
Abstract
According to Perez et al., social skills are culturally normative or socially sanctioned interpersonal behaviours that accurately communicate the emotions and needs of the individual in order to facilitate the achievement of interpersonal goals [1]. Social skills can be defined as the set of behaviours that an individual is required to present in a number of situations. This set of behaviours consists of those related to interpersonal skills, interpersonal competence, and communication competence. A comprehensive repertoire of social skills includes a subset of behaviours such as communication skills, civility, empathy and working capacity, as well as the ability to express positive feelings and personal interests [2]. The social skill concept is also related to the capacity to make judgements regarding social conventionality, as well as sensitivity to social cues and an awareness of the consequences of social events.
It is assumed that socially skilled individuals are more productive, and that such individuals enjoy more enduring and satisfactory personal and professional relationships. Deficits in these abilities are typically associated with difficulties and conflicts in interpersonal relationships, lower quality of life, and social isolation [3].
Psychiatric patients often present deficits in social functioning. In recent decades, social training programmes have been developed in order to allow such patients to compensate for these difficulties [4], [5]. Bipolar disorder can lead to psychological and social impairment, because depressive and manic episodes are frequently accompanied by significant behavioural changes that cause occupational and social dysfunction. Even when in remission, patients with bipolar disorder can present social skills deficits [6].
There have been a number of studies evaluating social skills in individuals with schizophrenia [7], [8], depression [2], [9], or anxiety disorders [10], but this topic has rarely been addressed in individuals with bipolar disorder. So far there have been four representative studies evaluating social skills in individuals with bipolar disorder [1], [11–13].
In a study involving patients with bipolar disorder, Scott et al. analysed dysfunctional attitudes that could influence psychosocial adjustment and reported that patients with bipolar disorder presented higher levels of perfectionism, a greater need for approval, a greater over-general recall on autobiographic memory and were less capable in social problem-solving tasks [11]. Patients with bipolar disorder presented less impaired social skills than schizophrenia patients [12].
Goldstein et al. showed that adolescents with bipolar disorder lag behind their peers in social performance but not in knowledge of social skills [13]. The author stated that difficulties in controlling emotions can interfere with the consistent exhibition of appropriate social behaviours.
Perez et al. showed that, in addition to deficits in social functioning, imbalances in social skills are significant indicators of clinical distress in individuals with mood disorder or schizophrenia [1]. The authors used the Social Skills Inventory, an instrument with 90 items developed by Riggio and Carney [14].
In two different studies, Benazzi studied interpersonal rejection sensitivity (IRS) in individuals with bipolar disorder type II and stated that the IRS personality trait seems to be more common in individuals with bipolar disorder type II than in those with unipolar depression [15], [16]. The authors also found that individuals with bipolar disorder type II and IRS were significantly younger, presented lower ages at onset, were more often female, and presented less psychosis than did those with bipolar disorder type II and no IRS [15], [16].
Data from neuroimaging studies provide evidence, such as a decrease in grey matter density in the left anterior cingulate, that certain brain regions are responsible for emotional processes [17].
The aim of the present study was to investigate the perceptions of Brazilian patients with bipolar disorder regarding their social skills and to compare them with those of healthy controls.
Methods
Participants
This study was conducted at the Institute of Psychiatry of the University of São Paulo School of Medicine, in São Paulo, Brazil. Subjects with bipolar disorder were selected from among those treated at the Bipolar Disorder Research Programme Outpatient Clinic. Healthy volunteers were recruited through advertisements in local newspapers. The enrolment period was from 2003 to 2005. For all subjects, the Structured Clinical Interview (SCID) for DSM-IV was used to assess psychiatric histories and diagnoses [18]. To take family histories, the Family History Screen was used [19]. Subjects were selected for inclusion in the bipolar group if they met the DSM-IV criteria for a diagnosis of bipolar disorder type I and the diagnosis was confirmed through the use of the SCID [20]. For all participants, the Hamilton Depression Rating Scale (HAM-D) and the Young Mania Rating Scale (YMRS) were also applied [21], [22]. None of the patients or controls had been diagnosed with substance-induced mood disorder or schizoaffective disorder. Nor did any of the subjects present the following: alcohol or substance abuse/dependence in the preceding 6 months; lifetime history of epilepsy or seizures; or use of topiramate or benzodiazepines in the preceding 2 weeks.
