
Abstract
Objectives:
This study aims to examine the characteristics of obsessive compulsive disorder (OCD) associated with high levels of schizotypy.
Methods:
Using the Schizotypal Personality Questionnaire (SPQ) with 177 individuals with OCD, patients with OCD and high levels of schizotypy (OCD-HS) were compared to patients with OCD and low levels of schizotypy (OCD-LS) on a range of clinical characteristics. Self-report and clinician-administered instruments were used. Results were adjusted for the severity of OCD symptoms, age, marital status and comorbidity using logistic regression.
Results:
Patients with OCD-HS were younger and less likely to have been married. OCD-HS was associated with higher rates of symmetry/order obsessions, ordering/arranging compulsions, checking compulsions, co-occurring major depression, post-traumatic stress disorder, substance use disorders and greater general psychopathology. Previously reported associations, such as higher total scores on the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) were not significant when adjusted for differences in demographic variables and comorbidity.
Conclusions:
Patients with OCD-HS were associated with specific OCD symptoms and comorbid conditions and may warrant a specific treatment approach.
Introduction
Obsessive compulsive disorder (OCD) is defined by recurrent and intrusive thoughts, images or urges (obsessions) and repetitive behaviours or mental acts (compulsions). The disorder can be chronic and disabling, with clinicians facing a diagnostic dilemma as to whether patients have OCD or schizophrenia when there are extensive cognitive deficits (Whitney et al., 2004), functional decline (Murray and Lopez, 1994) or delusional beliefs (Brakoulias and Starcevic, 2011; Oulis et al., 2013). The relationship between OCD and schizophrenia has intrigued researchers and clinicians over many decades (Berrios, 1989) and researchers have proposed a schizo-obsessive disorder (Attademo et al., 2012; Gross-Isseroff et al., 2003). In addition, schizotypy and schizotypal personality disorder constructs related to schizophrenia (Vollema et al., 2002) have been linked to OCD. Patients with OCD and high levels of schizotypy tend to be challenging to treat (Baer et al., 1992; Ravizza et al., 1995) and hence it is important to understand their clinical characteristics.
The term ‘schizotypy’ was first used by Kraepelin to refer to the relatives of patients with schizophrenia who were odd, but did not meet the criteria for schizophrenia (Meehl, 1962; Rado, 1953). These patients often exhibit ideas of reference, excessive social anxiety, odd beliefs and magical thinking, unusual perceptual experiences, odd or eccentric behaviour, absence of close friends, odd speech, constricted affect and suspiciousness (Raine, 1991). When patients have a pervasive pattern of social and interpersonal deficits marked by acute discomfort with, and reduced capacity for, close relationships as well as by cognitive or perceptual distortions and eccentricities of behaviour, beginning in early adulthood and present in a variety of contexts, they are said to have schizotypal personality disorder. Schizotypal personality disorder is more common as a secondary diagnosis in OCD than in other disorders (Poyurovsky and Koran, 2005), with frequencies ranging from 5% (Baer et al., 1990) to 33% (Jenike et al., 1986). The Schizotypal Personality Questionnaire (SPQ) (Raine, 1991) is the most widely used dimensional measure of schizotypy, whereas structured clinical interviews have been used to diagnose schizotypal personality disorder.
Patients with obsessive compulsive disorder (OCD) and high levels of schizotypy (OCD-HS) have been found to have more severe OCD symptoms (Huang et al., 2011; Tallis and Shaffran, 1997), a poorer prognosis (Huang et al., 2011) and an earlier age of onset of their disorder (Sobin et al., 2000). Neuroimaging has revealed reductions in grey matter volume (Jin Lee et al., 2006), and neuropsychological studies (Harris and Dinn, 2003; Shin et al., 2008) have reported dorsolateral and frontal lobe dysfunction in OCD-HS compared to those with a low level of schizotypy (OCD-LS). Co-occurring schizotypal personality disorder has predicted more severe OCD symptoms (Baer et al., 1992), more marked functional decline (Poyurovsky et al., 2008), poorer treatment outcome (Baer et al., 1992; Ravizza et al., 1995), increased prescription of antipsychotic medication (Poyurovsky et al., 2008), good response to low-dose antipsychotic agents when added to SSRIs (Bogetto et al., 2000) and an increased rate of relatives with schizophrenia (Poyurovsky et al., 2008). With several studies indicating that OCD-HS is associated with characteristics that distinguish it from OCD-LS, it has been proposed that OCD-HS may represent a valid subtype of OCD (Poyurovsky and Koran, 2005; Siever and Gunderson, 1983). However, the existing literature is limited in that the findings of reported studies did not control for severity of OCD. As OCD-HS is associated with more severe OCD, it cannot be determined whether the reported characteristics associated with OCD-HS were specific to OCD-HS or related to OCD severity.
