
Abstract
Objectives:
Few studies of neuropsychological function in major depression have examined emotional processing or the impact of gender. Patients have also been compared with highly selected control participants and rarely with other patient groups. The objective of this study was to compare neuropsychological function in a major depressive episode (MDE) with a group of patients with an anxiety disorder, social anxiety disorder (SAD), and healthy controls, to include measures of emotional processing and to analyse the effects of gender on neuropsychological function and emotional processing in these groups.
Method:
One hundred and one medication-free patients with MDE, 30 patients with SAD and 76 healthy control participants were recruited. The groups were matched for age and estimated premorbid intelligence and education. Subjects performed a battery of neuropsychological tests assessing; verbal learning and memory, visuospatial learning and memory, attention, executive function and psychomotor performance. They also performed a task measuring the accuracy of recognition of facial emotional expressions.
Results:
Compared with healthy participants and those with SAD, patients with MDE were significantly impaired in verbal learning and spatial working memory. The SAD group misclassified significantly more neutral expressions as angry and fewer as sad, compared with the MDE group and healthy controls, but there were no significant differences between the MDE group and healthy controls. The profile of performance was the same regardless of gender.
Conclusions:
The study confirms a significant impairment in neuropsychological function in a clinical sample of outpatients with MDE, which is likely to have important implications for day-to-day functioning and treatment.
Introduction
Many studies have investigated aspects of neuropsychological impairment during episodes of major depression, including the pattern and magnitude of impairment, the specific domains affected and the origin of these abnormalities (Porter et al., 2007). However, there are several unanswered questions in this area, among which are the following.
First, the specificity of neuropsychological deficits in major depression remains unclear since few studies have specifically compared the neuropsychological profile of depression with other psychiatric disorders. Previous studies might be criticised on the grounds that they use a ‘supernormal’ control group of participants specifically selected for the absence of any complicating co-morbid condition and often for the absence of a family history of affective disorder. This may have led to overestimating the functional importance of neuropsychological impairment in depression. Second, despite an increase in interest in emotional processing in depression, and in particular facial emotion processing (Bourke et al., 2010; Harmer et al., 2009), there has been only one previous study of this in a large sample of depressed patients (Douglas and Porter, 2010). Third, the effects of gender on neuropsychological function in depression have not been explicitly studied. This is of interest given the gender differences in the prevalence of depression (Kessler, 2003), the relationship between hormonal fluctuations, mood symptoms and neuropsychological function in females (Symonds et al., 2004), and the known differences in neuropsychological functioning between males and females (Postma et al., 2004).
The present study, involving a large group of medication-free depressed outpatients, addressed these limitations in the following ways. First, we compared patients with a major depressive episode (MDE) with a comparison group of patients with social anxiety disorder (SAD) as well as a healthy control group. Although there is a degree of conflicting evidence regarding the neuropsychological profile of anxiety disorders, clearly the deficits are subtle. This makes it potentially a group of subjects which is not highly selected for superior psychological health, but which is unlikely to have major neuropsychological deficit. Within anxiety disorders, SAD is the predominant condition and therefore was chosen as a comparison group. Second, as well as examining neuropsychological function, we examined emotional processing using a facial emotion processing task in the test battery. Third, we included gender as a factor in all analyses.
Methods
Participants
Depressed outpatients aged between 18 and 65 years with a Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV)-defined episode of major depression without psychotic features (single or recurrent major depressive disorder or bipolar II depression), were included in the study. Patients were recruited from general practice clinics and tertiary mental health services in Christchurch, New Zealand, or were referrals by self, family or friends. Apart from the occasional hypnotic, depressed patients were psychotropic medication-free for at least 6 weeks prior to recruitment. Diagnoses were established using the Structured Clinical Interview for DSM-IV Axis I Disorders Patient Edition (First et al., 1998). Depressed patients were excluded from the study if they had bipolar I disorder, schizophrenia, current moderate or severe alcohol or drug dependence, history of head injury, neurological illness or any serious physical illness. Patients with alcohol or drug abuse, or mild dependence were not excluded. Severity of depression was evaluated using the Montgomery–Åsberg Depression Rating Scale (MADRS) (Montgomery and Åsberg, 1979) and the 17-item Hamilton Depression Rating Scale (HDRS17) (Hamilton, 1960).
Individuals aged between 18 and 65 years with SAD (generalised) were recruited through an article in the local newspaper describing the symptoms of SAD, or through referrals to the Anxiety Disorders Unit (a publicly funded tertiary outpatient service in Christchurch, New Zealand). They were diagnosed with SAD according to the DSM-IV criteria using the Structured Clinical Interview for DSM-IV Axis I Disorders Patient Edition (First et al., 1998). Individuals with SAD were excluded from the study if they had any other current (but not lifetime) Axis I disorders, history of head injury, neurological illness or any serious physical illness. Individuals with remitted depression who were taking antidepressant medication were not excluded from the study.
