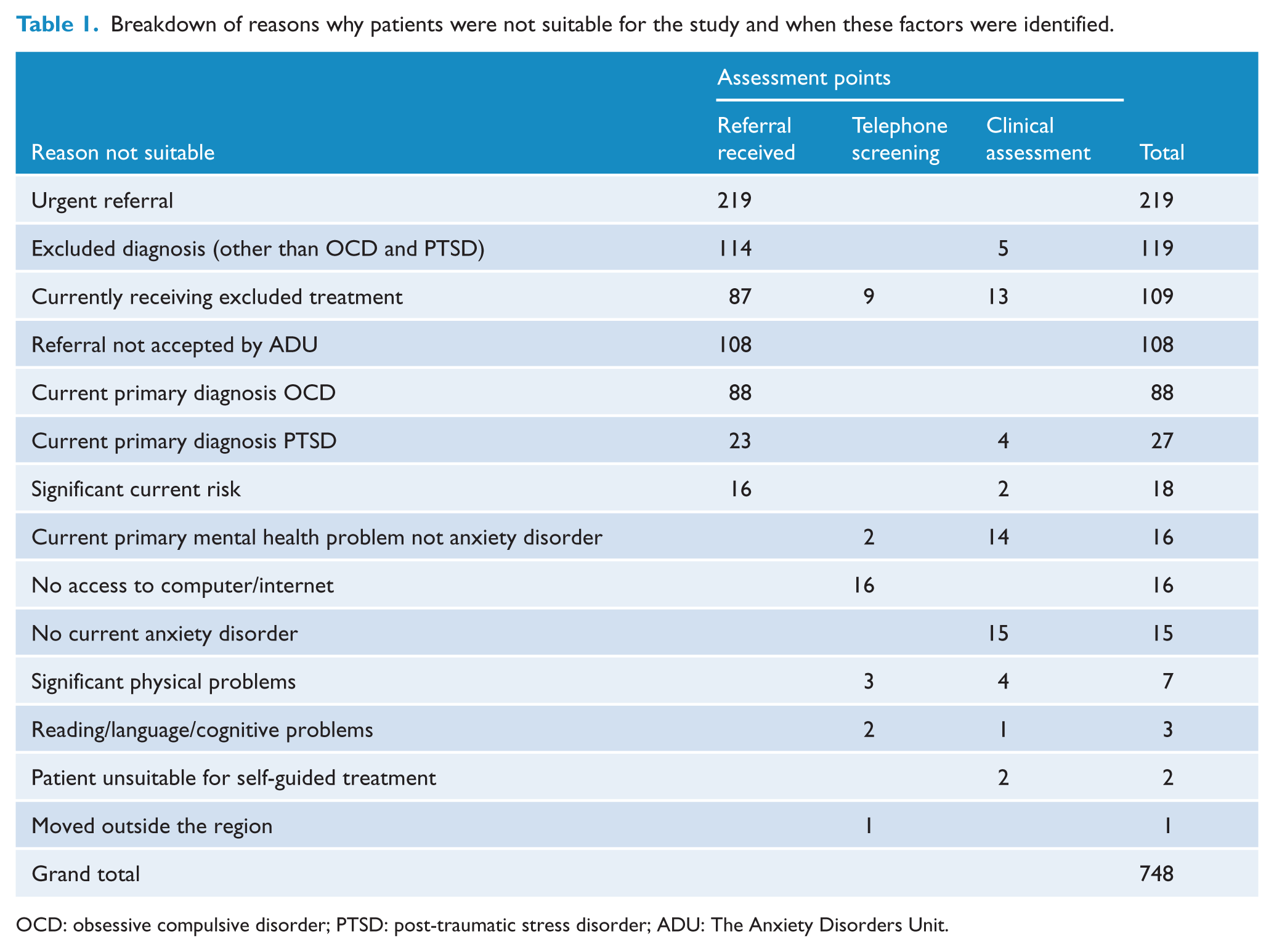
OCD: obsessive compulsive disorder; PTSD: post-traumatic stress disorder; ADU: The Anxiety Disorders Unit.
To aid interpretation of the results, the reasons for patients being identified as unsuitable for the study at referral, telephone screening and clinical assessment (see Table 1) were grouped into the clusters below.