The relationship between OCD-HS and specific OCD symptoms is somewhat unclear. Some studies (Tallis and Shaffran, 1997; Yamamoto et al., 2012) have associated OCD-HS with more prominent obsessions as measured by the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) (Goodman et al., 1989), in contrast to findings of one other study (Poyurovsky et al., 2008). OCD-HS has also been associated with specific OCD symptoms such as checking (Aardema and Wu, 2011; Chmielewski and Watson, 2008), ordering (Chmielewski and Watson, 2008; Sobin et al., 2000) and hoarding (Aardema and Wu, 2011; Chmielewski and Watson, 2008). One study found no association between OCD-HS and specific OCD symptoms (Huang et al., 2011).
The relationship between OCD-HS and co-occurring diagnoses also requires further evaluation. Only two studies (Poyurovsky et al., 2008; Sobin et al., 2000) have systematically assessed for associations between schizotypy in OCD and comorbid diagnoses. Sobin et al. (2000) found that OCD-HS was associated with higher rates of comorbid substance use disorders, panic disorder and specific phobia. Poyurovsky et al. (2008) found that the co-occurrence of schizotypal personality disorder did not predict any other comorbid diagnoses.
This study aims to add to existing literature by systematically evaluating the clinical characteristics associated with OCD-HS in a sample of patients with OCD and to determine whether previously reported findings remain significant when OCD severity has been accounted for. In accordance with previous studies (Huang et al., 2011; Sobin et al., 2000; Tallis and Shaffran, 1997), it was hypothesised that OCD-HS would be associated with OCD severity and co-occurring substance abuse. If confirmed, these hypotheses may have important implications for understanding and treating patients with OCD-HS.
Methods
Recruitment and criteria for inclusion
This report has resulted from the Nepean OCD Study, conducted in Sydney and several other Australian cities. Participants (N = 177) were recruited from the Nepean Anxiety Disorders Clinic, OCD support groups, newspaper advertisements and referrals from general practitioners, psychiatrists, clinical psychologists and mental health services. Participants were included if they had a primary diagnosis of OCD which was determined on the basis of a clinician-administered semi-structured interview, the MINI International Neuropsychiatric Interview plus version (Sheehan and Lecrubier, 2010), and the qualifier that OCD was the condition for which they sought help or which caused the most distress or impairment in functioning. Individuals with current comorbid diagnoses of psychosis, bipolar affective disorder, a pervasive developmental disorder, severe intellectual disability, or substance abuse or dependence were excluded on the basis that participants with these diagnoses would be unable to objectively and comprehensively answer the many questions required as part of the study. Participants needed to be over the age of 18. Institutional ethics committee approval was obtained prior to commencing the study and all participants provided signed informed consent.
Measures
Several clinician-administered and self-report instruments were used. The former included the MINI International Neuropsychiatric Interview (MINI) (Sheehan and Lecrubier, 2010), the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) (Goodman et al., 1989), the Clinical Global Impression Scale (CGI) (Guy, 1976), the Sheehan Disability Scale (SDS) (Sheehan, 1983), the Overvalued Ideas Scale (OVIS) (Neziroglu et al., 1999), and the Family History Screen (Weissman et al., 2000). The following self-report measures were administered: the Vancouver Obsessive Compulsive Inventory (VOCI) (Thordarson et al., 2004), the Symptom Checklist 90-Revised (SCL-90R) (Derogatis, 1994) and the Obsessive Beliefs Questionnaire (OBQ) (Obsessive Compulsive Cognitions Working Group, 2005; Steketee et al., 2003).
Schizotypy was assessed using the 74-item SPQ, which has excellent internal consistency (0.91), and good test–retest reliability (0.82) and discriminant validity (Raine, 1991). Participants were deemed to have had high schizotypy if their score on the SPQ was greater than 41. A cut-off score of 41 captured the top 10% of scores in Raine’s original 1991 study (Raine, 1991) where 55% of those scoring greater than 41 met DSM-III-R criteria for schizotypal personality disorder. A similar cut-off of 40 was also supported by a French validation of the SPQ (Dumas et al., 2000). Dichotomizing scores on the SPQ by way of imposing a cut-off for high levels of schizotypy is consistent with various taxometric analyses (Haslam et al., 2012) that have suggested that the construct of schizotypy has characteristics of a taxon rather than dimension.
The MINI (plus version) is a clinician-administered semi-structured interview that was used to determine co-occurring DSM-IV diagnoses and their age of onset, in addition to ascertaining whether the DSM-IV criteria for OCD have been met. The MINI has been validated against other widely used structured diagnostic interviews and its psychometric properties have been good (Lecrubier et al., 1997).
The severity of OCD was assessed by means of the Y-BOCS total score and the CGI, whereas OCD symptoms were assessed via the Y-BOCS Symptom Checklist (YBOCS-SC). The YBOCS-SC is a semi-structured interview which includes a comprehensive list of 64 obsessions and compulsions arranged by content into 15 categories. The categories for obsessions are: aggressive; contamination; sexual; hoarding/saving; religious; symmetry/exactness; miscellaneous; and somatic. The categories for compulsions are: cleaning/washing; checking; repeating; counting; ordering/arranging; hoarding/collecting; and miscellaneous. Two items from the aggressive obsessions category were reclassified as ‘obsessions about unintentional harm’. These were: ‘fear will harm others because not careful enough’ and ‘fear will be responsible for something else terrible happening’. All other items pertaining to aggressive obsessions were categorised as ‘impulsive aggression’ obsessions. This method has been used in other studies (Pinto et al., 2008) in an attempt to reduce the heterogeneity within the aggressive obsessions category.