All subjects were evaluated using a self-report questionnaire, the Brazilian Inventário de Habilidades Sociais (IHS, Social Skills Inventory), devised by Del Prette and Del Prette [3], together with the Wechsler Adult Intelligence Scale (WAIS) subtests Comprehension and Picture Arrangement [23]. The two WAIS subtests are also used to assess the ability to analyse social situations and to make judgements, both of which are important aspects of social skills. We found no previous studies in the literature that used the IHS to evaluate psychiatric patients. Therefore, there are no data available regarding social skills variability among such patients in Brazil. In view of this, we decided to obtain the largest sample possible during the enrolment period. The final sample consisted of 56 subjects: 25 patients with bipolar disorder and 31 controls.
Illness characteristics
In the patient group the mean number of previous hospitalizations was 1.28 (SD = 2.4), the mean duration of illness was 9.1 years (SD = 4.9 years), the mean age at onset was 21.1 years (SD = 5.64 years), and the mean number of depressive and manic episodes was 13.8 (SD = 9.55). The mean total HAM-D score was 1.36 (SD = 1.44), and the mean YMRS score was 0.96 (SD = 1.34). Fourteen patients presented psychotic symptoms over the course of the illness. Ten patients presented psychiatric comorbidities: panic disorder, n = 5; obsessive–compulsive disorder, n = 1; previous drug or alcohol abuse, n = 3; and attention deficit–hyperactivity disorder, n = 1. All patients were on medication at the time of testing. Of the 25 patients with bipolar disorder, 14 (56%) were being treated with lithium: six (24%) were receiving lithium as monotherapy and eight (32%) were receiving lithium in combination with antipsychotics, anticonvulsants or antidepressants.
Measures
Social skills assessment
The IHS is a self-report questionnaire composed of 38 items, each describing an interactive social situation and a possible reaction to it (Appendix 1). Examinees are asked to estimate how often they react in a given way. Participants rated their skills in each situation by assigning each statement a score of 0–4 points, ranging from 0, never or rarely, to 4, always or almost always. The items are grouped into five domains.
Domain 1 evaluates assertiveness in interpersonal situations, to safeguard the rights of the individual and maintain self-esteem (e.g. ‘When a friend to whom I've lent some money forgets to give it back, I find a way to remind him/her.’).
In domain 2, which analyses self-confidence in the expression of positive feeling, the items depict the need for positive interpersonal feedback and affirmation of self-worth (e.g. ‘When someone does something I think is good, even if it is not directly related to me, I mention it, praising him/her at the first opportunity’).
Domain 3 evaluates conversational skill and social boldness, and its items portray neutral situations of initial social encounters (e.g. ‘When I am with a person who I have just met, it is difficult for me to keep an interesting conversation going’).
Items in domain 4, which evaluates social openness to new people and new situations, describe situations that involve interacting with new people (e.g. ‘I avoid asking questions of people I don't know’).
The items in domain 5 evaluate self-control of aggressiveness and individual reactions to aversive stimuli that require the management of anger and aggressiveness (e.g. ‘When my schoolmates or work colleagues tease me, I don't let it bother me’).
Social situations and judgement
The WAIS Picture Arrangement subtest evaluates planning involving sequential events. Each item consists of a set of picture cards that tell a story. The cards are presented out of order to the examinee, who is asked to rearrange them in order to create a story that is logical.
The WAIS Comprehension subtest consists of a series of oral questions that require the examinee to understand and articulate social rules/concepts or to provide solutions to everyday problems.
Procedures
A trained psychologist, blinded to participant diagnoses, administered all evaluation instruments used during the study. Clinical data were obtained from the SCID and from medical charts. Patients and controls were carefully screened to ensure that all met the euthymia criteria. The psychiatrists who applied the HAM-D and the YMRS presented high inter-rater reliability for both scales (κ = 0.89).
This study was approved by the local ethics review committee, and written informed consent was obtained from all participants.
Statistical analysis
The normality of the distribution of continuous data was verified using the Kolmogorov–Smirnov test. We compared groups using Student's t-test, because all continuous variables presented a normal distribution. The differences between groups in gender rates were analysed using the χ2 test. Pearson's correlation test was used in order to evaluate the relationship between clinical variables and social skills scores. To compare patients who had anxiety disorder with those who did not, we used the Mann–Whitney U-test.