Healthy control participants were recruited through newspaper and radio advertisements and assessed using the Mini International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998). They were excluded if they met the criteria for any current or past psychiatric disorder, had a history of head injury, neurological disorder or any serious physical illness, or if they had a first degree relative with a history of any Axis I disorder.
As far as possible, groups were matched for age, gender, ethnicity, estimated premorbid intelligence quotient (IQ) [National Adult Reading Test (NART); Nelson, 1982] and years of formal education. Females were matched for phase of menstrual cycle at testing. All participants spoke English as their first language or were bilingual from childhood and fluent in English. The study was approved by the Upper South B Canterbury Regional Ethics Committee and written informed consent was given by all participants.
Neuropsychological assessment
Participants commenced neuropsychological testing at 13:00 h following a light lunch. Testing took approximately 100 min. Pencil-and-paper tests were administered according to standardised instructions (Lezak et al., 2004). Computerised tests from the Cambridge Neuropsychological Test Automated Battery (CANTAB) (Cambridge Cognition Limited, 2007) were administered according to CANTAB manual protocols on a laptop fitted with a colour touch screen monitor. The recognition components of the two verbal learning and memory tests, and a simple reaction time test, were administered using the experimental laboratory software SuperLab version 2 (Cedrus Corporation, San Pedro, California, USA). The tests used are briefly summarised below.
To measure the state of anxiety during neuropsychological testing, the three groups completed a visual analogue scale (VAS) at five time points. The VAS was designed to measure the magnitude of participants’ current anxiety and consisted of a horizontal line 100 mm in length anchored by the descriptor words ‘not at all anxious’ at one end of the scale and ‘worst anxiety ever’ at the other end of the scale. Participants were instructed to rate how anxious they felt currently by drawing a perpendicular line somewhere along the scale from 0 mm to 100 mm.
Verbal learning and memory
Rey Auditory Verbal Learning Task
The Rey Auditory Verbal Learning Test (RAVLT; Rey, 1964) assesses verbal learning and memory. For the present study, the recognition component of the RAVLT was presented as a computerised test using SuperLab version 2.0 to assess reaction time and recognition accuracy.
Consonant-vowel-consonant auditory verbal learning test
The consonant-vowel-consonant (CVC) verbal learning test was identical in format, administration and scoring to the RAVLT, except that ‘nonwords’ were presented instead of words with semantic meaning. The monosyllabic nonwords selected from the ARC Nonword Database (Rastle et al., 2002) used in the CVC test had no semantic meaning in the English language. Therefore, this test provided less opportunity than the RAVLT to access learning and mnemonic strategies, thus providing a mechanism to study verbal learning and memory functioning while controlling for the effects of semantic meaning. Two lists of 15 nonwords were compiled, each nonword comprising three letters, beginning and ending with different consonants, with a vowel as the middle letter.
As performance on the final two recall trials of list A depends on how well the words are learned initially, post-distracter scores were transformed as a percentage of the average number of words recalled on the first five trials, both for this test and for the RAVLT.
Visuospatial learning and memory
CANTAB Pattern Recognition Memory test
For the CANTAB Pattern Recognition Memory (PRM) test, participants first learned a series of 12 complex patterns before being presented with pairs of patterns, of which the index pattern must be discriminated from the distracter pattern. Accuracy and reaction time are reported for the two sets of 12 patterns.
CANTAB Spatial Recognition Memory test
For the CANTAB Spatial Recognition Memory (SRM) test, participants learned the spatial location of five squares presented sequentially at different on-screen locations. Pairs of squares were presented and participants identified which of the two squares was in the index location by touching the correct square. Accuracy and reaction time were reported for the four trials.
Attention and executive functioning
Controlled Oral Word Association Test (Benton, 1976)
For the Controlled Oral Word Association Test (COWAT), participants generated words beginning with the letters ‘F’, ‘A’ and ‘S’ over a 1-min period for each letter. Rules included exclusion of proper nouns, place names, or the same word with a different ending.
Digit Span Forwards and Backwards (Wechsler, 1997)
Participants recited increasing lengths of digit series, either forwards or backwards, until a pair of sequences was incorrect or a nine-digit sequence was completed correctly.
CANTAB Spatial Span
For the CANTAB Spatial Span (SSP) test, participants remembered the order of nine white squares on screen that changed colour one by one. Trials progressed from two to nine squares and the test self-terminated after three successive trial failures on a given number of squares. The longest span length correctly recalled was reported.
CANTAB Spatial Working Memory
For the CANTAB Spatial Working Memory (SWM) test, participants searched through on-screen boxes to find a blue token, beginning with four trials of four boxes, progressing to four trials of six then eight boxes. Repetitious search errors were reported and an efficiency index for search strategy was generated.