Interviews were conducted by a psychiatrist or clinical psychologist trained in the use of the MINI and YBOCS-SC. Inter-rater reliability was assessed for the first 49 participants (this involved two raters independently completing the MINI and the YBOCS-SC in the same assessment), and for the YBOCS-SC categories this was excellent (94.3% agreement).
Insight and other characteristics of belief related to OCD were measured using the OVIS. This structured clinical interview has been shown to have better predictive validity than the single item that assesses insight on the Y-BOCS and its internal consistency is 0.88 (Neziroglu et al., 2001).
Disability was measured using the SDS (Sheehan, 1983). This scale assesses levels of disability in three domains: work, social life, and family life/home responsibilities using a 10-point scale. It has good psychometric properties when used for assessing disability associated with anxiety disorders (Hambrick et al., 2004).
The Family History Screen (Weissman et al., 2000) is a validated tool designed to screen for the presence of a positive family history for a range of common psychiatric disorders (e.g. major depressive disorder, panic disorder, obsessive compulsive disorder, psychosis) by asking participants whether they had ever detected symptoms of these disorders in their first-degree relatives.
The VOCI (Thordarson et al., 2004) is a 55-item self-report measure of OCD symptoms. This instrument uses a five-point Likert-type scale, with ratings being summed to provide scores on six separate subscales (contamination, checking, obsessions, hoarding, just-right experiences and indecisiveness). The internal consistency (0.94), test–retest reliability and convergent and discriminant validity of the VOCI have been reported to be favourable (Thordarson et al., 2004).
Symptom distress and psychopathology were measured by the SCL-90R. This 90-item psychometrically sound instrument (internal consistency = 0.93) (Peveler and Fairburn, 1990), provides scores on the Global Severity Index and nine subscales: Somatization, Obsessive-compulsive, Interpersonal sensitivity, Depression, Anxiety, Hostility, Phobic anxiety, Paranoid ideation and Psychoticism.
Cognitive styles along the dimensions of responsibility/threat estimation, perfectionism/intolerance of uncertainty and importance/control of thoughts were assessed with the 44-item OBQ. The psychometric properties of the OBQ in samples with OCD, where it has been used in a large number of studies, have been reported to be good (internal consistency = 0.95) (Wu and Carter, 2008).
Statistical methods
All data were entered into the Statistical Package for the Social Sciences (SPSS) version 17 (2003) and analysed. Additional analyses were conducted using SAS version 9.3 (SAS Institute). The characteristics of participants with OCD whose SPQ scores were greater than 41 (‘high schizotypy’, OCD-HS) were compared with those participants whose SPQ scores were 41 or less (‘low schizotypy’, OCD-LS). The internal consistency of the SPQ, Y-BOCS, OVIS, SDS, VOCI, OBQ and SCL-90R was calculated. Logistic regression analysis was used to compare schizotypy groups across categorical variables and t-tests were used to compare across normally distributed continuous variables. A Kruskal–Wallis test was used for non-normally distributed data. Additionally, where appropriate, multivariate analyses were performed using logistic regression (for categorical data) and linear regression (for continuous data) to compare groups, adjusting for statistically significant clinical and patient characteristics. These are detailed in the tables.
Results
Of the 177 study participants with OCD, 41 (23.2%) had high levels of schizotypy. Using the results reported by Raine (1991), where 55% of participants with high levels of schizotypy met criteria for a DSM-III-R diagnosis of schizotypal personality disorder, perhaps more than 12% of participants in the present study would meet criteria for DSM-III-R schizotypal personality disorder. Participants with OCD-HS tended to be younger, were less likely to have been married, more likely to have had a comorbid diagnosis of major depressive disorder, post-traumatic stress disorder (PTSD), alcohol abuse, alcohol dependence and drug abuse (Table 1). Participants with OCD-HS had higher scores on all belief domains assessed by the OBQ (Table 1).
Demographic and clinical characteristics of OCD patients with and without high levels of schizotypy.