Results
We studied 25 patients (12 men, 13 women), aged 23–48 years (mean = 33.08 years, SD = 8.5). The mean level of education was 12.6 years of schooling (SD = 1.7), and the average intelligence quotient (IQ) was 101.9 (SD = 9.4). We compared those patients with 31 healthy controls (10 men, 21 women), aged 23–46 years (mean = 35.35 years, SD = 7). Among the controls, the mean level of education was 11.74 years of schooling (SD = 2), and the average IQ was 97.23 (SD = 9.5). There were no significant differences between the two groups in terms of level of education, age, sex, or IQ.
Social skills assessment
As can be seen in Table 1, there was a significant difference between the two groups in terms of the total score on the IHS, primarily due to the scores obtained for domains 3 and 4. The mean total score in the bipolar group was 52.12 (SD = 28.75), compared with 70 (SD = 25.88) in the control group (p = 0.018). The mean domain 3 score in the bipolar group was 61.36 (SD = 33.7) versus 78.26 (SD = 25.72) in the control group (p = 0.038). The mean domain 4 score in the bipolar group was 43.68 (SD = 28.18), compared with 64.94 (SD = 24.81) in the control group (p = 0.004).
Brazilian Social Skills Inventory scores
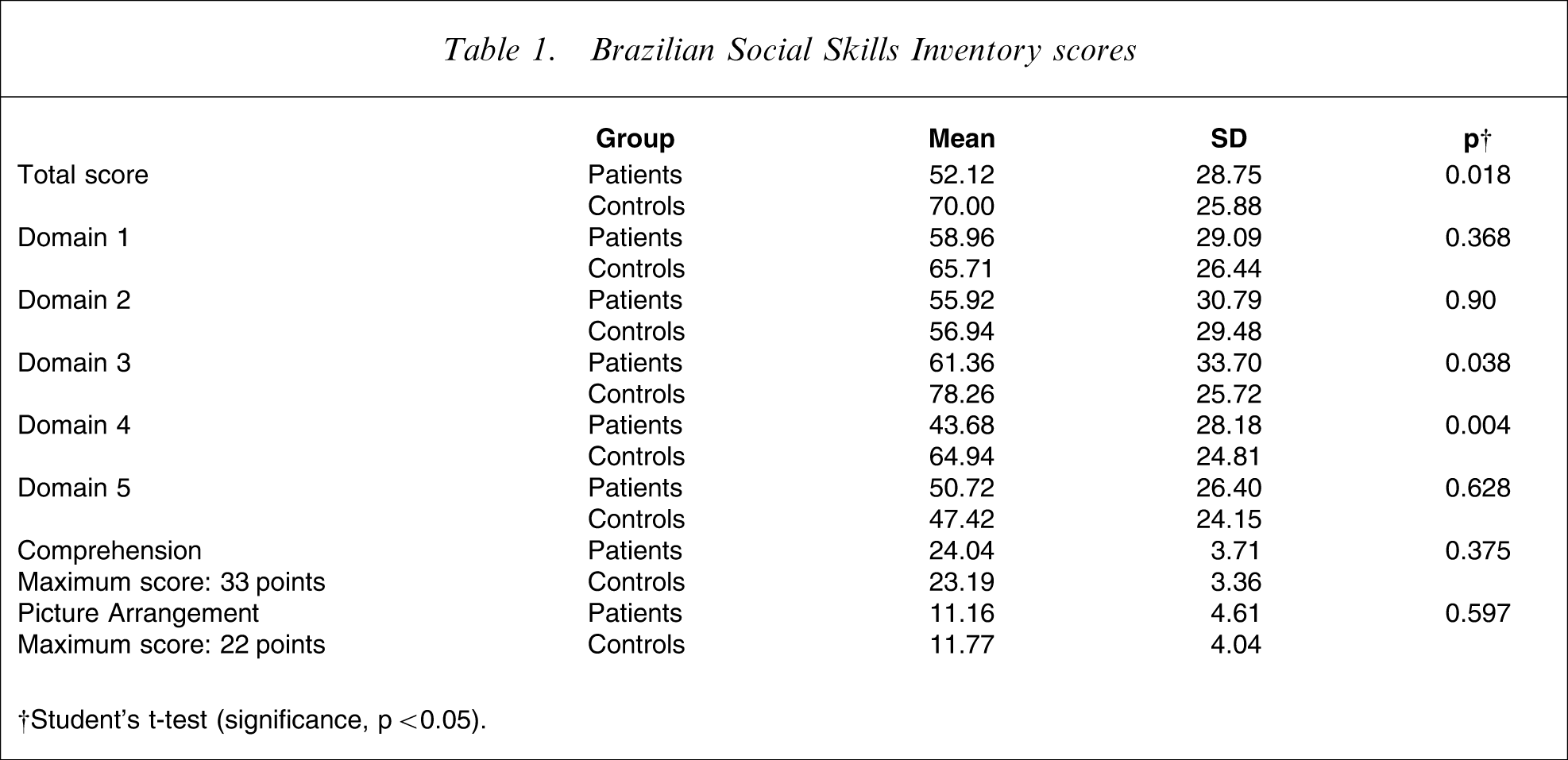
†Student's t-test (significance, p < 0.05).
