
Abstract
Objective:
Symptoms of depression are highly prevalent and persistent following myocardial infarction (MI). Whether depression is a risk factor for long-term mortality following MI remains controversial. The present study aimed to determine whether depression during hospitalisation for acute MI (AMI) predicted 5-year all-cause or cardiac mortality.
Method:
This study utilised the Identifying Depression as a Comorbid Condition (IDACC) database of 337 hospitalised patients with AMI. Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression scale (CES-D). Data were linked to a government administrative death registry to determine 5-year mortality. Survival data were analysed using Cox’s proportional hazards model.
Results:
The mean age during AMI hospitalisation was 59 years ± 12, 74% of patients were men and depression (CES-D ≥ 16) was present in 132 patients (39.3%). The 5-year all-cause mortality rate was 10.4% (35 deaths) and the cardiac mortality rate was 6.5% (22 deaths). When depression was defined as a dichotomous variable, moderate to severe depression (defined by CES-D ≥ 27) at the time of AMI was associated with all-cause mortality (hazard ratio 2.54, 95% confidence interval 1.03 to 6.28; p = 0.04) but not cardiac mortality. However, when depression was defined by three categories (no depression CES-D < 16, mild depression CES-D 16–26, moderate to severe depression CES-D ≥ 27), it was not found to predict mortality. In addition, perceived social support was a predictor of all-cause and cardiac mortality in AMI patients.
Conclusions:
Our results indicate that the relationship between mortality and depression severity is not linear and that the association only becomes evident when the severity reaches a threshold level of CES-D ≥ 27, consistent with major depression. Low power may have influenced the finding of a lack of association between depression and cardiac mortality.
Introduction
According to the World Health Organization, by 2020 depression will be the second leading cause of disability-adjusted life years lost – with ischaemic heart disease being the first (Murray and Lopez, 1996). Previous research has established that one in five patients experience depressive symptoms after myocardial infarction (MI) (Frasure-Smith et al., 1993) and that these symptoms are a risk factor for short-term mortality (Frasure-Smith et al., 1995). However, whether depression is a risk factor for mortality ≥ 5 years post-MI remains controversial, with some studies reporting that depression predicts mortality in MI patients (Carney et al., 2008; Lesperance et al., 2002; Pfiffner and Hoffman, 2004; Welin et al., 2000) while more recent reports have failed to detect an association (Dickens et al., 2007; Parakh et al., 2008). The present study was conducted to determine whether depression was associated with mortality 5 years after initial hospitalisation for acute MI (AMI) in a local Australian cardiac population. Analyses were undertaken on a well-characterised cohort of patients hospitalised for a range of cardiac conditions from the Identifying Depression as a Comorbid Condition (IDACC) (Schrader et al., 2005) database in terms of demographic, socioeconomic, psychological and cardiac factors. Predictors of all-cause and cardiac mortality were examined in a subset of patients hospitalised for AMI.
Method
Design
Details of the design of the IDACC study have been previously reported (Cheok et al., 2003) but, in brief, patients admitted to South Australian hospitals with a range of cardiac diagnoses were recruited between 2000 and 2002. Patients were screened for depression with clinical outcomes followed for 12 months following discharge (Cheok et al., 2003). Depression was diagnosed by the Center for Epidemiologic Studies Depression scale (CES-D) with scores being divided into three categories according to standard threshold scores (Ensel, 1986; Zich et al., 1990): not depressed < 16; mildly depressed 16–26, indicative of minor depression; and moderately to severely depressed ≥ 27, indicative of major depression (Cheok et al., 2003).
Patients with an admission diagnosis of AMI in the initial IDACC study were included in the present study. Mortality data, including cause of death, were obtained from the South Australian Government death register. Patients in the IDACC database were subsequently linked to the register. Patients who were initially admitted into hospital with AMI were then categorised after 5 years as being alive or deceased. Mortality was categorised as all-cause or cardiac by a cardiac clinician, who was blind to the depression status.
The study was approved by the North Western Adelaide Health Service Human Research Ethics Committee and the SA Health Ethics Committee for access to the administrative mortality database. All IDACC participants gave written informed consent.