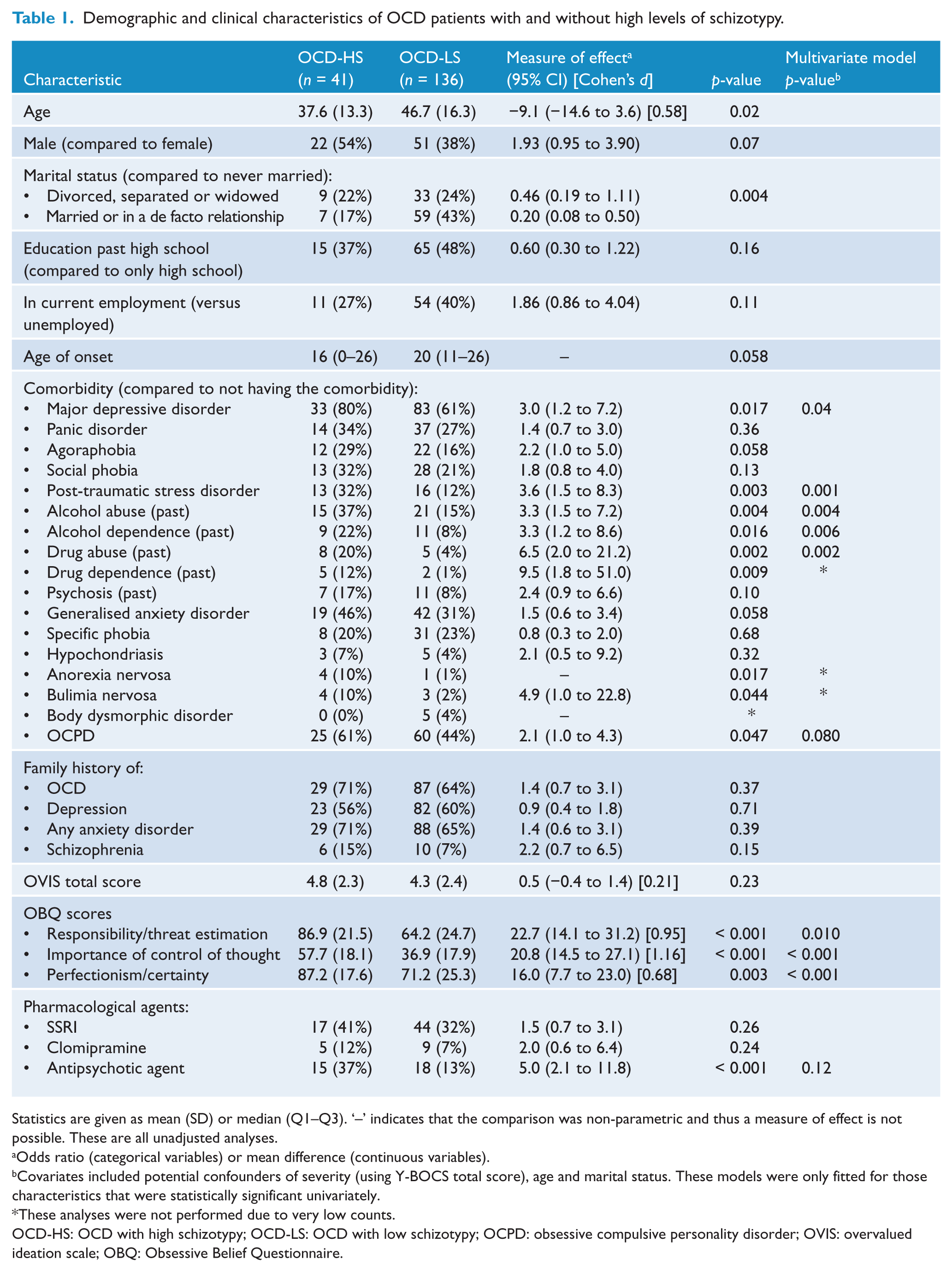
Statistics are given as mean (SD) or median (Q1–Q3). ‘–’ indicates that the comparison was non-parametric and thus a measure of effect is not possible. These are all unadjusted analyses.
Odds ratio (categorical variables) or mean difference (continuous variables).
Covariates included potential confounders of severity (using Y-BOCS total score), age and marital status. These models were only fitted for those characteristics that were statistically significant univariately.
These analyses were not performed due to very low counts.
OCD-HS: OCD with high schizotypy; OCD-LS: OCD with low schizotypy; OCPD: obsessive compulsive personality disorder; OVIS: overvalued ideation scale; OBQ: Obsessive Belief Questionnaire.
OCD-HS was associated with two markers of severity (CGI and VOCI total sore), but the association with higher Y-BOCS scores did not remain significant when adjustments were made for age, marital status and comorbidity (Table 2). After adjusting for severity, age, marital status and comorbidity, a lower level of function was no longer associated with the OCD-HS group.
Levels of severity and disability in OCD patients with and without high levels of schizotypy.