Social situations and judgement
There were no differences between patients and controls in terms of the scores obtained of the WAIS subtests Comprehension (p = 0.375) and Picture Arrangement (p = 0.597).
There were no significant correlations between the IHS scores and the number of prior hospitalizations (p = 0.399), duration of illness (p = 0.236) or number of prior depressive and manic episodes (p = 0.701). When we compared patients based on lifetime occurrence of psychotic symptoms, we found no differences in the social skill scores (p = 0.697). We found a difference, however, in domain 2, when patients who had anxiety disorders (two men, four women; mean age = 35.83 years, SD = 10.62, mean level of education = 12.33 years of schooling, SD = 1.63) were compared with patients who did not have anxiety disorders (10 men, nine women; mean age = 33.16 years, SD = 7.97, mean level of education = 12.79 years of schooling, SD = 1.75; p = 0.047). Two patients who had anxiety disorders required hospitalization Table 2.
Brazilian Social Skills Inventory scores according to presence of anxiety disorder
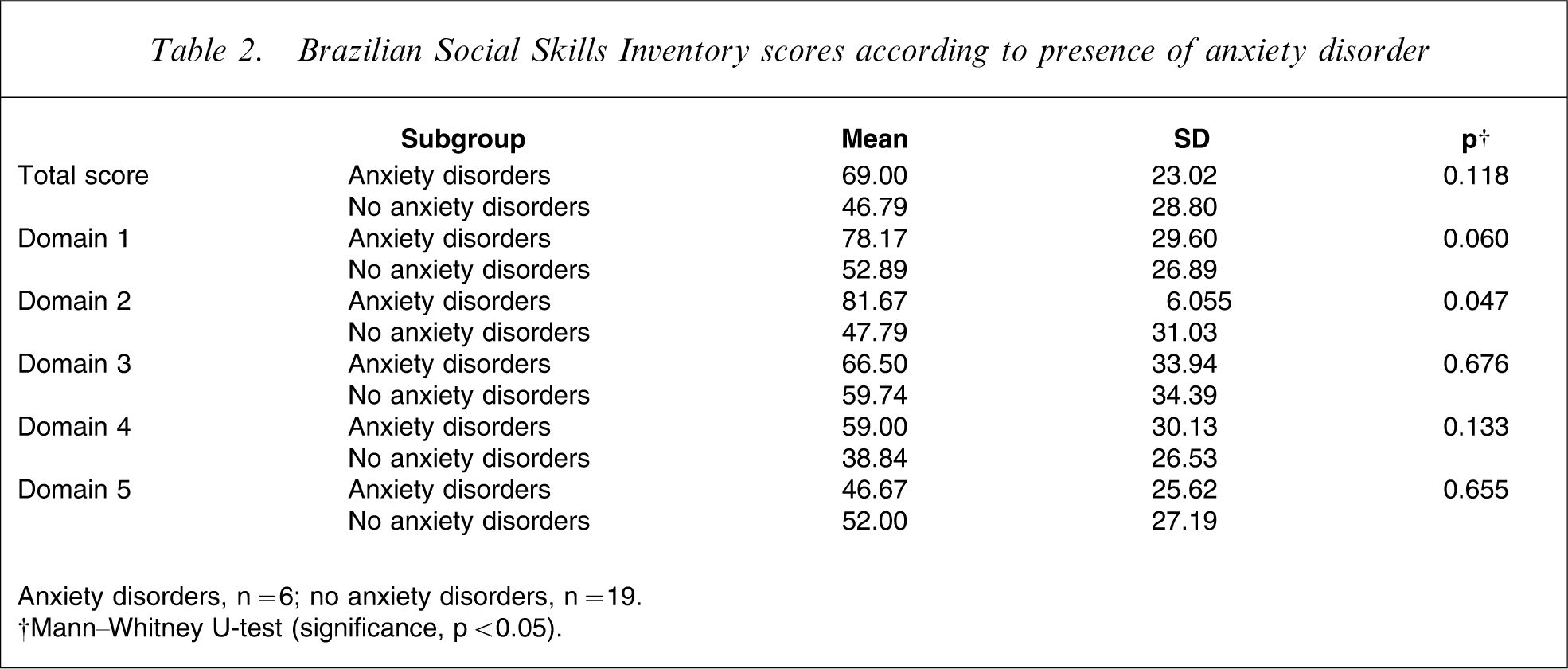
Anxiety disorders, n = 6; no anxiety disorders, n = 19.