Psychomotor performance
CANTAB Motor Screening Test
This motor screening test (MOT) screens for motor and visual disorders, and served as training for CANTAB (use of the touch screen). Participants touched a series of pink and green crosses as they appeared on the screen. The mean reaction time (ms) to correctly respond to each of 10 crosses was recorded.
Simple reaction time test
This test was developed for the present study as an additional test of psychomotor speed and as a control task for the Facial Expression Recognition Task. Participants were presented with 28 numbers from 1 to 7, followed by words (anger, happy, sad, surprise, disgust, fearful and neutral) in random order for 500 ms. Participants pressed the corresponding labelled key on a response box. Mean reaction time (ms) to respond was recorded.
Facial emotion processing
Facial Expression Recognition Task (SuperLab version 2)
This computerised facial emotion processing task featured facial expressions of six primary emotions (happiness, sadness, surprise, fear, anger and disgust). The task was developed at Oxford University, UK, using similar photographs to those from the Pictures of Affect Series (Ekman and Friesen, 1975). The black and white photographs of facial expressions had been morphed in 10% steps between each prototype and neutral, using techniques similar to those developed by Young et al., (1997).
Four examples of each of the six emotional categories (portrayed by male and female actors) at each level of intensity were given (40 stimuli for each emotion). Each face was also presented in a neutral expression (24 stimuli), giving a total of 264 stimulus presentations. The task was broken down into three blocks (88 stimulus presentations per block) with an untimed rest period between each block to prevent fatigue. Each face was presented in random order for 500 ms and was immediately replaced with a blank screen. On identification of the emotional expression, participants pressed the corresponding labelled key on a response box. Accuracy, mean reaction time (ms) and misclassification errors for neutral expressions (percentage of neutral expressions misclassified as each emotion category) were the outcome measures.
Statistical analysis
Demographic and neuropsychological data were compared using analysis of variance (ANOVA) with group (MDE, SAD, healthy control) and gender as between-subject factors. Where tests had more than one level, an additional within-subject factor of ‘problem difficulty’ or ‘trial’ was added and analysis carried out by repeated measures ANOVA, within a multivariate general linear model. Degrees of freedom were adjusted using the Huynh-Feldt epsilon if the assumption of sphericity was violated. For clarity, unadjusted degrees of freedom are reported. To reduce skewness, errors on the SWM test were square root transformed. Estimates of effect size were calculated for untransformed data using the formula ( x– diff -x– diff)/σ pooled. Statistical analyses were carried out using SPSS version 13.0 (SPSS Inc., Chicago, Illinois, USA). Post hoc ANOVAs were used to compare individual groups where a group effect was found in the primary ANOVA. Further post hoc analyses of covariance (ANCOVAs) were used to compare the performance of three groups, MDE without co-morbid SAD, MDE with co-morbid SAD and SAD, with the covariate HDRS17 score. In keeping with the literature in this field, we chose not to use a Bonferroni correction for multiple comparisons but instead to examine the pattern of results and interpret results which do not fit within an overall domain pattern with caution.
Results
One hundred and one patients with a MDE (MDE n = 93; bipolar II disorder n = 8) were recruited. Current co-morbid psychiatric disorders among depressed patients included anxiety disorders (SAD n = 30; panic disorder n = 17; post-traumatic stress disorder n = 11; obsessive compulsive disorder n = 2; specific phobia n = 17), alcohol abuse (n = 4) or mild alcohol dependence (n = 9) and bulimia nervosa (n = 3). Thirty patients with SAD were recruited. Thirteen patients in the SAD group met the diagnostic criteria for a lifetime history of major depressive disorder, although all were in remission. Nine patients with SAD were taking antidepressant medication (n = 7) or benzodiazepines (n = 2).
Patients were matched with a control group of 76 healthy participants. Age (F = 0.96, df = 2,206, p = 0.90), NART estimated verbal IQ (F2,206 = 1.59, p = 0 .20), years of formal education (K2 = 2.13, p = 0 .34), and for female participants, phase of menstrual cycle (
Demographic characteristics of patient groups and matched healthy controls.