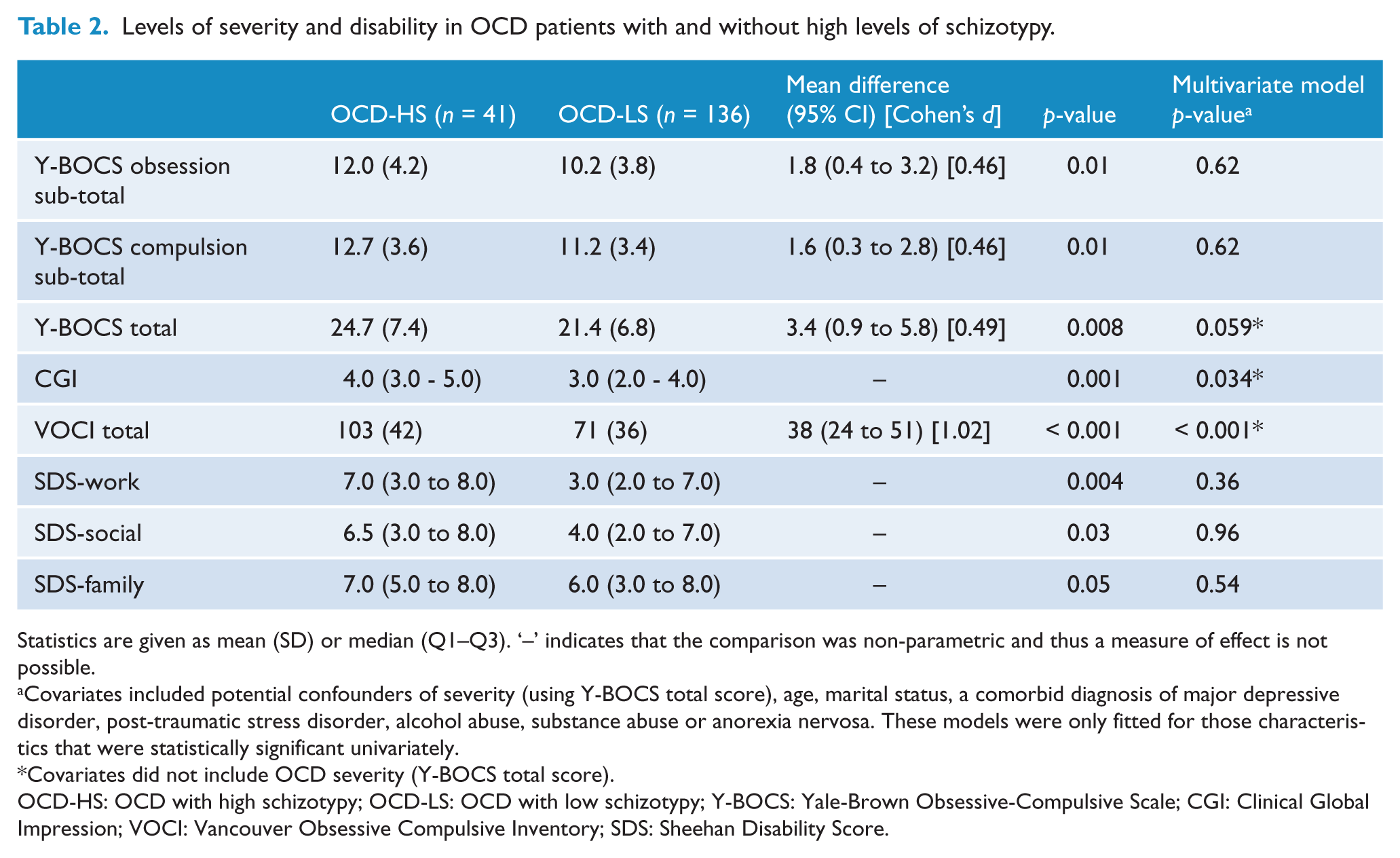
Statistics are given as mean (SD) or median (Q1–Q3). ‘–’ indicates that the comparison was non-parametric and thus a measure of effect is not possible.
Covariates included potential confounders of severity (using Y-BOCS total score), age, marital status, a comorbid diagnosis of major depressive disorder, post-traumatic stress disorder, alcohol abuse, substance abuse or anorexia nervosa. These models were only fitted for those characteristics that were statistically significant univariately.
Covariates did not include OCD severity (Y-BOCS total score).
OCD-HS: OCD with high schizotypy; OCD-LS: OCD with low schizotypy; Y-BOCS: Yale-Brown Obsessive-Compulsive Scale; CGI: Clinical Global Impression; VOCI: Vancouver Obsessive Compulsive Inventory; SDS: Sheehan Disability Score.
High levels of schizotypy were associated with all VOCI symptom subscale scores except for contamination, whereas significant associations with the Y-BOCS-derived OCD symptoms were only present for symmetry/order obsessions, checking and ordering/arranging compulsions (see Table 3). Table 4 illustrates the significantly increased rates of general psychopathology as measured by the SCL-90R in the OCD-HS group.
OCD symptoms in OCD patients with and without high levels of schizotypy.