CCBT unsuitable, unavailable, or unwise (n = 380/748)
Reasons included in this cluster: urgent referral (n = 219), current primary diagnosis of OCD or PTSD (n = 115), significant current risk (n = 18), no computer/internet access (n = 16), physical health problems contraindicating CCBT (n = 7), reading/language/cognitive difficulties (n = 3), patient unsuitable for self-treatment (n = 2).
Significant other (non-anxiety) mental health problems (n = 135/748)
Reasons included in this cluster: presence of excluded diagnoses (current bipolar 1 disorder, psychotic illness or alcohol/drug dependence; n = 119), or primary mental health problem not anxiety disorder (n = 16).
Inappropriate referral to service (n = 123/748)
Reasons included in this cluster: referral not accepted by service (n = 108), no current anxiety disorder (n = 15).
Currently receiving excluded treatment (n = 109/748)
Reasons included in this cluster: receiving CBT or recently started on psychotropic medication (n = 109).
Miscellaneous (n = 2/748)
Reason included in this cluster: moved from the region (n = 1).
Declined to participate
As stated previously, 178 of the original 1141 (16%) patients declined to participate in the study. Consistent with our ethical agreement, patients’ right to decline to participate in the study without needing to give an explanation was respected. A minority of patients (n = 55) volunteered the following reasons for declining to participate: too busy (n = 26), no computer/internet access (n = 7), don’t want/need treatment now (n = 5), already in treatment/counselling (n = 3), can’t get time off work (n = 2), want to wait for assessment at The Anxiety Disorders Unit (n = 2), pregnant (n = 2), moving out of Christchurch soon (n = 2), too physically sick/facing major surgery (n = 2), participation in study too threatening (n = 1), no anxiety disorder (n = 1), too anxious (n = 1) and ‘I don’t do studies’ (n = 1).
Treatment ratings
