
Abstract
Background:
The scientific literature on stigma has been confused because there are multiple components of stigma with different correlates. In order to help make sense of this confusion, the present review focuses on research on one of the most commonly measured components - belief in dangerousness.
Method and Results:
The review examines: measurement of belief in dangerousness; prevalence of belief in dangerousness; characteristics of people who believe in dangerousness; experiences associated with belief in dangerousness; characteristics of people that elicit belief in dangerousness; the effects of psychiatric labelling; the effects of causal explanations; interventions to reduce belief in dangerousness; and effects on help-seeking.
Conclusion:
It is concluded that future research needs to focus on rigorous evaluation of interventions to reduce belief in dangerousness and the impact of this belief on people affected by mental disorders.
Introduction
Stigma was defined in the 2001 World Health Report as “a mark of shame, disgrace or disapproval which results in an individual being rejected, discriminated against, and excluded from participating in a number of different areas of society” (WHO, 2001). While there is an extensive literature on stigma, this is often confusing, with many apparently inconsistent findings. One of the reasons for this confusion is that stigma is not a unitary construct. Factor analytic studies have reported multiple dimensions and these dimensions may have different correlates. A way through this complexity is to focus on specific aspects of stigma that have been measured in fairly consistent ways. In a previous review, this was done for the literature using a measure of social distance, because this is the most commonly measured component of stigma (Jorm and Oh, 2009). The present review continues this approach by focusing on another commonly measured component – belief in dangerousness of people with a mental disorder. Dangerousness has been measured both in terms of dangerousness to others and dangerousness to self. In this review the focus is on belief in dangerousness to others.
As a preliminary to reviewing the evidence on public beliefs, it is worth briefly examining what is known about the risk of dangerous behaviour in people with mental disorders. Torrey (2011a,b) has argued that violent behaviour by mentally ill people is the major cause of stigma. Indeed, systematic reviews have found that schizophrenia, other psychoses and bipolar disorder are associated with increased risk of violence, however much of the association is due to associated substance misuse or non-adherence to treatment (Douglas et al., 2009; Fazel et al., 2009, 2010; Yee et al., 2011).Violence is more likely in people in a first episode of psychosis before presenting for treatment (Large and Nielssen, 2011). Associations have also been found with substance use disorders, depression, some anxiety disorders, and personality disorders, with comorbid disorders having stronger associations (Pulay et al., 2008). However, despite this increased risk, the overwhelming majority of people with mental disorders are not violent (Pulay et al., 2008).
Methods
The academic literature was systematically searched through PsycINFO and PubMed to include publications that met the following criteria: (i) described a study that involved the measurement of the perception of dangerousness in mentally ill people; and (ii) focused on mental disorders that included any psychiatric disorder, with the exception of mental retardation.
The searches included all studies between 1970 and 6 July 2011 and were limited to English language publications. A keyword search in PsycINFO used danger OR dangerousness AND attitude OR perception OR perceived AND ‘mental disorder’. Using an autoexplode strategy, the same keyword search on PubMed was carried out with the addition of medical subject headings for mental disorder. Additional papers were found by searching the reference lists of already retrieved studies, dating back to 1962, and altogether 1115 articles were identified (Figure 1). Dissertations were excluded because of the difficulty of obtaining them.