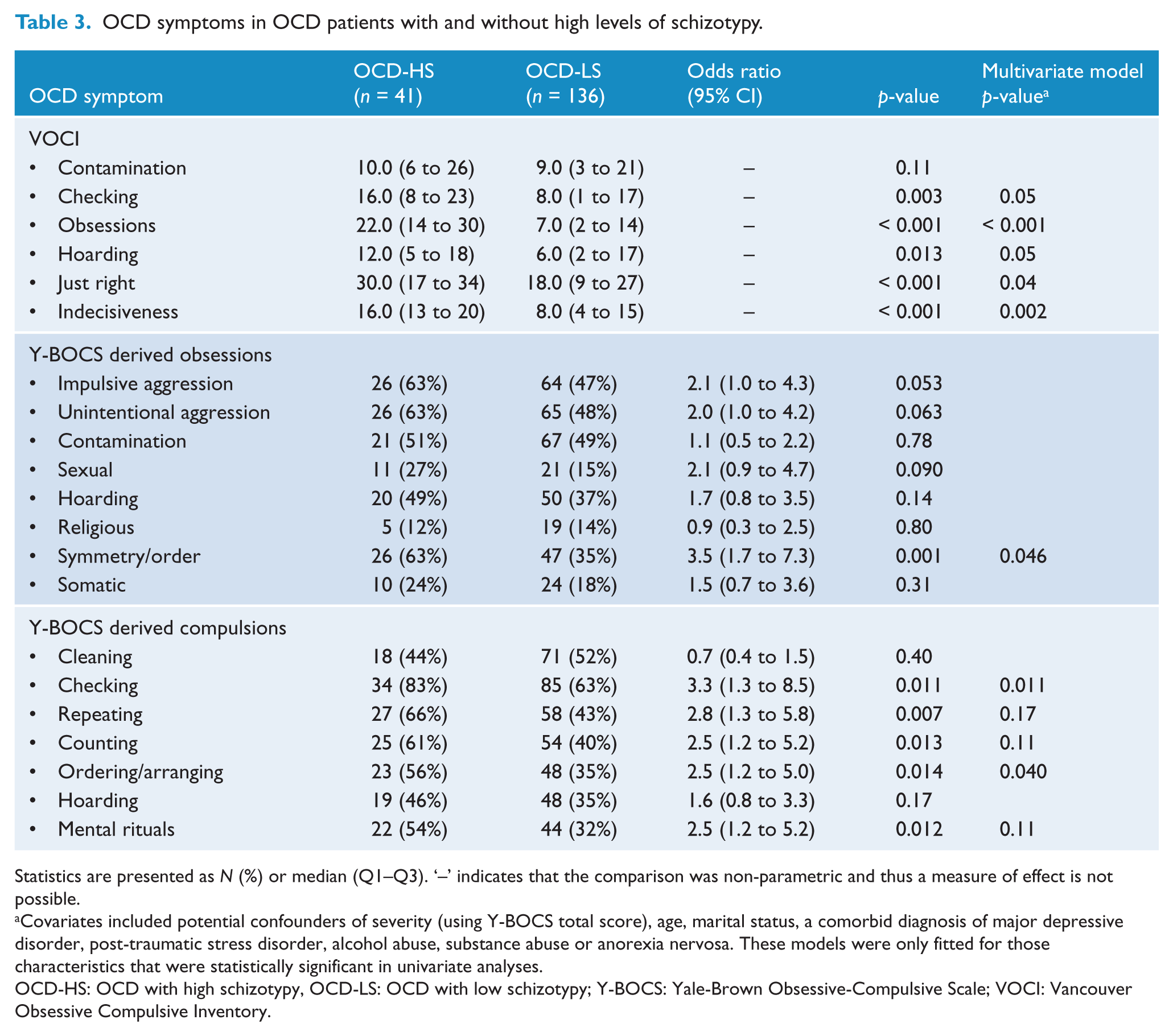
Statistics are presented as N (%) or median (Q1–Q3). ‘–’ indicates that the comparison was non-parametric and thus a measure of effect is not possible.
Covariates included potential confounders of severity (using Y-BOCS total score), age, marital status, a comorbid diagnosis of major depressive disorder, post-traumatic stress disorder, alcohol abuse, substance abuse or anorexia nervosa. These models were only fitted for those characteristics that were statistically significant in univariate analyses.
OCD-HS: OCD with high schizotypy, OCD-LS: OCD with low schizotypy; Y-BOCS: Yale-Brown Obsessive-Compulsive Scale; VOCI: Vancouver Obsessive Compulsive Inventory.
A comparison of mean SCL-90R sub-scores and global severity indices for OCD-HS compared to OCD-NHS.