Table 2 shows mean (SD, range) ratings of treatment credibility, treatment satisfaction, treatment acceptability and telephone support made across the three diagnostic groups for patients randomised to treatment (1–7 treatment credibility; 0–8 all other scales). Ratings for treatment credibility were made prior to receiving treatment, whereas all other treatment ratings were made at the end assessment. Overall, the mean treatment ratings were favourable on all of the treatment scales. No significant differences were found between the diagnostic groups on ratings of treatment credibility, treatment satisfaction, treatment acceptability or telephone support (p > 0.05, using one-way analysis of variance).
Ratings (mean, SD, range) of treatment credibility, treatment satisfaction, treatment acceptability and telephone support for patients randomised to treatment across diagnostic groups.
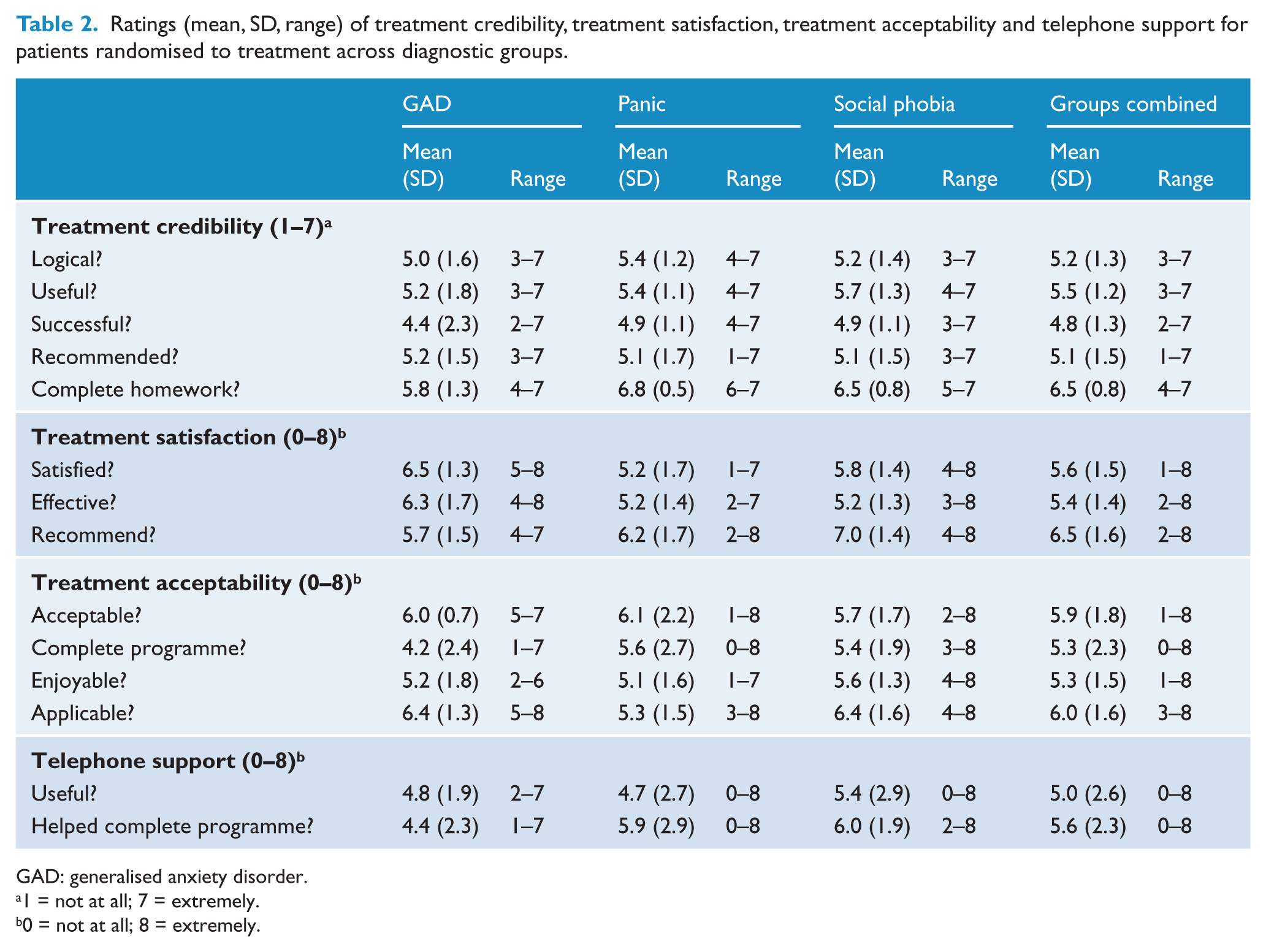
GAD: generalised anxiety disorder.
1 = not at all; 7 = extremely.
0 = not at all; 8 = extremely.
Treatment completion
Treatment completion across diagnostic groups
As stated previously, 14 of the 40 (35%) patients randomised to treatment did not complete treatment (GAD = 2/7, 29%; panic disorder = 7/16, 44%; social phobia = 5/17, 29%). Table 3 shows the number of treatment sessions completed by patients across the different diagnostic groups. Differences in dropout rates across the three diagnostic groups were not statistically significant (p = 0.64 using chi square). Figure 2 shows the percentage of patients who attended treatment sessions (categorized according to sessions attended) for patients randomised to treatment across the diagnostic groups. Examination of this figure shows a similar pattern across the diagnostic groups. Patients most commonly participated in ‘most’ or ‘all’ sessions, but approximately 10% of patients did not participate in any treatment sessions.
The number of treatment sessions completed by patients with GAD, panic disorder and social phobia.