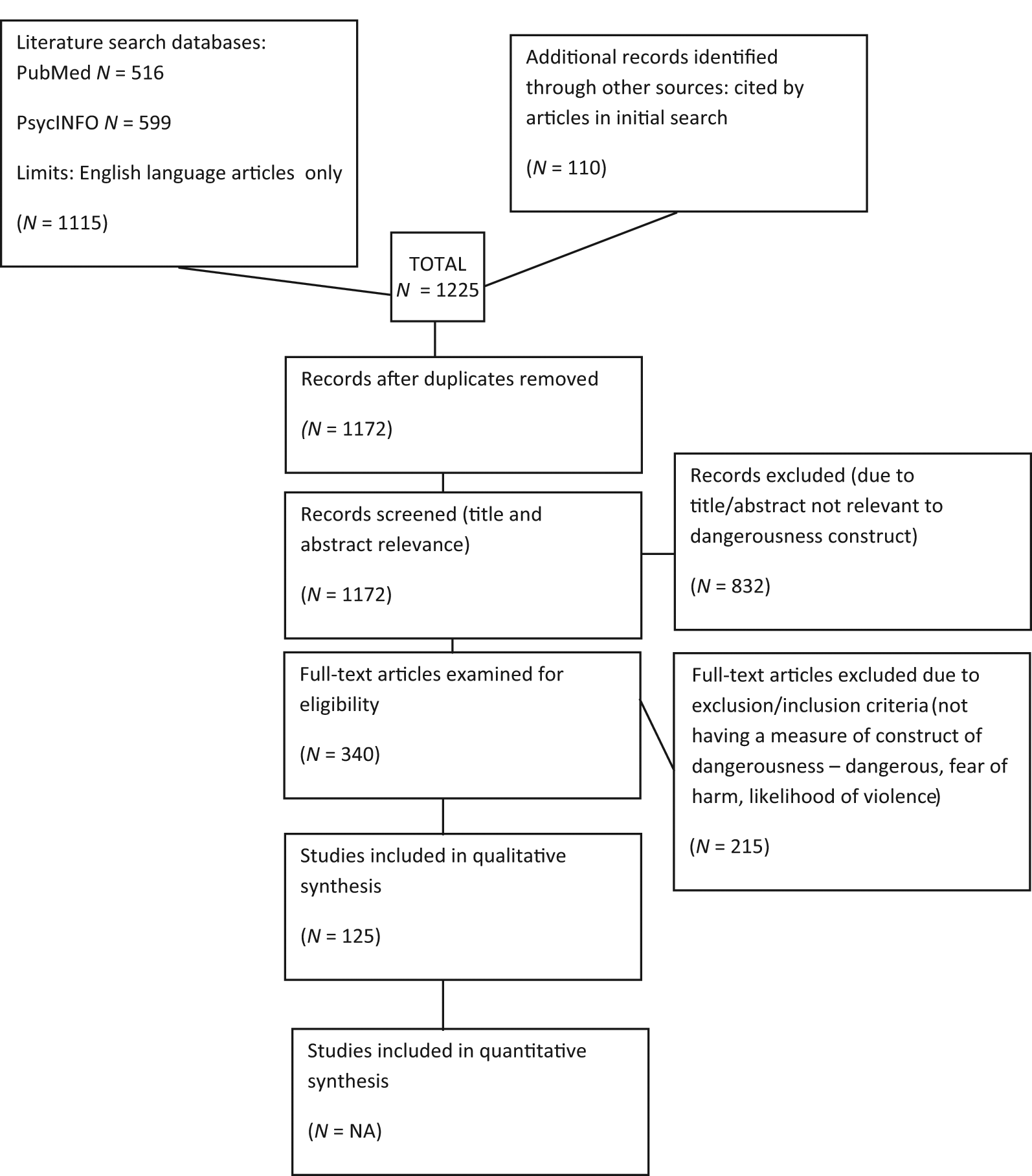
PRISMA flow diagram of the literature search and screening process
The studies were reviewed by one author and subsequently checked for accuracy by another author. The studies were reviewed by organizing them according to the variables examined, and specific conclusions were arrived at in relation to each variable. However, to increase readability, the results are presented under headings stating each of these conclusions.