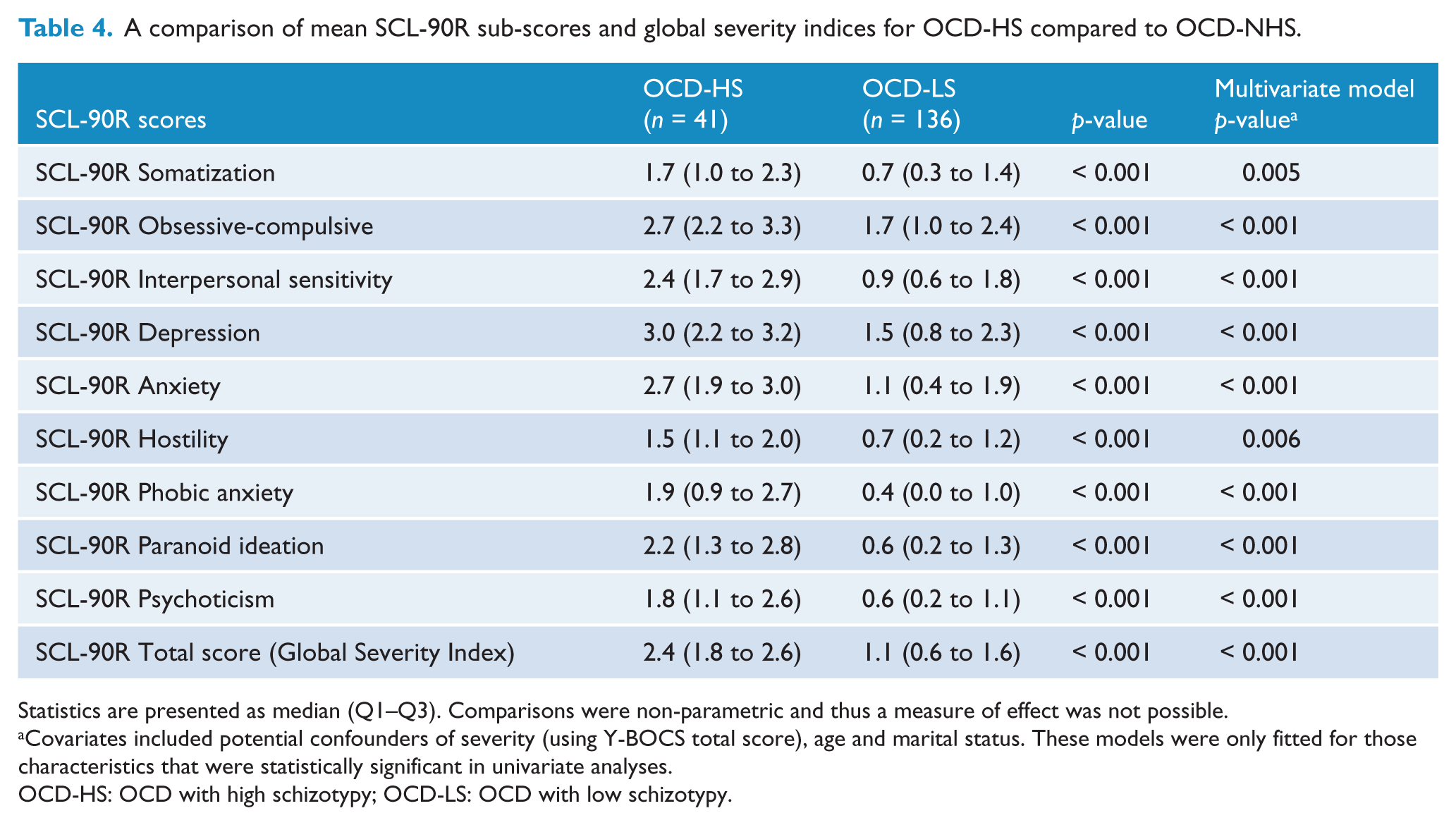
Statistics are presented as median (Q1–Q3). Comparisons were non-parametric and thus a measure of effect was not possible.
Covariates included potential confounders of severity (using Y-BOCS total score), age and marital status. These models were only fitted for those characteristics that were statistically significant in univariate analyses.
OCD-HS: OCD with high schizotypy; OCD-LS: OCD with low schizotypy.
The internal consistencies of the measures used in this sample were favourable (SPQ (0.95), Y-BOCS (0.89), OVIS (0.85), SDS (0.85), VOCI (0.95), OBQ (0.96) and SCL-90R (0.98)).
Discussion
The results of this study cast doubt on our hypothesis and on previous findings that OCD-HS is associated with increased OCD severity. Y-BOCS total scores were no longer significantly higher in patients with OCD-HS than in those with OCD-LS when age, marital status and comorbidity were controlled for. The significantly higher scores on all domains of the SCL-90R and significantly higher CGI scores in patients with OCD-HS indicate a more severe general psychopathology. However, this does not appear to be related to OCD, but rather to the characteristics associated with schizotypy. This is supported by studies reporting less severe OCD symptoms in patients with OCD and schizophrenia in comparison to OCD alone (Doyle et al., 2014). Hence it is unlikely that OCD occurs on a spectrum of severity towards schizophrenia, and the more severe OCD would not necessarily indicate a greater likelihood of the occurrence of schizophrenia.
Consistent with findings in the literature thus far (Chmielewski and Watson, 2008; Tallis and Shaffran, 1997; Yamamoto et al., 2012), there were conflicting findings between results derived from self-report and clinician-administered instruments in relation to the association between high levels of schizotypy and specific OCD symptoms. The self-report instrument (the VOCI) revealed associations with more OCD symptoms than did the clinician-administered instrument (the Y-BOCS), possibly because self-report measures tend to overestimate symptoms (Rush et al., 2006).
The strong association (as indicated by odds ratios in the range of 2.5 to 3.5) between OCD-HS and symmetry/order obsessions, symmetry arranging compulsions and checking compulsions adds to the findings of previous studies (Aardema and Wu, 2011; Chmielewski and Watson, 2008; Sobin et al., 2000). The association with symmetry/arranging symptoms may be explained by magical thinking that often accompanies both these OCD symptoms and schizotypy. ‘Just-right feelings’ that are often associated with symmetry/arranging symptoms may be more likely to appear in a personality with schizotypal characteristics. Studies have also reported associations between checking compulsions and social anxiety that accompanies schizotypy (Roth and Baribeau, 2000; Sher et al., 1991). Magical thinking, ‘just-right feelings’ and social anxiety may be important targets for future research aiming to improve cognitive-behavioural approaches to treating symmetry/arranging compulsions and checking compulsions in patients with prominent schizotypy.