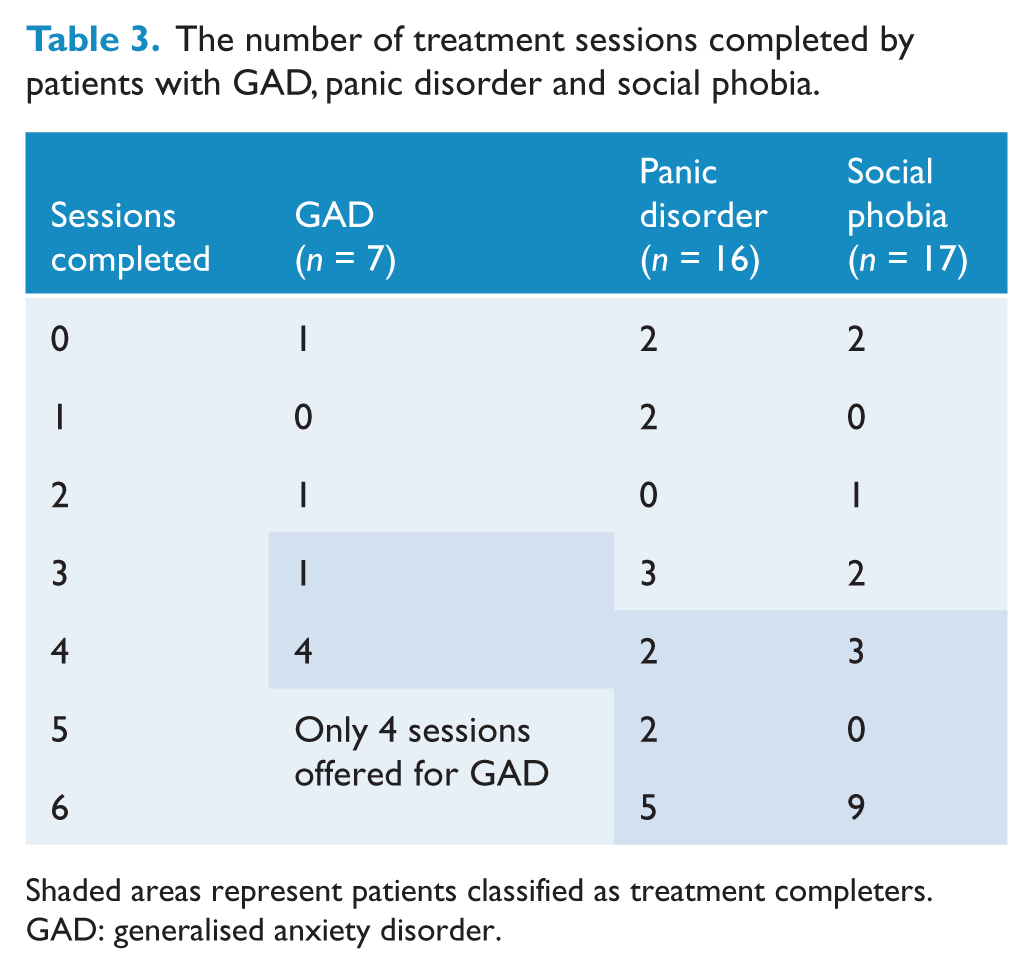
Shaded areas represent patients classified as treatment completers.
GAD: generalised anxiety disorder.
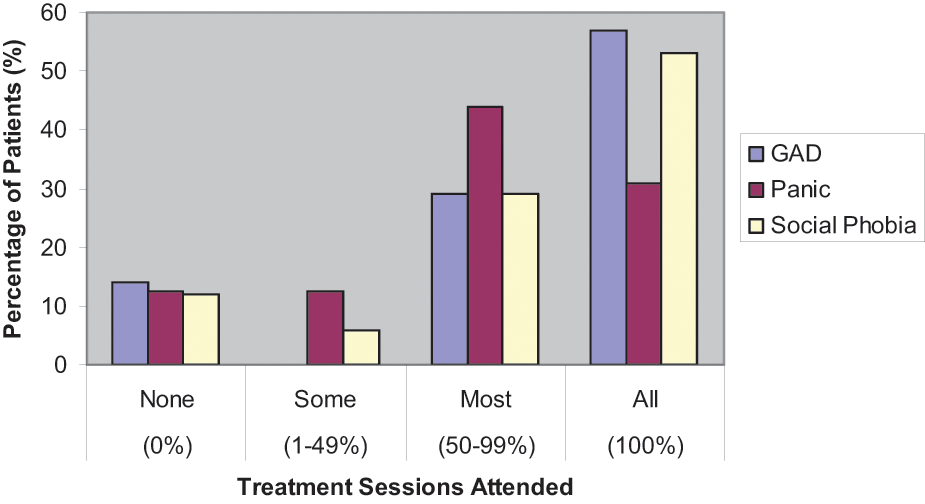
The percentage of patients who attended treatment sessions (categorized according to how many sessions were attended) for patients randomized to treatment across the diagnostic groups*
Treatment completers versus non-completers at baseline
Patients who completed treatment were compared with those who did not complete treatment on a range of demographic and baseline symptom severity ratings using independent samples t-tests and chi square. No significant differences were found in these tests. The exception was for the Beck Depression Inventory (Beck et al., 1996), where those who went on to complete treatment had significantly higher depression scores at baseline (t = 2.3, p = 0.03). Completers and non-completers were also compared on ratings of treatment credibility (made prior to treatment), and treatment satisfaction, treatment credibility, acceptability and telephone support made following treatment on independent samples t-tests. As expected, patients who completed treatment had significantly higher rates of self-reported treatment completion (‘Complete programme?’ Likert scale question on the Acceptability scale; t = 2.4, p = 0.03). Patients who completed treatment also had significantly higher ratings on the ‘Applicable?’ Likert scale question (Acceptability scale; t = 2.9, p = 0.02). No other significant differences were found between completers and non-completers.