†Mann–Whitney U-test (significance, p < 0.05).
Discussion
To our knowledge, this is the first controlled study using the Brazilian IHS to evaluate social skills in a sample of patients with bipolar disorder. We found that there was a significant difference between patients with bipolar disorder and controls in terms of the total IHS score. This difference might be principally attributable to the differences in the scores obtained for domains 3 and 4. Patients scored lower than did controls on questions related to their ability to maintain a conversation and to confront new situations. But we found no significant differences between the two groups in terms of the way the subjects answered questions related to the capacity to discern rules and norms that regulate social situations, as well as those related to perceiving cause-and-effect relationships in social situations.
The present results suggest that patients with bipolar disorder present impairment in the capacity to cope with neutral or adverse social situations. The differences between the two groups in the self-evaluation indicate that individuals with bipolar disorder tend to be more cautious in making social contact and feel uncomfortable when they need to interact in a direct way in interpersonal relationships. Patients with bipolar disorder also seem to be more recalcitrant when they need to approach strangers or cope with new situations, as measured in domain 4. It is of note that the deficits found did not correlate with the clinical variables of the disease, such as duration of illness, number of hospitalizations, number of depressive and manic episodes, or psychotic symptoms.
As stated by Scott et al., individuals with bipolar disorder present higher levels of perfectionism and need for approval, and this might be related to their careful approach to social encounters [11]. Benazzi argued that individuals with bipolar disorder type II can present greater IRS than do those with unipolar depression [15], [16]. In the present study we obtained similar results in our comparison of individuals with bipolar disorder type II and healthy controls. According to Pope et al. it is also possible that people who experience the stigma and loss of social status commonly associated with having a mental illness lose confidence in their ability to initiate and sustain conversations in both neutral and new situations, and that they suffer problems of self-esteem [24].
The IHS domain 1 scores did not differ significantly between patients and controls. Subjects in both groups evaluated themselves as having no difficulties in being assertive. In addition, there was no difference between groups in terms of the domain 2 scores. Individuals with bipolar disorder evaluated themselves as being self-confident and fully capable of expressing positive emotions. Review studies, however, have shown that patients with depressive symptoms have difficulty in being assertive and in expressing positive emotions, and that such patients evaluate themselves in a more negative way than do patients with bipolar disorder [25], [26]. The fact that all patients were found to be euthymic using a very careful assessment might explain our findings in this domain. But subjects with anxiety disorders scored higher for domain 2 than did those without. It has been shown that individuals with anxiety disorders worry more about expressing positive emotions in interpersonal relationships than do those without anxiety disorders. The need to please and to be accepted is more evident in individuals with anxiety disorders.
Self-control of aggressive behaviour, as measured in domain 5, was comparable between the two groups, indicating that patients and controls were able to react to aversive stimuli with reasonable anger control and in a socially competent way. This result is interesting, because impulsivity and irritability can frequently occur over the course of bipolar disorder. In a review article on the impact of depression on social skills, Tse and Bond reported that depressed patients were less cooperative and more exploitive of their partners [9].
An interesting finding of the present study was that the mean number of depressive and manic episodes among the patients was 13.8. Scott and Colom, in their psychotherapy studies, stated that the occurrence of more than 12 episodes is predictive of poorer psychotherapy outcome and represents a severe clinical stage of the illness [27]. Therefore, it might not be possible to generalize the present results to individuals in the earlier stages of bipolar disorder.