Participants
Details of the number of patients meeting enrolment criteria and patients excluded in the IDACC study have been previously reported (Schrader et al., 2005). The IDACC database consisted of 1541 patients. The IDACC study recruited 337 patients with an admission diagnosis of AMI (aged 23–84 years, 74% males), who formed the target population in the present prospectively designed, long-term, follow-up study.
Measures
Details of the measures collected in the IDACC study have been previously reported (Cheok et al., 2003). Variables included (a) patient demographics (age, sex, marital status and index of relative socioeconomic disadvantage); (b) cardiac risk factors (body mass index (BMI), length of stay in hospital, family history of heart disease, cigarette smoking status, prior high blood pressure/high cholesterol, prior diabetes and prior heart condition/heart procedure); (c) depression risk factors (prior emotional problem and persistent depression (defined as being depressed at both baseline and 12 months)); and (d) psychometric data, including (i) quantitative depression questionnaires (CES-D) (Radloff, 1977) and Hospital Anxiety and Depression Scale (HADS) anxiety score (Zigmond and Snaith, 1983), (ii) a generic quality of life questionnaire (Short Form-36 (SF-36) mental and physical component summary score) (Ware and Sherbourne, 1992), and (iii) life event and social support questionnaires (Life Orientation Test-Revised (LOT-R) (Scheier et al., 1994) and Perceived Social Support Scale (PSSS)) (Zimet et al., 1988).
Statistical analyses
Statistical analyses were performed using the SPSS statistical software package version 11.0.4 (SPSS for Mac OS X; Chicago, IL: SPSS Inc., 2005). In the univariate analyses, ambiguous responses to categorical variables (e.g. ‘not sure/not asked/not stated’) were recoded and managed as missing values. Descriptive statistics were reported as means ± standard deviation and percentages. Initially, categorical data were analysed with the chi-squared statistic, and continuous variables with t-tests, to identify associations between the outcome of mortality at 5 years and potential predictor variables. Baseline clinical features analysed as possible predictors of mortality were based on previous literature (Carney et al., 2008; Lesperance et al., 2002; Parakh et al., 2008; Pfiffner and Hoffman, 2004; Welin et al., 2000). Baseline variables assessed in univariate analyses included (a) demographic data, (b) cardiac risk factors, (c) depression risk factors, and (d) questionnaire scores (CES-D, HADS, SF-36, LOT-R and PSSS). Analyses were performed on both continuous and categorical CES-D scores. In addition to the primary analysis, the prediction model was tested with depression defined as (1) CES-D ≥ 16 and (2) CES-D ≥ 27. Based upon the available data from the IDACC study and considering the prevalence of moderate to severe depression (CES-D ≥ 27) in the cohort, a power calculation for this investigation was performed. The study had 75% power to detect a hazard ratio of 2.5 at the p < 0.05 significance level for all-cause mortality and a 61% power for cardiac mortality.
In accordance with the recommendations of Hosmer and Lemeshow (1999), a significance level of p ≤ 0.15 in the univariate analyses was used as a criterion for entry into the multivariate analysis. A multivariate Cox proportional hazards model was developed to test the association between covariates and all-cause and cardiac mortality at 5 years. The survival time in AMI patients at 5 years was used as the dependent variable to determine the hazard ratio (HR) (exp β) and 95% confidence interval (CI) of predictor variables. Missing and ‘not sure/not asked/not stated’ responses (≥ 10 cases) for the categorical covariates were combined into a valid category to include the maximum number of records possible in the analysis and to mitigate bias. The significant variables from chi-squared and t tests were entered into the Cox model and the best predictors selected using backward elimination of non-significant terms. Models were fit separately using either continuous or categorical versions of the CES-D. Covariates were removed from the survival model one by one according to the significant criterion specified (entry = 0.05, removal = 0.06) and the model assessed at each step using the log likelihood test. The best-fit model of all the variations was determined using Akaike’s Information Criterion (AIC). The significance level for predictors of mortality in the final model was defined as p < 0.05. The accuracy of the proportional hazards assumption was tested graphically and using partial residuals.