Treatment completion and treatment outcome
Patients who completed treatment were compared with those who did not complete treatment on symptom severity ratings at 12 weeks and 24 weeks. No significant differences were found using independent samples t-tests and chi square.
Reasons for not completing treatment
Table 4 shows ratings (mean, SD, range) of reasons for not completing treatment made at the end of treatment by patients who had been randomised to treatment (0–8 scale). For all three diagnostic groups, the highest rated reason for not completing treatment was ‘too busy’. ‘Poor motivation’ was also rated highly. In the panic and social phobia groups, ‘difficulties with access to computer’ were rated highly, whereas the GAD group rated ‘too anxious’ and ‘all too much’ highly.
Ratings (mean, SD, range) for reasons for not completing treatment made by patients randomised to treatment across the diagnostic groups.
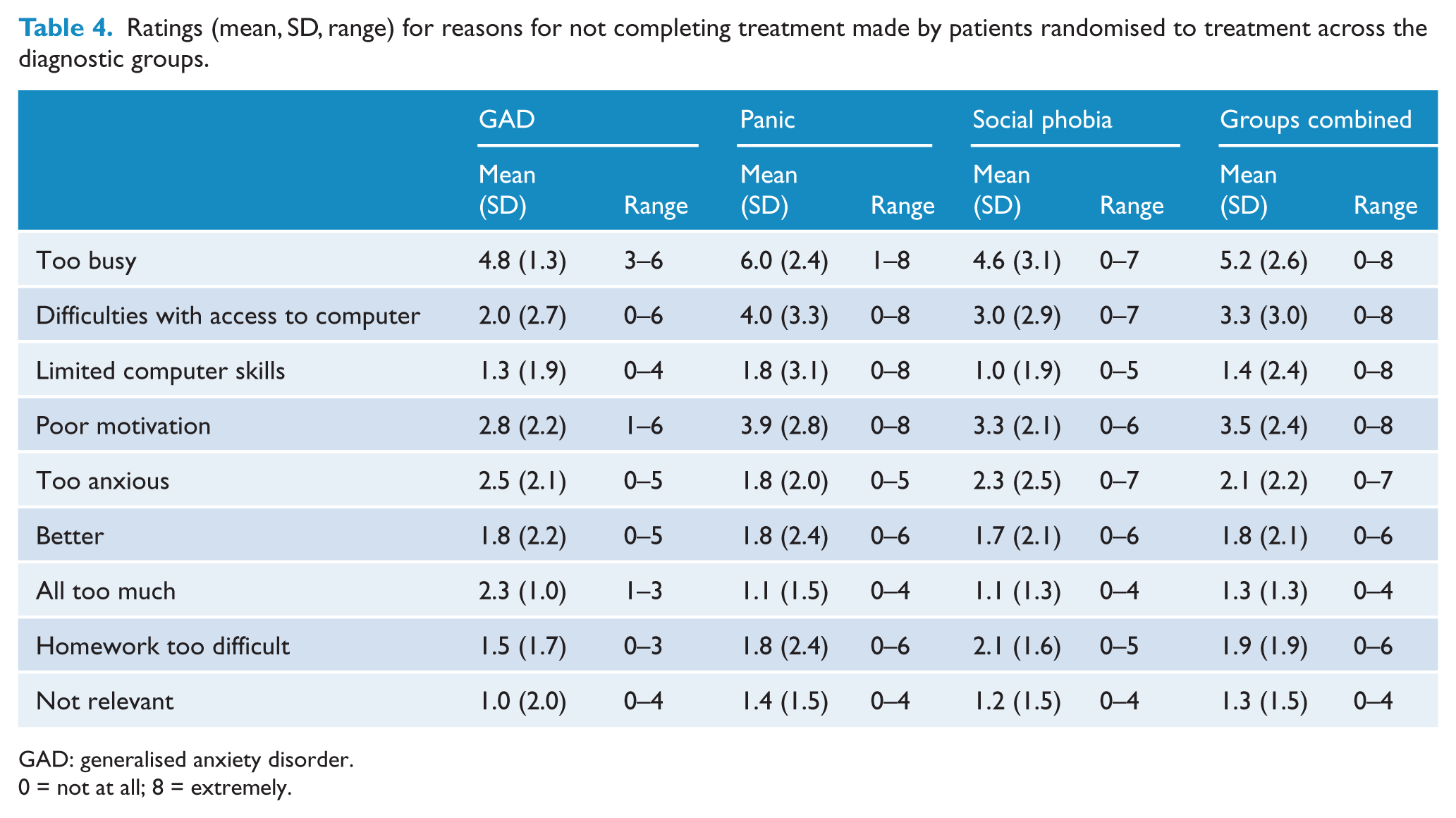
GAD: generalised anxiety disorder.