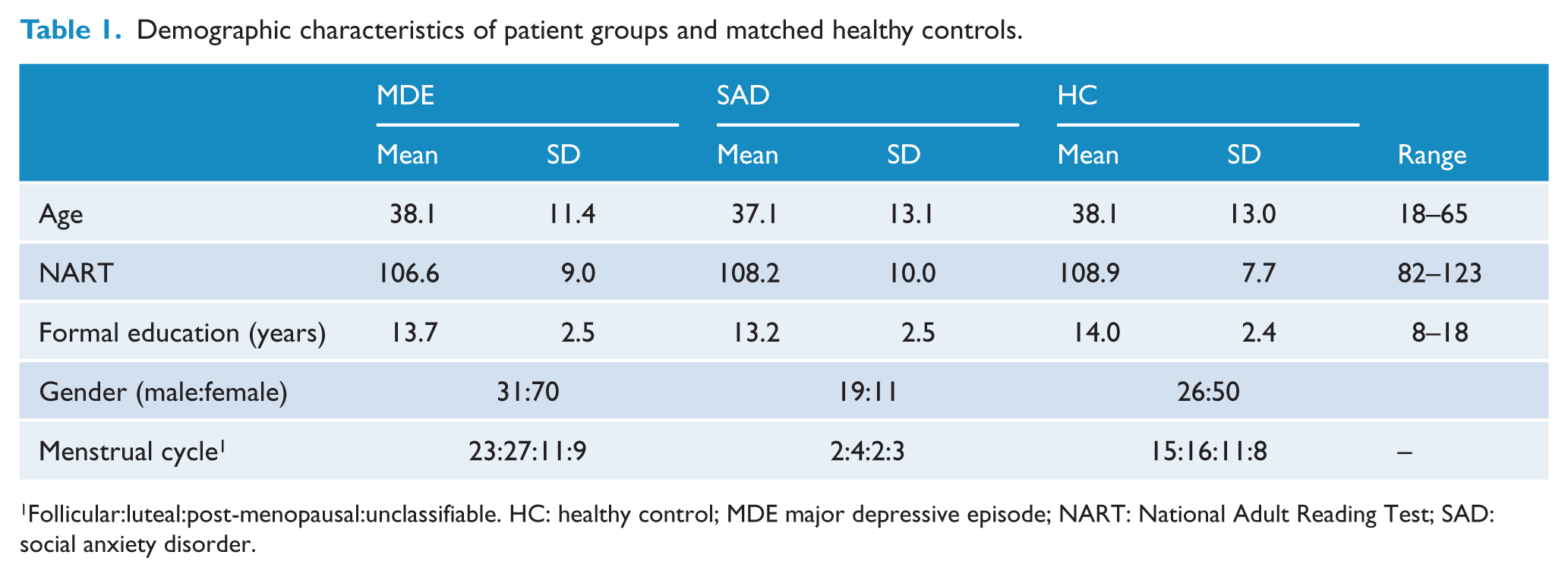
Follicular:luteal:post-menopausal:unclassifiable. HC: healthy control; MDE major depressive episode; NART: National Adult Reading Test; SAD: social anxiety disorder.
Patient groups: illness characteristics and rating scale scores.
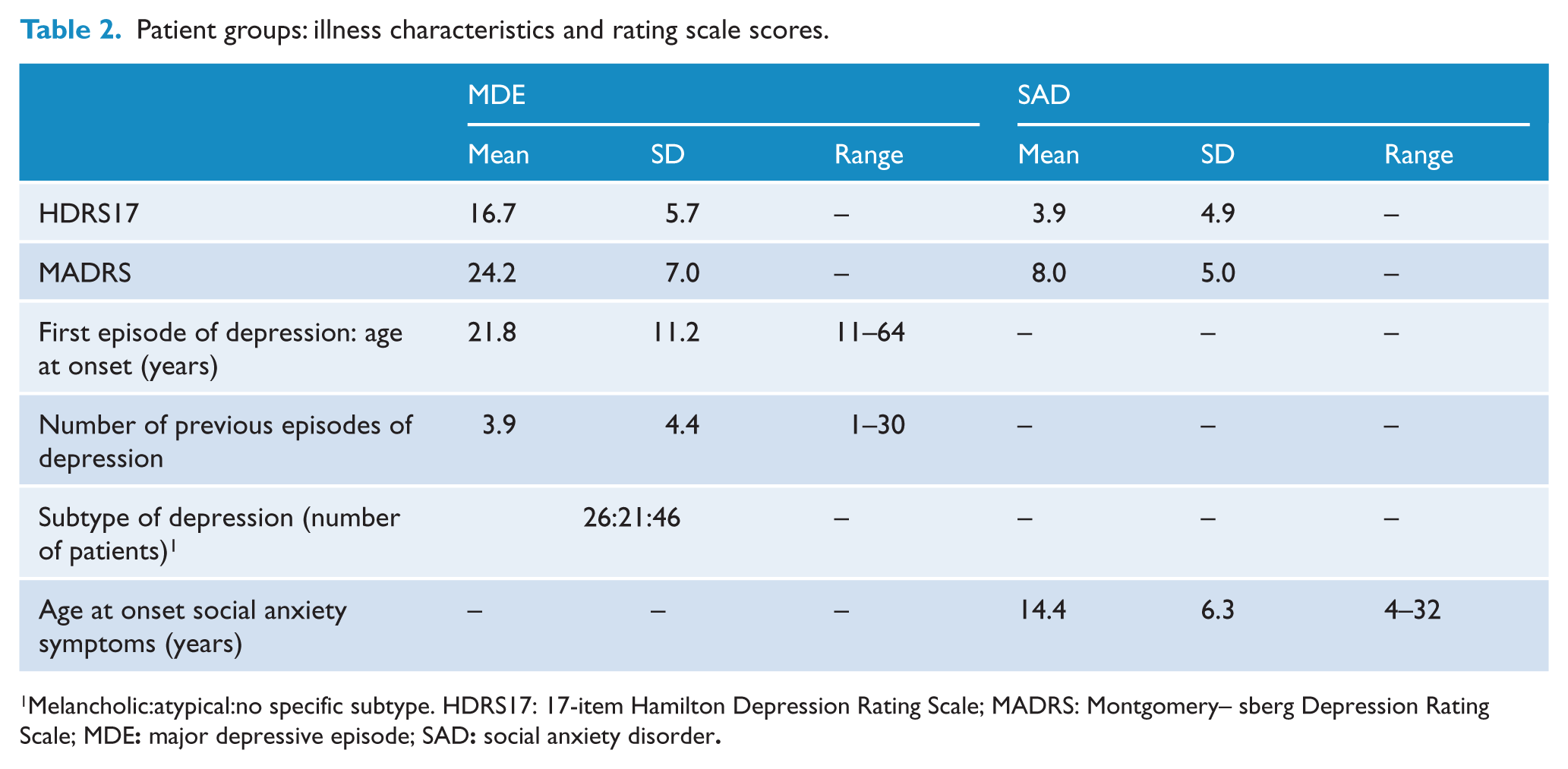
Melancholic:atypical:no specific subtype. HDRS17: 17-item Hamilton Depression Rating Scale; MADRS: Montgomery–Ǻsberg Depression Rating Scale; MDE: major depressive episode; SAD: social anxiety disorder.
The percentage of depressed patients who smoked cigarettes (17.8%) was significantly higher (