Results
Of the 337 AMI patients, depression at baseline (defined as CES-D ≥ 16) was evident in 132 patients (39.3%) (mild depression in 76 (22.6%); moderate to severe depression in 56 (16.7%) patients), while 204 patients (60.7%) were not depressed. One case was missing depression data, and was not included in the analysis.
Vital status was determined for all patients at 5 years. There were 35 (10.4%) all-cause deaths and 22 (6.5%) cardiac deaths. Of those dying from non-cardiac causes, six died from cancer, three from respiratory failure, two from sepsis and two from renal failure. Tables 1 and 2 summarise the clinical and psychometric characteristics for all-cause and cardiac mortality, respectively.
Univariate baseline characteristics of acute myocardial infarction patients who survived to 5 years and those who died from all-causes.
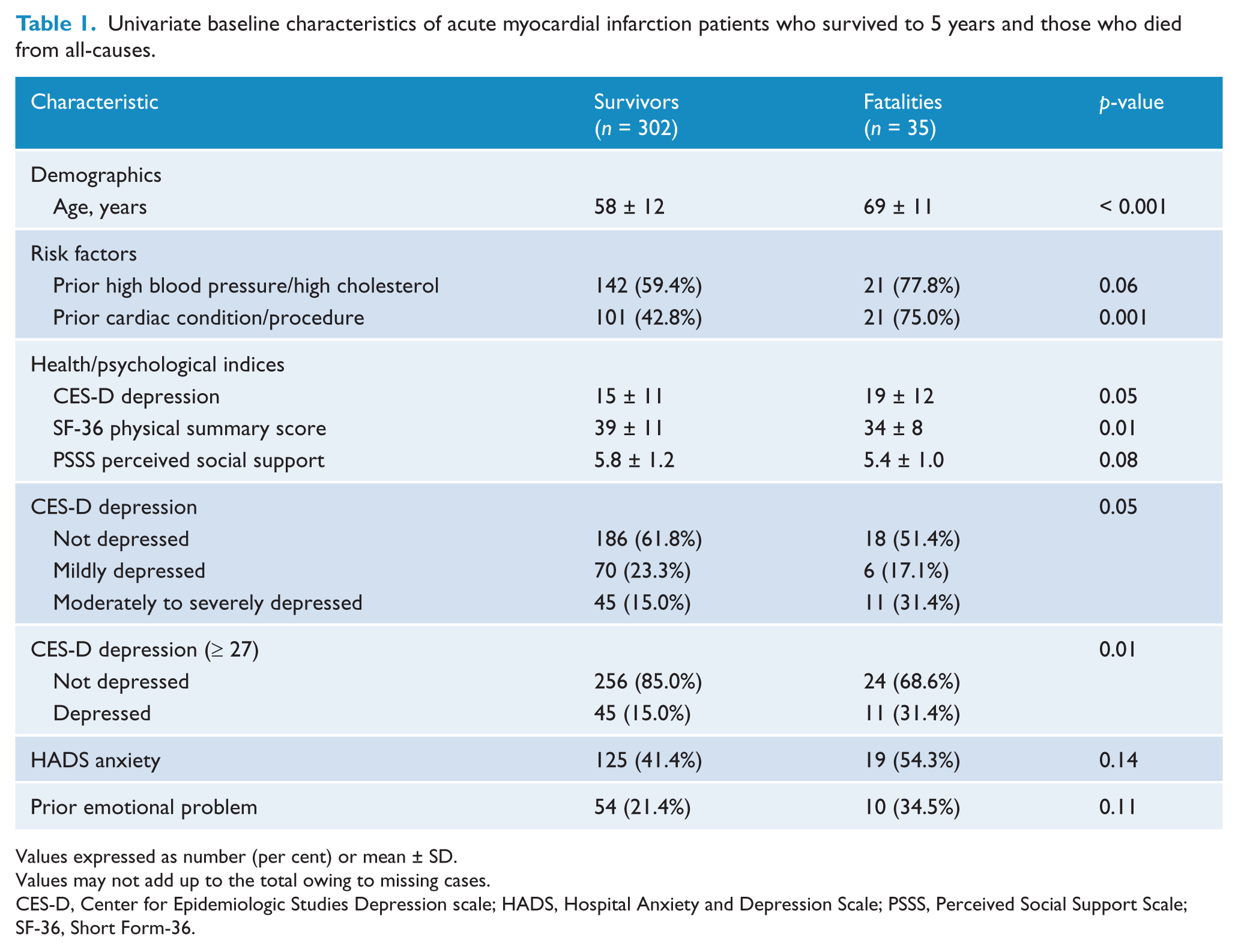
Values expressed as number (per cent) or mean ± SD.
