
Abstract
Objective:
Those with mental illness are at increased risk of physical health problems. The current study aimed to examine the information available online to the Australian public about the increased risk and consequences of physical illness in those with mental health problems and the services available to address these co-morbidities.
Methods:
A structured online search was conducted with the search engine Google Australia (www.google.com.au) using generic search terms ‘mental health information Australia’, ‘mental illness information Australia’, ‘depression’, ‘anxiety’, and ‘psychosis’. The direct content of websites was examined for information on the physical co-morbidities of mental illness. All external links on high-profile websites [the first five websites retrieved under each search term (n = 25)] were examined for information pertaining to physical health.
Results:
Only 4.2% of websites informing the public about mental health contained direct content information about the increased risk of physical co-morbidities. The Australian Government’s Department of Health and Ageing site did not contain any information. Of the high-profile websites, 62% had external links to resources about physical health and 55% had recommendations or resources for physical health. Most recommendations were generic.
Conclusions:
Relative to the seriousness of this problem, there is a paucity of information available to the public about the increased physical health risks associated with mental illness. Improved public awareness is the starting point of addressing this health inequity.
Introduction
The promotion of physical health care in people with severe mental illness is a key issue. If we do not regard it as a priority we will not be able to state that a better quality of life [for] our patients is really what we strive for. (Maj, 2009)
Those who suffer from mental illness are at increased risk of co-morbid physical health problems (Leucht, 2007; Sim et al., 2006), which contribute to high rates of morbidity and mortality. Schizophrenia has been associated with higher rates of cardiovascular disease, obesity, diabetes, dental and optical problems (Leucht, 2007; Sim et al., 2006; Thornicroft, 2011), human immunodeficiency virus (HIV) infection and hepatitis (Rosenberg et al., 2001), osteoporosis (Hummer et al., 2005), sexual dysfunction (Smith et al., 2002), and obstetric complications (Jablensky et al., 2005). Similarly, depression has been strongly associated with cardiovascular disease (Andrei et al., 2007; Charlson, 2011; Grippo and Johnson, 2009) and is emerging as an independent risk factor for heart disease (Charlson, 2011; Dantzer et al., 2008).
The physical disease burden contributes to substantially reduced life expectancy for people with serious mental illness (Thornicroft, 2011), estimated to be approximately 20 years for those with schizophrenia compared to the general population. Reduced life expectancy is substantially accounted for by cardiovascular disease arising from the combination of lifestyle factors and the metabolic side effects of second-generation antipsychotic medication (Lawrence et al., 2010; Saha et al., 2007; Wahlbeck et al., 2011). This problem is further compounded by poor access to effective physical health care for this vulnerable group (Kisely, 2010; Lawn, 2012; Lawrence et al., 2010; Thornicroft, 2011; Wang, 2006).
There has been an increased public awareness of mental health problems through the provision of mental health literacy. This has enabled members of the public to access, understand, and use information about mental health conditions and treatment options in ways that promote mental health and well-being (Barney et al., 2006; Jorm et al., 2003; Lauber et al., 2003). In contrast to the excellent progress made in improving mental health literacy, physical health in the mentally ill has received relatively little attention (Killackey et al., 2011; Maguire et al., 2011).
Much of the dissemination of health information is now done online (Burns, 2010; Christensen and Hickie, 2010; Jorm et al., 2007). There has been a high take-up of Internet use in Australia; at the end of June 2011, there were 10.9 million Internet subscribers and 9.7 million mobile handset subscribers in Australia (Australian Bureau of Statistics, 2009, 2011) suggesting very widespread use in the Australian population. A substantial proportion of young Australians report that they use the Internet for information about mental health problems, either for themselves or for a friend (Burns, 2010; Jorm et al., 2007). Most use a search engine such as Google (93.3%) rather than deliberately accessing a specific website (6.7%) (Burns, 2010).
There is an obvious imperative to inform those who experience mental illness or care for someone with mental health problems of the associated increased physical health risks. This knowledge would assist in preventing physical illness by enabling monitoring and early interventions for physical morbidity. Furthermore, increasing public awareness of the alarming statistics associated with reduced life expectancy in those with serious mental illness brings pressure on governments to develop policy and provide resources addressing this health inequity. The current study aimed to examine what information was available online to the Australian public about the increased risk and consequences of physical illness in those with mental health problems and the services available to address these co-morbidities.