One limitation of the present study was the relatively small sample size. But in the patient group we included only individuals in whom a diagnosis of bipolar disorder type I was confirmed through application of the SCID. In addition, patients and controls were carefully screened to ensure that they met the criteria for euthymia. The SCID and rating scales were administered by well-trained clinicians, and the level of inter-rater reliability was high. Furthermore, the two groups were similar in terms of level of education, age, sex and IQ. Moreover, despite the small sample size, we were able to determine the influence that comorbidities had on perceived social deficits. This will be important in future studies, especially in determining the impact of comorbid anxiety disorder on social skills in representative samples.
The assessment of social skills is important considering the effect that they have on the quality of life of psychiatric patients. The data obtained through the use of the IHS can inform decisions regarding more specific therapeutic requirements. Various social skills training programmes for depressed patients have focussed on many of the aspects addressed by the inventory [25], [26].
Conclusion
The present results suggest that euthymic patients with bipolar disorder have specific difficulties in social skills, presenting inhibited and overattentive behaviour in relation to other people and their environment. These deficits can have a negative impact on their level of social functioning and quality of life. Further investigations into the mechanisms of these impairments are essential in order to establish specific targets for the development of cognitive behavioural therapies and to improve social training programmes for patients with bipolar disorder.
Footnotes
Appendix 1.
Brazilian Inventário de Habilidades Sociais (HIS, Social Skills Inventory)[3]
1. In a group of people who I am not acquainted with, I feel comfortable and speak naturally.
2. When a member of my family keeps telling me what I have to do, contradicting the way I think, I accept it to avoid problems.
3. When I am wholeheartedly praised by someone, I thank him/her in reply.
4. In a conversation, if someone interrupts me, I ask him/her to wait until I finish my sentence.
5. When a friend to whom I've lent some money forgets to give it back, I find a way to remind him/her
6. When someone does something I think is good, even if it is not directly related to me, I mention it, praising him/her at the first opportunity.
7. If I feel like getting to know someone to whom I was not introduced before, I introduce myself.
8. When I am among schoolmates or work colleagues, I have difficulty in joining the conversation (get-together).
9. I avoid making speeches or giving lectures in front of strangers.
10. At home, I express feelings of affection for my family through words and gestures.
11. In a class or meeting, when the teacher or a superior makes an inaccurate statement, I speak out and state my point of view.
12. If I am interested in having a sexual relationship with someone, I can approach her/him to start a conversation.
13. If someone praises me at work or at school, I blush, and I don't know what to say.
14. When I am required to make a speech in a classroom or at work (for example, a lecture), I do it.
15. When a relative criticizes me unfairly, I express my annoyance directly.
16. If I'm in a group of acquaintances and I disagree with the majority, I express it verbally.
17. In a conversation with friends, I have difficulty in ending the conversation and I prefer to wait for the others to do so first.
18. When one of my relatives, for some reason, criticizes me, I react in an aggressive way.
19. Even when I am very close to an important person whom I would like to meet, I have difficulty in approaching him/her to initiate a conversation.
20. When I fall in love with someone I have been going out with, I take the initiative to express my feelings to him/her.
21. When I receive a damaged product, I go to the store where I bought it and I demand they replace it.
22. When requested by a friend to put his/her name on work done without his/her participation, I end up doing so, even thinking it is not right.
23. I avoid asking questions of people I don't know.
24. I have difficulty in ending a telephone conversation, even with someone I know.
25. When I am criticized in a direct and fair way, I am able to control myself, admitting my mistakes or explaining my point of view.
26. In charitable campaigns, I avoid tasks that involve asking strangers for donations or favours.
27. If a friend takes advantage of my generosity, I directly express my displeasure to him/her.
28. When a member of my family (child, parent, sibling, spouse etc.) achieves something important to which he/she has been dedicating a lot of effort, I praise him/her for his/her achievement.
29. At school or at work, when I don't understand an explanation about something in which I am interested, I ask the questions that I believe are necessary for me to understand.
30. In a group situation, when someone is being treated unjustly, I rush to his/her defence.
31. When I enter a place where there are many new people, I greet them.
32. When I feel I need help, I can easily ask for help among my circle of friends.
33. When my partner insists on having sex without a condom, I agree in order to avoid him/her getting irritated or hurt.
34. At work or at school, I agree to do tasks that are requested and are not my obligation, even when I feel that I am being taken advantage of.
35. If I am feeling well (happy), I express it among my circle of friends.
36. When I am with a person who I have just met, I find it difficult to keep an interesting conversation going.
37. If I need to ask a favour of a colleague, I end up not doing so.
38. When my schoolmates or work colleagues tease me, I don't let it bother me.