Values may not add up to the total owing to missing cases.
CES-D, Center for Epidemiologic Studies Depression scale; HADS, Hospital Anxiety and Depression Scale; PSSS, Perceived Social Support Scale; SF-36, Short Form-36.
Univariate baseline characteristics of acute myocardial infarction patients who died from non-cardiac causes or survived to 5 years and those who died from cardiac causes.
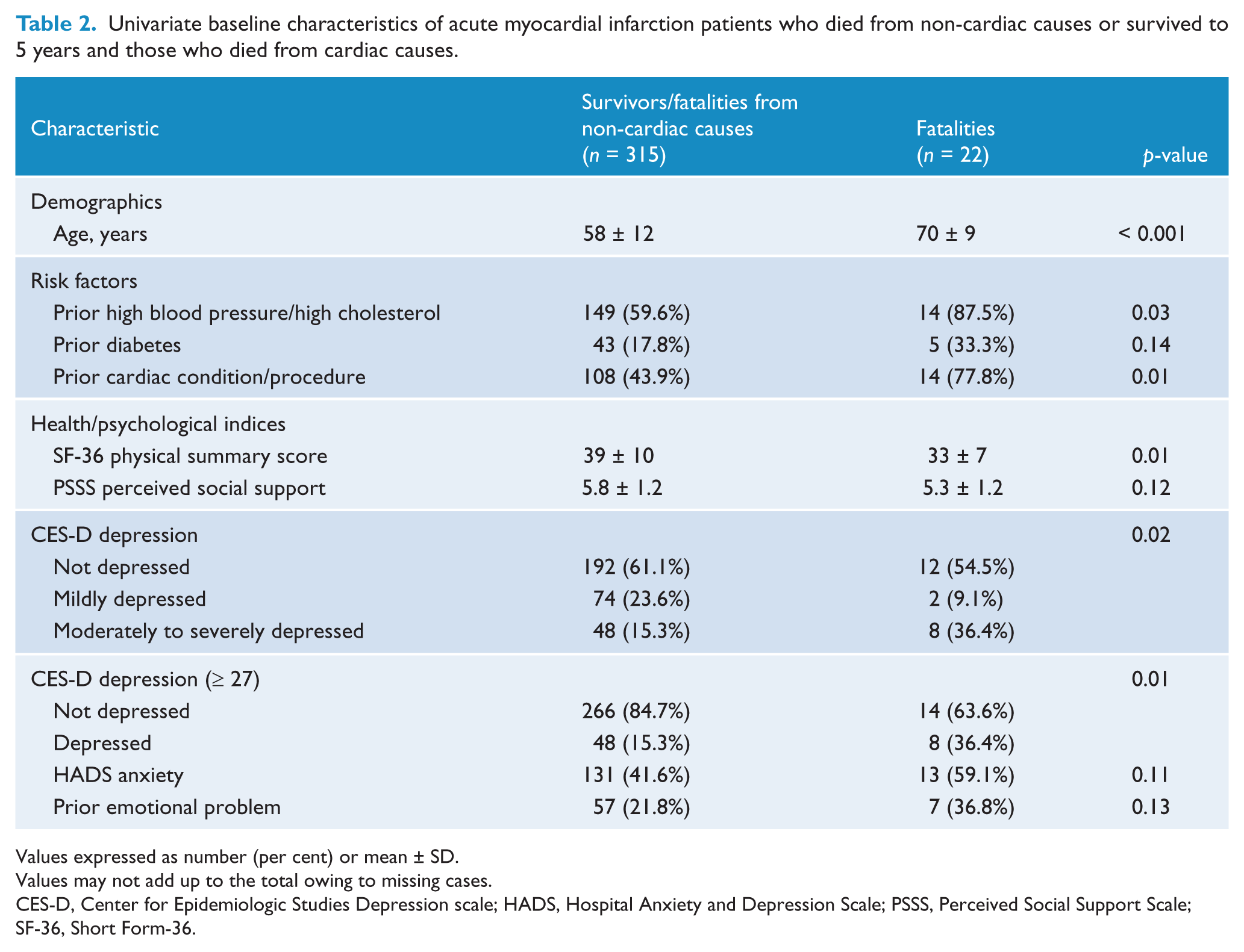
Values expressed as number (per cent) or mean ± SD.