0 = not at all; 8 = extremely.
Discussion
The present study sought to evaluate the suitability and acceptability of CCBT for patients referred to a secondary care service in the usual manner. Two other studies (Bergström et al., 2010; Hedman et al., 2011) have previously evaluated CCBT for anxiety disorders in a secondary care setting. However, these studies also included a substantial proportion of participants (one-third to three-quarters) who had self-referred for treatment rather than being referred by their physician. The present study is the only known study where all the participants were referred to a secondary care service (by either a general practitioner or mental health clinician), and none were self-referred. We report the effectiveness of CCBT in detail elsewhere (Bell et al., 2012).
Following referral, potentially suitable patients were assessed and eligible and consenting patients participated in a randomised controlled trial comparing the efficacy of CCBT with a control condition (waitlist) for patients with a current primary anxiety disorder (GAD, panic disorder or social phobia). Specifically, we examined the recruitment and retention of patients, and patient ratings of treatment credibility, treatment satisfaction, treatment acceptability and telephone support.
Of the 1141 patients referred to a specialist outpatient anxiety service, only a small minority of patients (8%) was eligible and consenting for the study. Of those referred to the service, 66% were not suitable for the study, 16% declined to participate, and 11% were not contactable. Of the patients randomised to treatment (n = 40), 65% completed treatment. Drop-out rates were not significantly different across diagnostic groups. At the end assessment and follow-up assessment, 82% and 81% of eligible and consenting patients, respectively, participated in assessment. Mean treatment credibility, treatment satisfaction, treatment acceptability and telephone support ratings were favourable and no significant differences were found across diagnostic groups. The most commonly cited reason for not completing treatment was ‘too busy’.
The most striking finding from the present study was the high rate of patients who were unsuitable for the study (66%). This figure reflects the stringent research criteria that were applied, and does not necessarily generalise to the use of CCBT in a clinical setting. The most common single reason for patients not being suitable was that the referral was urgent. In the present study, patients who had been urgently referred were not eligible in part because there was insufficient time for them to complete the programme before being assessed at The Anxiety Disorders Unit. Therefore, in a clinical setting where CCBT could be used alongside clinical management, these patients may not have needed to be excluded.
When reasons were grouped to form clusters, the following factors were identified for patients being unsuitable (listed from most common to least common): (a) CCBT unsuitable, unavailable or unwise; (b) presence of other (non-anxiety) mental health problems; (c) inappropriate referral to the service; (d) patient participating in excluded treatment (CBT or recently commenced psychotropic medication); and (e) miscellaneous.
Within the ‘CCBT unsuitable, unavailable or unwise’ category, the most common reasons for patients being unsuitable were being an urgent referral or having a primary anxiety diagnosis for which a treatment package was not available (OCD or PTSD). This reflects the design of the study (CCBT could not be undertaken simultaneously with other effective treatment), and the investigators’ choice of computer package (no treatment for OCD or PTSD offered by CLIMATE at the time), rather than anything intrinsic about CCBT. It was much less common for patients to be unsuitable for the study because they had significant current risk, no computer access, physical problems that contraindicated participation or had reading/language difficulties.