Neuropsychological test performance
Due to technical failure there are missing data for all of CANTAB MOT, PRM, SRM, SSP, SWM (one participant); Facial Expression Recognition Task (one participant); simple reaction time test (11 participants); CVC recognition memory (three participants).
Test results are presented in Table 3. Effect sizes for between-group comparisons are given for the comparisons between MDE and the other two groups. Only significant results are reported in the text.
Neuropsychological test results and effect sizes.
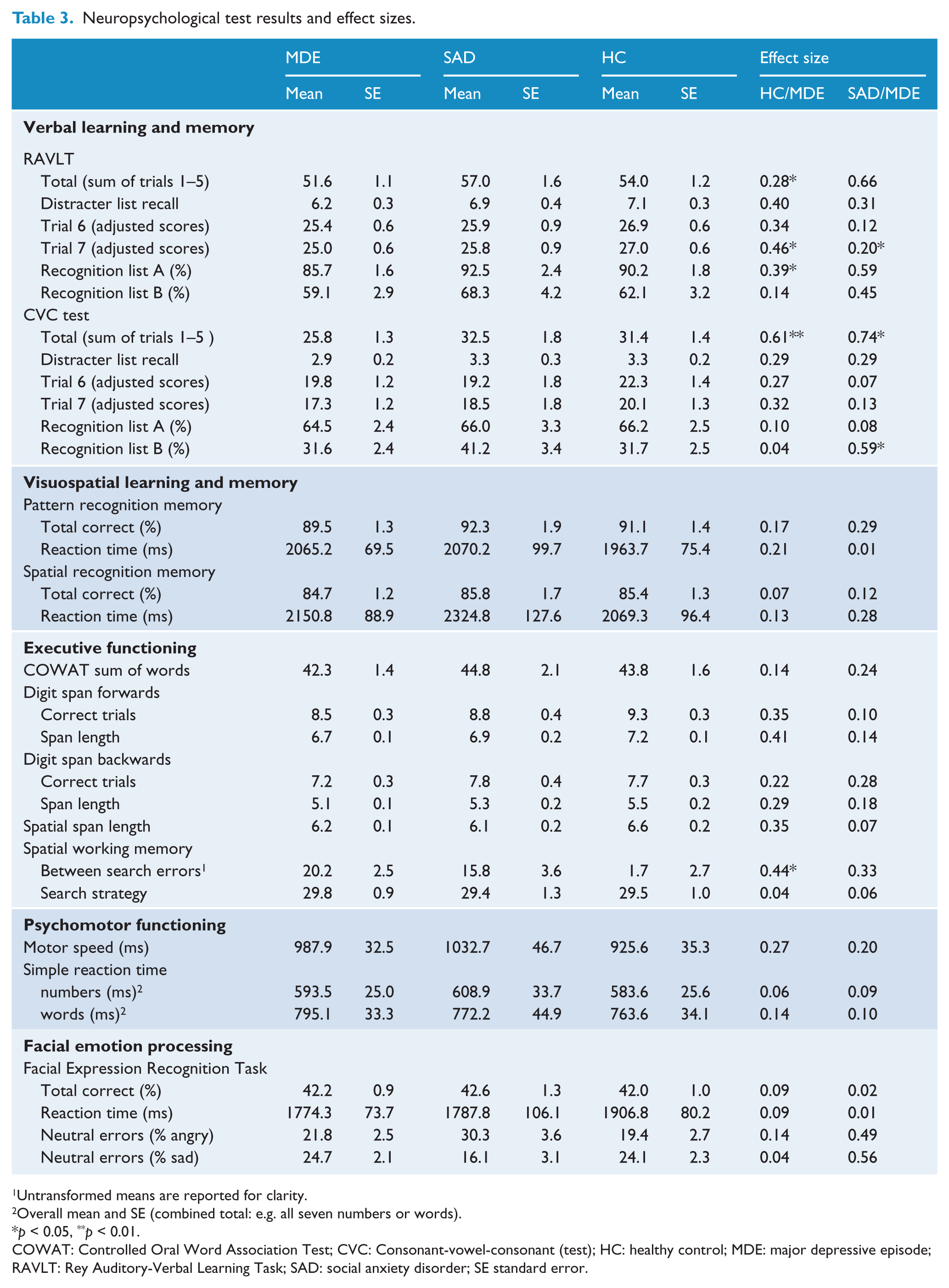
Untransformed means are reported for clarity.