Methods
A search was conducted by one of the authors (M A) with the search engine Google Australia (www.google.com.au), using the generic search terms ‘mental health information Australia’, ‘mental illness information Australia’, ‘depression’, ‘anxiety’, and ‘psychosis’ on 7 December 2011. The search terms were chosen by author consensus as being non specific words that a member of the Australian public might use to search for information about mental illness. To mimic a search performed by a member of the public, the first 50 websites that appeared for each search term were considered to be a representative sample of the information available online, and the direct content (i.e. all content on the website excluding the external links) was examined for physical health information, issues, and resources. Websites were explored in the order of appearance. Scholarly (research) articles and sites for health professionals were not examined, as the focus was on information for the general public, rather than that available to the health or academic community. Sites that did not contain relevant content pertaining to mental health were also excluded. For example, sites about the ‘Economic Great Depression’ and the Internet Movie Database (IMDb) web pages for movies with titles including our search terms were excluded. Where there was uncertainty about the inclusion of a website, a second author (J S) was consulted and a consensus was reached. After exclusions, 142 websites were retained to examine for information relating to physical health issues in those with mental illnesses.
Additionally, for each of the five search terms, we examined all direct and indirect (i.e. external links) sections of the first five websites retrieved by Google for information about physical health (Figure 1). Information for consumers from these high profile websites pertaining to physical health was reported in standardised tabular form (Table 1). Three sites with direct content on physical health were also identified in the high profile websites. When the high-profile websites came up under more than one search term, we discarded the duplication and added the next site retrieved by Google.
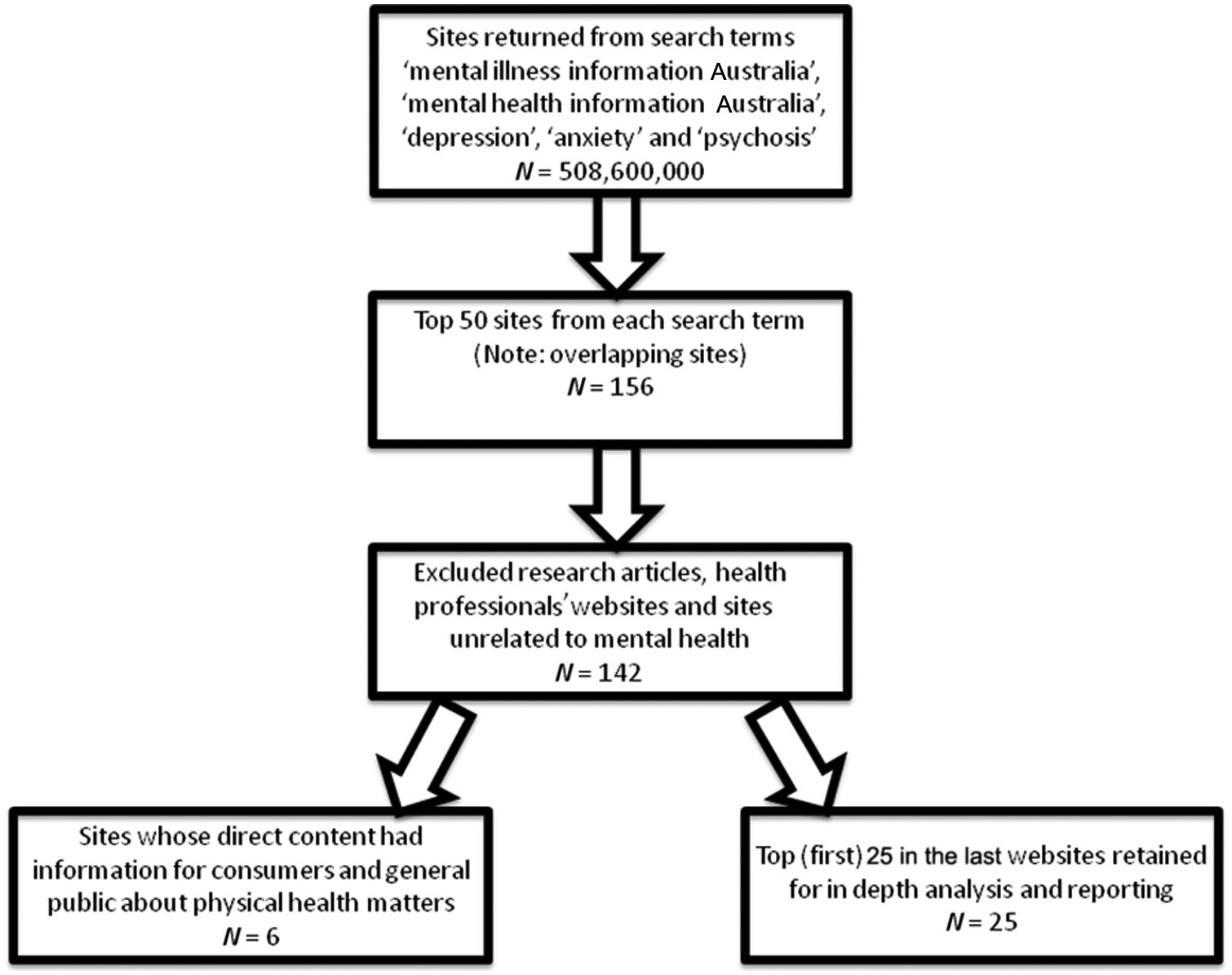
Search strategy used to explore mental health websites for physical health information and resources.