Values may not add up to the total owing to missing cases.
CES-D, Center for Epidemiologic Studies Depression scale; HADS, Hospital Anxiety and Depression Scale; PSSS, Perceived Social Support Scale; SF-36, Short Form-36.
All-cause mortality
In the univariate analyses for all-cause mortality in AMI patients (Table 1), both the continuous and categorical CES-D (with three categories) variables were significant potential predictors of all-cause mortality at 5 years. Other potential predictors included age, SF-36 physical summary score, perceived social support, prior emotional problem, prior high blood pressure/high cholesterol, HADS anxiety score, prior cardiac condition/procedure and CES-D ≥ 27.
In the multivariate analysis, AIC was used to determine the model of best fit. Models using both categorical (with three categories) and continuous CES-D were analysed. CES-D was removed from both of the final models, as it was not found to be a significant predictor of all-cause mortality. However, age (HR 1.09, 95% CI 1.05 to 1.13; p < 0.001) and perceived social support (HR 0.70, 95% CI 0.54 to 0.90; p = 0.006) were significant independent predictors. Using CES-D as a continuous or categorical variable (with three categories) did not affect the result. However, when the CES-D score was divided into two categories (not depressed 0–26, depressed ≥ 27) depression was associated with all-cause mortality in the unadjusted model (Figure 1) and multivariate model (HR 2.54, 95% CI 1.03 to 6.28; p = 0.043). Other predictors in this model included age (HR 1.10, 95% CI 1.06 to 1.15; p < 0.001) and perceived social support (HR 0.68, 95% CI 0.50 to 0.94; p = 0.019).
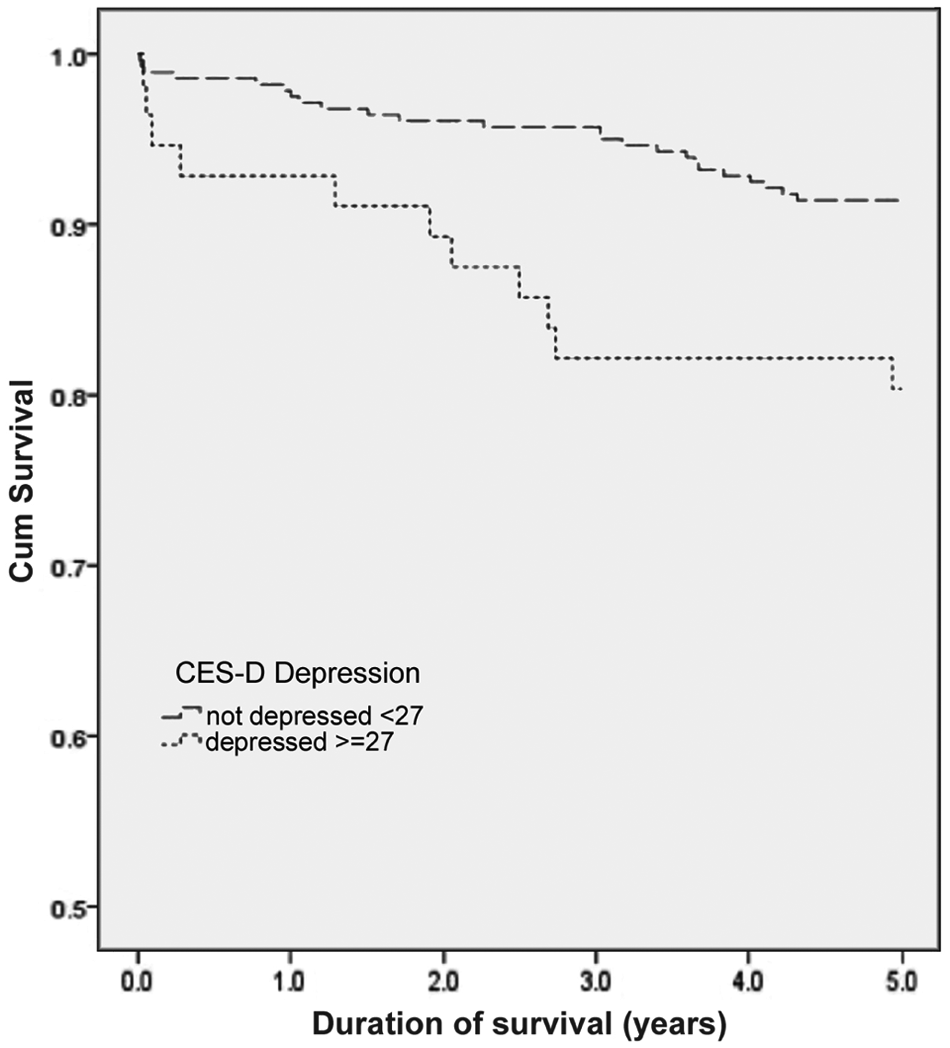
Proportion of patients surviving during 5-year follow-up by presence of depression. Kaplan–Meier survival curves are shown for patients with and without depression during the initial hospitalisation for AMI. There was a significant difference in survival between the two groups.
Cardiac mortality
Table 2 summarises the characteristics of those experiencing a cardiac cause of death within 5 years of hospital admission for AMI. Compared with the survivors/fatalities from non-cardiac causes, patients who died of a cardiac cause were older, had more risk factors and were more likely to have a prior cardiac condition. They were also more depressed and had a poorer quality of life at the time of study recruitment (Table 2).
When cardiac death was analysed in AMI patients, univariate analyses showed that age, SF-36 physical summary score, perceived social support, prior emotional problem, prior high blood pressure/high cholesterol, prior diabetes, HADS anxiety score, prior cardiac condition/procedure, categorical CES-D (with three categories) and CES-D ≥ 27 were potential predictors of cardiac mortality in AMI patients (Table 2).