Overall mean and SE (combined total: e.g. all seven numbers or words).
p < 0.05, **p < 0.01.
COWAT: Controlled Oral Word Association Test; CVC: Consonant-vowel-consonant (test); HC: healthy control; MDE: major depressive episode; RAVLT: Rey Auditory-Verbal Learning Task; SAD: social anxiety disorder; SE standard error.
There were gender effects on several tests (data available from the authors by request), but in no case was there a significant group by gender interaction. There were no significant effects of smoking.
Except for error scores, test results were normally distributed.
Verbal learning and memory
Rey Auditory Verbal Learning Task – recall and recognition
There was a significant effect of group for recall of trials 1–5 (F2,199 = 4.703, p = 0.01), with depressed patients recalling fewer total words than healthy controls (p = 0.02) and patients with SAD (p > 0.05). The interaction between group and trial was not significant (F8,796 = 1.021, p = 0.41), thus indicating no difference in the magnitude of the learning curves between groups. Performance on trial 7 (adjusted for scores on trials 1–5) was significantly lower in depressed patients compared with healthy controls (F2,199 = 3.151, p = 0.04). For RAVLT recognition, depressed patients recognised significantly fewer list A words (F2,199 = 4.374, p = 0.01) than healthy controls (p = 0.02).
Consonant-vowel-consonant auditory verbal learning test – recall and recognition
For recall of trials 1–5 there was a significant effect of group (F2,199 = 8.188, p < 0.001), with depressed patients recalling fewer nonwords than healthy controls (p < 0.001) and patients with SAD (p = 0.002).There was a significant interaction between group and trial (F8,796 = 2.739, p = 0.007), suggesting a difference in the learning curves between the groups with reduced learning (flatter curve) in depressed patients. There was no group effect on the adjusted trial 7 scores (F2,199 = 1.459, p = 0.232 ).
There was a significant effect of state anxiety on trials 1–5 (F1,199 = 6.659, p = 0.01). The group by trial interaction and the group effect were still highly significant when this was taken into account.
There was no significant group effect on recognition accuracy of list A nonwords (F2,196 = 0.168, p = 0.84), but there was a significant group effect for distracter list nonwords (F2,196 = 4.084, p = 0.01). Depressed patients recognised fewer distracter list nonwords than patients with SAD (p = 0.04), but not healthy controls (p = 0.93).
Attention and executive functioning
CANTAB Spatial Working Memory
There was a significant effect of group for total between-search errors (F2,198 = 3.091, p = 0.04). Pairwise comparisons showed that depressed patients made significantly more between-search errors than healthy controls (p = 0.02),
Facial emotion processing
Facial Expression Recognition Task
There were no significant interactions between group and emotion for accuracy (F12,1188 = 0.521, p = 0.87) or reaction time (F12,1188 = 0.405, p = 0.95). Separate analysis of intensity of emotional expressions (low ≤ 50% and high > 50%) showed that emotional intensity did not affect accuracy differentially between groups (F10,990 = 0.880, p = 0.55).
There was a significant interaction between group and emotion for misclassification of neutral expressions (F = 2.114, df = 10, 990, p = 0.039), and separate ANOVAs for each emotion showed differences between the groups for angry (F2,198 = 3.926, p = 0.021) and sad (F2,198 = 3.574, p = 0.030) misclassification errors. Pairwise comparisons showed that patients with SAD misclassified more neutral expressions as angry and fewer as sad, compared with depressed patients and healthy controls but there were no significant differences between depressed patients and healthy controls for misclassification of neutral faces to any emotional category.