High profile a websites from Google search examined for direct and indirect content about physical health information and resources (N=29).
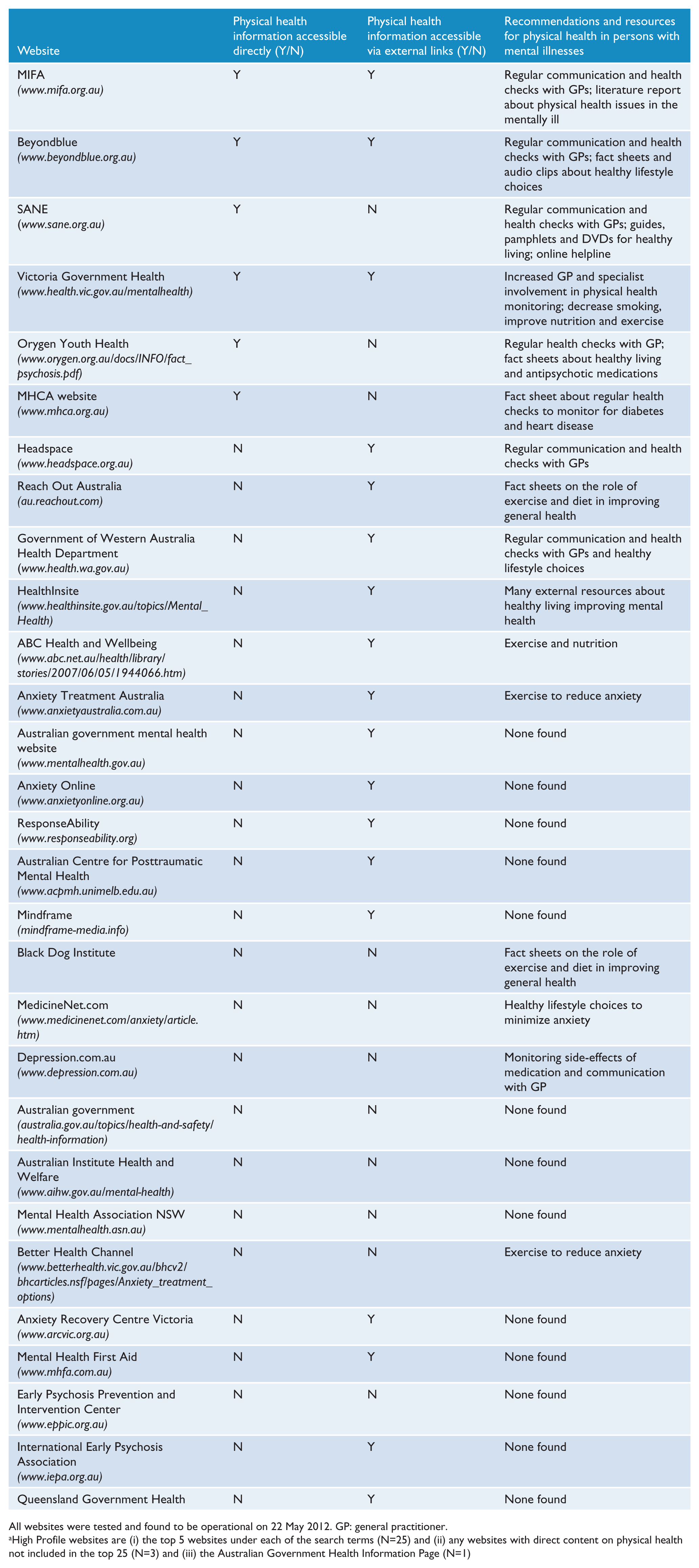
All websites were tested and found to be operational on 22 May 2012. GP: general practitioner.