It is important to view the present results within the context in which the study was conducted. The acceptability of CCBT was evaluated within the context of a randomised controlled trial primarily designed to compare the effectiveness of CCBT with a waitlist control group for a current primary anxiety disorder (Bell et al., 2012). As a consequence, many patients were deemed to be unsuitable for the study that may have been suitable in many clinical settings. Outside of a randomised controlled trial, patients who had been referred urgently, were receiving CBT, or had recently commenced psychotropic medication would also potentially have been suitable for CCBT. Because the study evaluated the impact of treatment on a current primary anxiety disorder, patients whose anxiety difficulties did not meet criteria for a DSM-IV disorder, or whose current primary diagnosis was, for example, major depression (with a co-morbid anxiety disorder), were unsuitable for the study even though they may well have benefited from CCBT for anxiety. Some patients were unsuitable for the study owing to safety concerns or because they had an excluded diagnosis (e.g. bipolar 1 disorder). However, in a clinical setting where CCBT was an adjunct to treatment and/or monitoring by a clinician, many of these patients may have been able to be offered CCBT for anxiety. Therefore, while the present results are sobering, caution needs to be exercised in extrapolating these results to clinical settings outside of a randomised controlled trial. For example, Gega and colleagues evaluated CCBT for anxiety and depression in a study that did not involve randomisation, and reported rates of less than half those found in the present study for patients being unsuitable (e.g. Gega et al., 2004).
Although it was less common for patients to reject the study than for patients to be unsuitable for the study, a substantial minority (16%) of patients declined to participate. It is possible that the demands of the assessment protocol were a factor in discouraging potential participants. However, we are not in a position to comment on the extent to which this may have occurred. Only a minority of participants volunteered that being ‘too busy’ was a factor in declining participation. Other studies that have recruited participants with mental health problems from general practice report rates of patients declining ranging from less than 1% (Marks et al., 2004) to 26% (Proudfoot et al., 2004). The two studies most similar to the present study that evaluated CCBT for anxiety disorders in a secondary care setting do not report ‘declined’ specifically (Bergström et al., 2010; Hedman et al., 2011). However, combining categories that may potentially overlap with this construct (e.g. not showing up to the interview, not accepting the research protocol/group treatment/randomisation, practical obstacles, unknown or other) suggests that these studies found a broadly similar rate of participants who declined to participate in their studies, for a range of reasons.
In the present study, 10% of those randomised to treatment did not start treatment. Similar studies in secondary care report that between approximately 6% and 20% of participants randomised to computer-based treatment do not commence treatment (Bergström et al., 2010; Hedman et al., 2011). Overall, 65% of patients randomised to treatment completed treatment (GAD 3/4 sessions, panic and social phobia 4/6 sessions). Other studies evaluating CCBT for anxiety have reported rates ranging from 1% (Farvolden et al., 2005) to 90% (Carlbring et al., 2001) for patients completing all treatment sessions. In a naturalistic evaluation of CCBT in a secondary care setting similar to the present study, 71% of participants completed all eight treatment sessions (Learmonth et al., 2008). In a review of the literature, Waller and Gilbody (2009) reported that a median of 56% of patients completed a full course of CCBT for anxiety and/or depression.
The present results suggest that even when patients’ difficulties are such that they are referred to a secondary care service, and when they are offered the chance of free treatment earlier than they would otherwise receive it, a substantial minority will decline this offer or will withdraw from treatment. We are unable to provide a comprehensive account of why patients declined to participate, as patients have the right to decline participation without needing to give a reason why. The most common reason volunteered by patients for not wanting to participate was being ‘too busy’, which is consistent with the reasons provided for not completing treatment. Being ‘too busy’ would be expected to be an obstacle to a range of treatments, and would not be expected to be specific to computerised treatment.
Encouragingly, patient ratings of treatment were typically favourable. This suggests that for patients who were randomised to treatment, computerised treatment was viewed positively and that the treatment itself is acceptable to patients. These findings are consistent with other studies which have found that participants’ perceptions of CCBT are generally positive (Titov et al., 2009).
In conclusion, CCBT was typically rated favourably by patients referred to a secondary care service and randomised to treatment. However, only a small minority of patients was eligible and consenting for the trial. Therefore, while CCBT may be an acceptable treatment, its suitability for secondary care settings remains unclear.
Footnotes
Acknowledgements
The authors wish to thank Cecilia Bourke and Wendy Mayes for the management of this study, and Dr Christopher Frampton for statistical advice. Preliminary findings from this paper were presented at the Department of Psychological Medicine Research Meeting, May 2010.
Funding
This study was supported by the Canterbury District Health Board and was financed by the Canterbury Medical Research Foundation and New Zealand Lottery Grants Board.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.