There were no significant gender effects for accuracy of emotion identification or reaction time; however, females misclassified a significantly higher proportion of neutral expressions as happy than males (F1,198 = 7.211, p = 0.008, effect size = 0.44).
Co-morbid major depressive disorder and social anxiety disorder
Because 30 patients with MDE had co-morbid SAD, we conducted a post hoc ANCOVA to determine whether there was a difference in performance between the group with MDE alone, SAD alone and both MDE and SAD. The HDRS17 score was entered as a covariate. There was no effect of group on any of the measures of neuropsychological function or emotional processing.
Several clinical variables and co-morbidities were present at low frequency in the MDE group. Because of the low numbers, the impact could only be explored by excluding those cases in sub-analyses. In separate analyses the following were excluded from the MDE group: (1) bipolar disorder (n = 8) and (2) alcohol abuse/dependence (n = 13). These exclusions made no difference to any of the results.
Discussion
The main findings of this study are as follows:
The MDE group showed a deficit in aspects of verbal memory compared with controls and SAD. This was most evident when verbal learning was tested using the CVC test.
The MDE group showed no abnormalities in accuracy of recognition of facial expressions of emotion or response bias in misclassification of neutral expressions.
The pattern of impairment in MDE was not dependent on gender.
The MDE group had a statistically significant impairment in spatial working memory. This was an isolated finding in the executive domain and should be interpreted with caution.
The SAD group showed a bias in processing of neutral faces, being more likely than the other two groups to misclassify these as angry and less likely to misclassify them as sad.
Verbal learning and memory
Depressed patients had significantly reduced scores on both verbal learning tests. For the CVC test this was greatest for the total number of words recalled on trials 1–5 with an effect size of 0.61 and a total difference over the five trials of approximately eight nonwords recalled between depressed and healthy controls or patients with SAD. We also noted on this task only that there was a significant effect of state anxiety, with poorer performance related to greater anxiety. On the RAVLT there was also a significant difference between depressed patients and healthy controls but with a smaller effect size (0.28). Findings related to whether these effects involved ‘learning’ as well as working memory were conflicting. No ‘learning effect’ (trial by group interaction) was found on the RAVLT but there was a significant effect of group on the delayed recall when adjusted for recall on the first five lists. For the CVC test there was a ‘learning effect’ but no effect on the delayed recall when adjusted.
While studies involving similar patients with similar depression severity (Grant et al., 2001; Gualtieri et al., 2006; Porter et al., 2003) have not shown significant effects on verbal learning and memory, it is likely that sample size and the tests used are the major factors leading to inconsistencies in findings. For example, the depressed groups in the Gualtieri et al., (2006) and Porter et al., (2003) studies involved depressed samples of 38 and 44 participants respectively, thus affecting the power to detect differences between the groups. In the study by Grant et al., (2001) the shorter 12-word Hopkins Verbal Learning Test was used, increasing the likelihood that ceiling effects reduced the sensitivity of the task.
In contrast to the depressed group, patients with SAD did not show deficits in verbal learning and memory compared with healthy controls. While this lack of effect could be attributed to smaller numbers, the performance of patients with SAD was generally slightly better than that of the healthy controls, particularly on the RAVLT. This finding is in contrast to the study by Airaksinen et al., (2005) in which impaired episodic memory was reported in a group of patients with SAD. It is possible that sample characteristics may explain the differences in findings. For example, all but two patients with SAD in the present study were assessed as moderately or mildly socially anxious, with minimal functional impairment (i.e. most were employed), and none had any current co-morbid Axis I disorders. In contrast, the Airaksinen et al., (2005) study recruited individuals with anxiety disorders and other co-morbid Axis I disorders, thus making it difficult to determine whether the verbal learning and memory deficits were associated with SAD or another co-morbid disorder, such as MDE. In our post hoc analysis separating out the patients with co-morbid MDE and SAD, there was no group effect, suggesting that those patients with co-morbidity perform similarly to those with MDE alone, i.e. the addition of SAD has neither a significant adverse or protective effect.
The moderately large effect size difference between MDE and SAD/healthy controls on the CVC test should be viewed in the clinical context. This was a clinical study in which there were relatively few exclusion criteria and a high degree of co-morbidity. The reason for this was partly that MDE subjects entered a treatment trial which was intended to be a pragmatic trial and partly because the underlying aim of the study was to examine neuropsychological dysfunction in a real group of patients with MDE rather than a highly selected group. The addition of the SAD group was also an attempt to avoid a supernormal comparison group. In order to avoid contamination by patients who may be obviously different, we repeated the analysis having excluded bipolar patients and in another analysis having excluded patients with alcohol abuse or mild dependence. This did not affect the results. In the SAD group, there were 13 patients with a history of depression and nine on medication. These factors, however, would be expected to close the gap between MDE and SAD and make our conclusions more conservative. Overall, in a real clinical sample of patients with MDE compared with controls and compared with a comparison group of patients with SAD who were not screened to be a particularly pure group, there was still a very important deficit in verbal memory.