High Profile websites are (i) the top 5 websites under each of the search terms (N=25) and (ii) any websites with direct content on physical health not included in the top 25 (N=3) and (iii) the Australian Government Health Information Page (N=1)
The Mental Health web page on the Australian Government’s Department of Health and Ageing website was also included as a high profile website for detailed examination on the 31 October 2011 as it was considered to be a valuable source of information about mental health resources. Items found under the ‘publications’ link were scanned for mental health resources, and information pertaining to physical health was sought within these resources. Furthermore, external links related to mental health were explored. The National Mental Health Reports, which primarily deal with the financial aspects of mental health services were excluded, as were any other legislative reports, implementation guidelines, and consultation and policy reports as these did not provide information about the health of those with a mental illness. Clinician guidelines and literary reviews were also excluded. Links to health professionals’ websites were not investigated. In total, the direct and indirect content of 29 high profile websites were examined and reported in detail (Table 1).
Results
Of the 142 websites investigated, only six (4.2%) [beyondblue, the Mental Health Council of Australia (MHCA), the Mental Illness Fellowship of Australia (MIFA), Orygen Youth Health (OYH), SANE, and the Victoria Mental Health Services] had direct content for the general public about physical health, and were further analysed to evaluate the information available. The Mental Health web page on the Australian Government’s Department of Health and Ageing website did not have information on the increased risk of co-morbid physical illness in the mentally ill.
Only two of the six websites outlined the issue of increased mortality and co-morbidity and reduced life expectancy in those with serious mental illnesses (MIFA and the Victoria Mental Health Services). The MIFA website was the most informative about the higher risk of developing physical illnesses in the mentally ill. It provided specific statistics on the increased incidence of physical illnesses in those with mental health disorders and also informed the public of increased mortality due to various conditions. Beyondblue explained the coexistence of depression with arthritis, coronary heart disease, dementia, and type 2 diabetes. The increased incidence of depression due to physical illness and the inverse relationship were both described, although there was an emphasis on the former.
The association between antipsychotic medication and weight gain, hypertension, hypercholesterolaemia, hyperglycaemia, diabetes, and heart disease was explained by the MHCA, MIFA, and OYH websites. Both beyondblue and SANE informed readers of the association between increased rates of smoking and depression, which in turn may result in poor physical health. Reduced physical activity was suggested as a cause for poor physical health by both MIFA and SANE.
With regard to the services available to meet the demands of co-morbid physical illness in the mentally ill, MIFA advocated the need for more resources to become available to address physical health issues. The Victoria Mental Health Service website recommended that the Victorian and Australian Governments should increase public awareness of the appropriate management of physical health issues in those with serious mental illnesses. Proposed means to minimise physical health issues included improving access to physical health checks, integrating mental and physical health care, increasing access to physical health information, establishing better communication between patients and general practitioners (GPs), and improving the socio-economic conditions of those with mental illnesses so as to enhance their physical health.
Increased communication by patients with their GPs was recommended by five sites (beyondblue, MHCA, MIFA, OYH, and SANE). Additionally, three sites (MHCA, OYH, and SANE) specifically promoted monitoring blood sugar and cholesterol levels, blood pressure, and weight, particularly in patients taking antipsychotic medications.
Of the high profile websites examined in detail for both direct and indirect content, 18 (62%) had external links to resources about physical health and 16 (55%) had recommendations or resources for physical health. Most websites were informative about different types of mental illness and the signs, symptoms, and management of each, but complicating physical health problems associated with mental illness were not described.
Eleven websites (ABC Health & Wellbeing, Anxiety Treatment Australia, beyondblue, Black Dog Institute, Government of Western Australia, HealthInsite, MedicineNet.com, OYH, Reach Out, SANE, and the Victoria Government websites) acknowledged the importance of diet, exercise, and other lifestyle choices on overall health, but did not specifically identify an increased necessity for those with mental illnesses to monitor their physical health due to the increased risk of health problems. Seven websites [beyondblue, Depression.com.au, Government of Western Australia, Headspace (National Youth Mental Health Foundation), MIFA, SANE, and Victoria Government websites] promoted regular communication and health checks with GPs, thus implying the association between mental and physical well-being.
The most common recommendation was healthy lifestyle choices to improve overall physical health followed by communication with GPs. The most common resource was downloadable fact sheets on improving physical health (Table 1).