However, in the multivariate model, depression was not significantly associated with 5-year cardiac mortality. Other predictors of increased mortality included age (HR 1.10, 95% CI 1.05 to 1.15; p < 0.001) and perceived social support (HR 0.67, 95% CI 0.49 to 0.93; p = 0.016). Results did not change when CES-D was divided into two categories: not depressed 0–26 and depressed ≥ 27.
Discussion
The major finding of this study was that moderate to severe depression (defined as CES-D ≥ 27) predicted all-cause but not cardiac 5-year mortality in AMI patients. However, when the cut-off for depression was lowered (i.e. CES-D ≥ 16), that is, when patients with milder depression were also included in the analyses, depression was not found to be predictive of either all-cause or cardiac mortality. We did not find that depression was associated with either all-cause or cardiac mortality when CES-D was analysed as a continuous variable. This may indicate that the relationship between mortality and depression severity is not linear and that the association only becomes evident when the severity reaches a threshold level (e.g. CES-D ≥ 27), consistent with major depression. The findings of this study are similar to others in reporting an association between depression and long-term mortality (Carney et al., 2008; Lesperance et al., 2002; Pfiffner and Hoffman, 2004; Welin et al., 2000), while different from those who failed to find an association (Dickens et al., 2007; Parakh et al., 2008).
Previous studies of depression and long-term mortality in AMI patients
The population studied was similar with respect to depression prevalence (CES-D ≥ 16) to that of Drago et al.’s study (2007) (Beck Depression Inventory (BDI) ≥ 10). The prevalence of moderately to severely depressed AMI patients in our study was also similar to that of the major depressive disorder (MDD) prevalence in Drago et al.’s study (2007). However, they reported an increased risk of mortality in patients with MDD compared with those who had mild to moderate depression, as assessed by the BDI (Drago et al., 2007). This suggests a direct correlation between the severity of depression and its influence on prognosis. Similarly, Carney et al. (2008) reported that both minor and major depression were predictive of 5-year all-cause mortality in AMI patients; however, the hazard was higher for major depression than for minor depression. It may be that the CES-D scale we used to measure depression included less severely depressed patients in its mild depression category than the BDI used by Drago et al. (2007) and Carney et al. (2008). This may explain our finding that CES-D ≥ 16 did not predict mortality.