Executive functioning
Poorer performance of the MDE group on SWM, compared with healthy controls, is consistent with previous studies reporting impaired spatial working memory in mild to moderately depressed groups (Porter et al., 2003; Taylor Tavares et al., 2007). A larger effect size for between-search errors (0.67) was reported by Porter et al., (2003) than that found in the present study (0.44), which may be due to the greater severity of depression in the participants in the study by Porter and colleagues. However, the relationship between severity of depression and neuropsychological impairment in depression is not clear, largely due to the heterogeneity of the disorder and the methodological differences between studies (McDermott and Ebmeier, 2009).
With the exception of SWM, MDE patients in the present study showed no other deficits in executive functioning and no deficits in psychomotor speed or visuospatial learning and memory. The absence of group differences across these domains is in contrast to previous studies of medication-free, mild to moderately depressed outpatients. Most studies have reported executive function or attention deficits, (Grant et al., 2001; Gualtieri et al., 2006; Merriam et al., 1999; Porter et al., 2003; Taylor Tavares et al., 2007) or visuospatial learning and memory deficits (Porter et al., 2003, Taylor Tavares et al., 2007). Differences in severity of depression, even among less severely depressed groups of outpatients, and differences in the tests used to evaluate aspects of executive functioning, may explain the variable findings.
We note that the study examined a large number of variables. The problems inherent in analyses of multiple variables was not corrected for in the analysis because we believe that it is preferable not to correct statistically, but to interpret with caution statistically significant results which do not fit within the overall pattern of impairment. The statistically significantly poorer performance of the MDE group on SWM is not in keeping with other results in the executive domain and may therefore represent a chance finding secondary to the analysis of a large number of variables.
Facial emotion processing
We have previously published a preliminary report comparing facial expression recognition in SAD patients with 30 healthy control participants. This showed a bias towards classifying more neutral faces as angry and fewer as sad (Bell et al., 2010). The current data confirms this result in the same patients, but in comparison with a larger group of healthy controls.
Performance on the Facial Expression Recognition Task did not differ among groups for accuracy of emotion identification or reaction time for responses. Although the overall low accuracy rate may suggest a possible floor effect on the task, separate analyses of low versus high levels of intensity showed that intensity of emotion did not affect performance differentially between groups and is therefore unlikely to have affected the sensitivity of the task. The results are in contrast to a recent study which showed a selective impairment in accuracy of recognition of disgust in inpatients with MDE (Douglas and Porter, 2010). That study used the same task, but it excluded low-intensity (0–50%) stimuli. It is likely that the difference in findings is explained mainly by the much greater severity of depression in that study. Other studies in which emotion specific or global identification accuracy deficits have been reported have also tended to involve more severely depressed patients (Mikhailova et al., 1996; Persad and Polivy 1993).
Gender effects on neuropsychological test performance
The lack of group by gender interactions in the present study is an important finding as it suggests there is no difference between males and females in the neuropsychological profile of depression. The finding is in contrast to a recent study of neuropsychological function in individuals with bipolar I disorder (Carrus et al., 2010) in which gender was found to modulate the degree of immediate memory (verbal and visual) dysfunction. The study by Carrus and colleagues was conducted in relatively euthymic patients, while in the current study, patients were depressed at the time of neuropsychological testing. It is possible that gender may be an important factor in more severe affective disorder but not in mild to moderate MDE (unipolar or bipolar II). These results suggest that there is no distinct neuropsychological phenotype in depression in women.
Conclusion
The current study found impaired verbal learning and memory, and impaired spatial working memory in outpatients with mild to moderate MDE, compared with patients with SAD and healthy controls. Notably, on the immediate recall trials of the CVC test, developed particularly for this study, there was an effect size difference of 0.61, which in our opinion, is clinically significant and likely to give rise to significant functional impairment and distress. The effects are not due to the use of ‘supernormal’ control subjects, since the difference also existed between MDE and SAD. There are preliminary studies investigating the use of specific cognitive training for the treatment of major depression (Elgamal et al., 2007; Siegle et al., 2007). The evidence of significant cognitive dysfunction even in mild to moderate MDE suggests that cognitive dysfunction may be an important and independent target for treatment by specific cognitive training techniques.
Footnotes
Acknowledgements
All authors were involved in the conception and design of the study and contributed to the collection of data. Cecilia Bourke and Richard J Porter analysed the data and wrote the first draft of the manuscript. All authors contributed to subsequent drafts and approved the final version.
We thank Katie Douglas for comments on an earlier draft of the manuscript
Funding
The study was funded by the Health Research Council of New Zealand and New Zealand Lotteries Grants Board.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.