Discussion
Similar to the increased health risks and reduced life expectancy of indigenous Australians, the high prevalence of physical morbidity among those with mental illness is a serious concern. The alarming statistic that the life expectancy in those with schizophrenia is reduced by approximately 20 years is now being recognised by health professionals (Charlson, 2011; Lawrence et al., 2010; Thornicroft, 2011). The contributors to this are a complex synergy of lifestyle factors, such as smoking, poor diet, and sedentary behaviours, neuroleptic therapy, complex physiological processes, e.g. depression and cardiac disease, higher rates of suicide and accidental death, and poorer access to physical health care than the rest of the population (Lawrence et al., 2010; Saha et al., 2007; Thornicroft, 2011; Wahlbeck et al., 2011). However, this major health inequity has yet to come to the attention of the Australian population.
The current paper examined the availability of physical health-related information contained within websites returned from online searches on mental illness. Only 4.2% of websites with high mental health visibility contained information specific to physical health risks. Furthermore, only two sites provided information on the risk of increased mortality and physical co-morbidities of serious mental illness (MIFA and the Victoria Mental Health Services websites). Although some sites provided generic health and well-being information about diet and exercise, on the majority of websites there was a paucity or absence of useful information available to increase public awareness of physical health problems in the mentally ill. This reflects the ongoing divide between physical and mental health and the failure of integrated health care for people with mental illness (Killackey et al., 2011; Maguire et al., 2011). The Commonwealth Government has made a substantial investment to improve the mental health of Australians. Congruent with this, it is imperative that they provide information to the public through their website on the physical health inequities of those with a mental illness.
The MIFA website extensively reviewed physical health risks in people with mental illness. We recommend that, at the time of this study, this site was the ‘gold standard’ and sites promoting mental health information should include similar detailed information on physical health risks. As well as current statistics on physical health risks in people with a mental illness (including mortality), specific information relating to the type of mental illness and associated physical health risks, information associated with the challenges of achieving good physical health, such as reduced access to care for physical illness and increased need for physical health monitoring due to medication side effects, and increased risk of substance use and social isolation should be included as a minimum standard on mental health websites.
The Internet is ubiquitous in modern life and is a major source of health information for the general public (Burns, 2010). Several well-known Australian organisations working in the mental illness sector have a substantial online presence, and even engage in web-based mental health interventions. Studies have demonstrated the efficacy of these online therapies (Christensen and Hickie, 2010). Yet, the physical health risks associated with mental illness, and physical health information and interventions for mental health problems appears to have been ignored by this sector. A potential risk is that the provision of this information may cause alarm and further distress. However, without the dissemination of information, the poor physical health of people with mental illness will persist.
This study has several limitations. The search was undertaken by only one of the authors. This strategy increases the risk of bias in the selection of websites. The methodology could have been further improved by the use of two investigators searching independently with data collection sheets designed a priori and assessment of inter-rater reliability. Furthermore, this study relies on a single web search engine using a proprietary search strategy. It is also done at a moment in time, and the rapid online changes will outdate searches as soon as they are complete. However, these limitations may also be strengths of the study, as it represents a naturalistic search for information. Finally, the method assumed no interest in scholarly works, which may well have revealed the information sought to the interested member of the general public. Despite these limitations, the study provides a snapshot of what is likely to be encountered during an online search on mental illness and reveals a distinct lack of information on the substantial physical health morbidity associated with mental illness.
Government and non-government bodies need to address physical health problems in those with mental ill health. An obvious starting point is informing the public about these risks. Furthermore, widely available and specific information on how to abate these risks must be made available to consumers and the general public. Given the widespread use of the Internet to disseminate public health information, it is recommended that clear and unambiguous information be available on websites informing the public about mental illness. It has previously been reported that Australian mental health consumers attend GPs more often than the rest of the population (Mai et al., 2010). Therefore, in Australia, it is not an issue of access but rather one of effective use of consultations. Websites must provide information to empower consumers in making the best use of their consultations with their GPs so as to reduce their risk of physical morbidity and mortality.
Future research should investigate the use of the Internet for the provision of information on physical health to this high-risk population. In particular, it is important to better understand the form and content of information that consumers with mental illness and their families would value. It is also essential to determine if the use of fact sheets, which are currently available on some websites, actually results in changes in health behaviours. Research should examine the most effective ways that the Internet can be used to improve physical health in the mentally ill.
The findings of this study suggest an urgent need to address the paucity of information available on co-morbid physical health problems in the mentally ill. This information needs to be provided to those who are very early in the course of mental ill health so that appropriate health monitoring and necessary interventions can be instigated. Increasing public awareness of this serious health inequity would catalyse governments to address this problem with the urgency it deserves.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.