Our finding that perceived social support is associated with all-cause and cardiac mortality is consistent with others who have found that social isolation is associated with a worse prognosis and mortality after MI (Welin et al., 2000). Furthermore, Pfiffner and Hoffman (2004) found that the lack of a partner predicted mortality. The mechanisms underlying this association have not been well explained. It may be that people lacking social support are less capable of controlling their cardiovascular risk factors or they may respond later to premonitory symptoms (Welin et al., 2000). Although perceived social support was an independent predictor of mortality in AMI patients, this does not preclude there being a relationship between perceived social support and depression.
Why moderate to severe depression was related to all-cause and not cardiac-specific mortality in AMI patients is unclear from our study. In part it may be related to an insufficient sample size, thus requiring a larger cohort for the more specific cardiac mortality endpoint. In our study, similar to others (Dickens et al., 2007; Parakh et al., 2008; Pfiffner and Hoffman, 2004; Welin et al., 2000), cigarette smoking status, BMI, family history of heart disease, prior high blood pressure/high cholesterol or diabetes were not predictors of all-cause or cardiac mortality in AMI patients. However, psychosocial factors have been reported to be predictive of the development and prognosis of cardiovascular disease (Bunker et al., 2003; Everson-Rose and Lewis, 2005).
Discrepancies between the findings of the present study and other studies (Carney et al., 2008; Lesperance et al., 2002; Pfiffner and Hoffman, 2004; Welin et al., 2000) may be related to differences in the management of the AMI patient populations, which have occurred over the last few decades. The 5-year death rates in our study were lower than in earlier studies examining the impact of depression on mortality in MI patients (Carney et al., 2008; Lesperance et al., 2002), which may possibly be due to the greater efficacy of contemporary therapies for coronary heart disease (Lamy et al., 2011). Exposure to newer therapies may have modified the impact of depression on long-term mortality. The IDACC cohort was recruited from 2000 to 2002, and subsequently exposed to newer, more effective cardiac interventions, compared with earlier cohorts where depression emerged more clearly as a predictor of mortality. Of note, no association between depression and mortality was found in Parakh et al.’s recent study (2008). However, their study (Parakh et al., 2008) analysed a higher risk population in terms of co-morbidities than the cohort we examined.
Study limitations
This study had several limitations. A baseline self-rated measure of depression was used in this study, and patients did not undergo diagnostic interviews by clinicians. Information on whether the depressed patients in hospital were still depressed at the time of their death or up to 5 years was also not available. Length of stay in the index hospital was used as a proxy for severity of AMI, as severity risk factors were not available, and long-term antidepressant medication usage was not collected. Information relating to the use of antipsychotic drugs, multiple medical comorbidities and level of physical activity was also not collected. Despite these limitations, data analysed in this report came from a multicentre study with a large patient population, where patients were exposed to more recent therapeutic advances. The analyses were also broken down into all-cause and cardiac mortality, while many studies are limited to one or the other (Carney et al., 2008; Dickens et al., 2007; Drago et al., 2007; Lesperance et al., 2002; Parakh et al., 2008).
The present findings highlight the complexity of the association between depression and long-term mortality after AMI. Nonetheless, we found an association between moderate to severe depression (measured by self-report during hospital admission for AMI) and all-cause mortality over the subsequent 5-year period in a cohort of patients exposed to contemporary cardiac care. This finding may have implications for the routine use of screening depression in patients admitted to hospital for AMI. Future research designed to establish causal relationships by analysing longitudinal data combining repeated measurements of depression and pathophysiological mechanisms would be beneficial (Lesperance et al., 2002).
Footnotes
Funding
AW was funded by a Queen Elizabeth Hospital Post Graduate Scholarship.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.