This study revealed significant associations between OCD-HS and specific co-occurring psychiatric disorders, even when adjustments were made for severity, age and marital status. Although higher rates of co-occurring substance abuse have been previously reported in patients with OCD-HS (Sobin et al., 2000), this study revealed a particularly strong relationship between OCD-HS and past substance abuse (OR = 6.5). Hence, it is important to screen these patients for substance abuse. Schizotypy is thought to precede substance abuse (Schiffman et al., 2005), with the latter possibly related to the social anxiety (Sher et al., 1991) or the deficits in frontal lobe function (Mass et al., 2001) associated with schizotypy.
The association between OCD-HS and the diagnosis of a major depressive disorder is contrary to the findings of previous studies (Poyurovsky et al., 2008; Sobin et al., 2000), but depression may be precipitated by a higher rate of interpersonal stressors to which patients with high levels of schizotypy might be predisposed due to their poor social skills. This same vulnerability may also explain the increased co-occurrence of PTSD in individuals with OCD-HS. Although this finding has not been previously reported, it is worthy of further investigation as patients with schizotypy lack social judgement (Morrison et al., 2013) and may therefore unknowingly find themselves in dangerous situations or inadvertently provoke others to the extent that they become physically threatened. Steel et al. (2008) also suggest that schizotypy may be a vulnerability factor that predisposes individuals to the development of PTSD.
Patients with OCD-HS were found to be younger and less likely to be married, which is in agreement with results reported by Huang et al. (2011). Within the limitations of their retrospective file audit, they speculated that patients with high levels of schizotypy were younger and single as they tended to develop schizophrenia as they grew older. An alternative explanation is that schizotypy becomes less prominent over time. Hence prospective studies are required to more accurately determine the prognosis of patients with OCD-HS.
OCD-HS was not associated with more antipsychotic use, or with higher OVIS scores. The higher scores on all cognitive domains of the OBQ suggest that patients with OCD-HS had stronger cognitions relating to responsibility/threat, perfectionism/uncertainty and importance of control of thoughts. Higher ratings on these cognitive domains may reflect schizotypal patients’ strong and unusual beliefs (though not necessarily delusional beliefs), as well as their social isolation, which would lead to fewer opportunities for reality checks with other people. This suggests the importance of tackling beliefs in the course of cognitive-behavioural therapy in patients with OCD-HS.
The limitations of this study pertain first to its cross-sectional design. Although the study advances previous research by the use of clinician-administered instruments, use of self-report measures may have led to over-reporting of some symptoms and psychopathology, and these measures may have items that overlap across several domains of assessment. It appears that study participants are fairly representative of individuals with OCD in Australia and elsewhere, however we cannot entirely exclude the possibility of certain referral bias. Also, our comprehensive assessment might have deterred some individuals who would have otherwise been willing to participate. Another limitation was exclusion of OCD participants with schizophrenia and bipolar disorder, as inclusion of such participants might have added more depth to the findings, particularly with regards to the relationship between OCD-HS and OCD with schizophrenia. However, the comprehensive nature of our assessment with reliance on a number of self-report instruments mandated a decision to exclude individuals with severe mental illness. Future studies should also investigate non-clinical samples with high and low levels of schizotypy to determine whether there are any specific characteristics associated with OCD-HS.
In conclusion, this study represents a major contribution to the literature in that it has demonstrated that patients with OCD-HS have distinct clinical characteristics that are unrelated to OCD symptom severity. In addition, it is the first study to use a comprehensive methodology that involved controlling for several key demographic and clinical variables. While treating patients with OCD-HS, cognitive-behavioural therapy should be tailored to address the magical thinking, unusual beliefs, ‘just-right feelings’ and social anxiety that often accompany schizotypy. Behavioural approaches to address interpersonal difficulties may help to increase opportunities for reality testing and reduce social ineptness. This study also suggests that patients with OCD-HS should be assessed for the presence of any co-occurring substance abuse, depression and PTSD; if present, these disorders should receive full therapeutic attention alongside OCD.
Footnotes
Acknowledgements
The authors are grateful to Colin Slocombe from ACEDA Adelaide, Michelle Graeber from ARCVIC Melbourne, Scott Blair-West of the Melbourne Clinic, the Blacktown and Kogarah OCD Support Groups, the Mental Health Association of NSW, the Penrith Mental Health Practitioners’ Network and to statistician Dr Andrew Martin.
Funding
This research was funded by the Nepean Medical Research Foundation, a competitive Pfizer Neuroscience Grant and the Discipline of Psychiatry at The University of Sydney.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper. Underlying research materials related to this paper are available on request by contacting the corresponding author.