Results
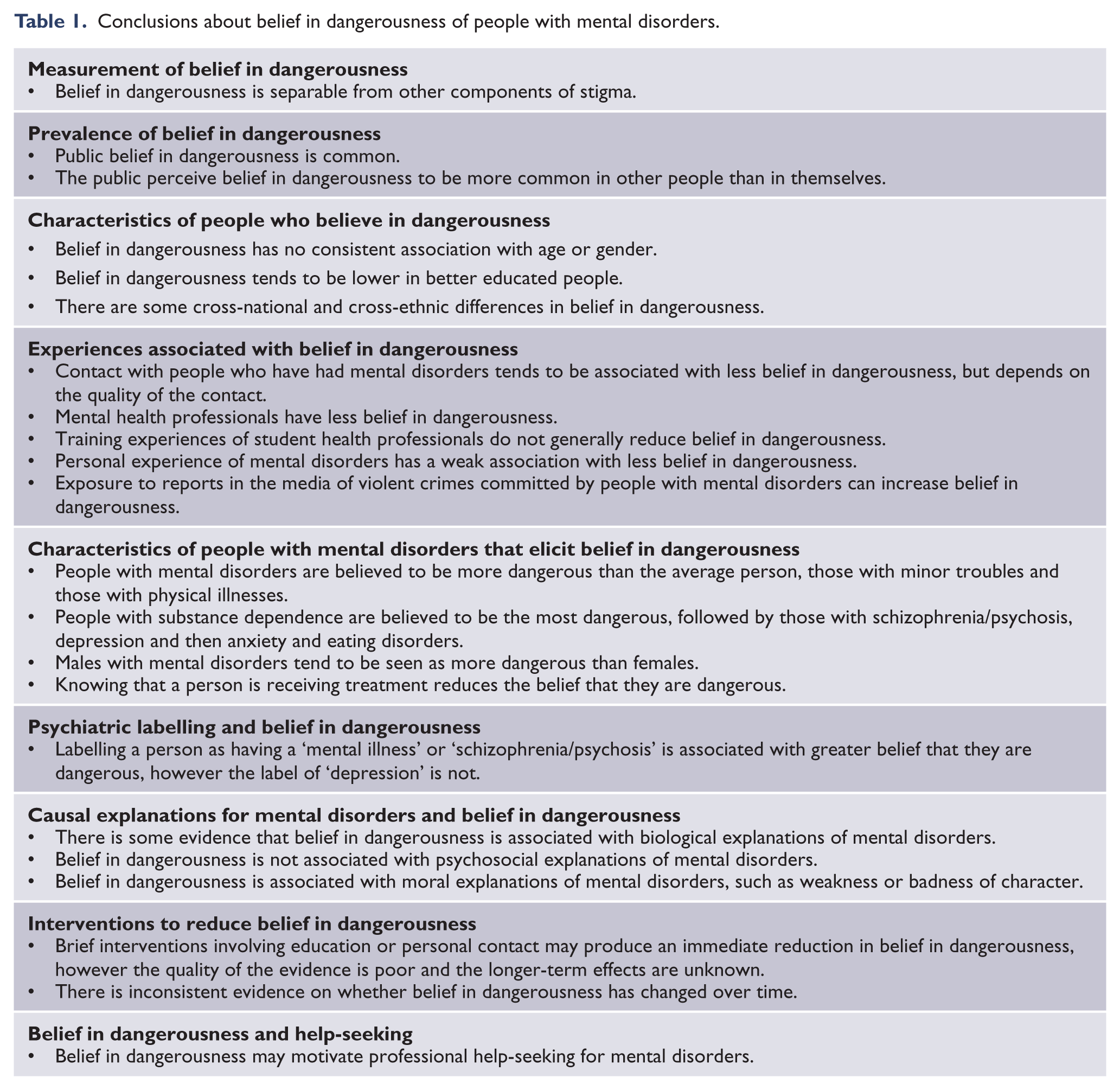
The results of this review can be summarized as the set of conclusions in Table 1. The literature justifying each of these conclusions is reviewed in detail below.
Conclusions about belief in dangerousness of people with mental disorders.
Measurement of belief in dangerousness
Belief in dangerousness is separable from other components of stigma
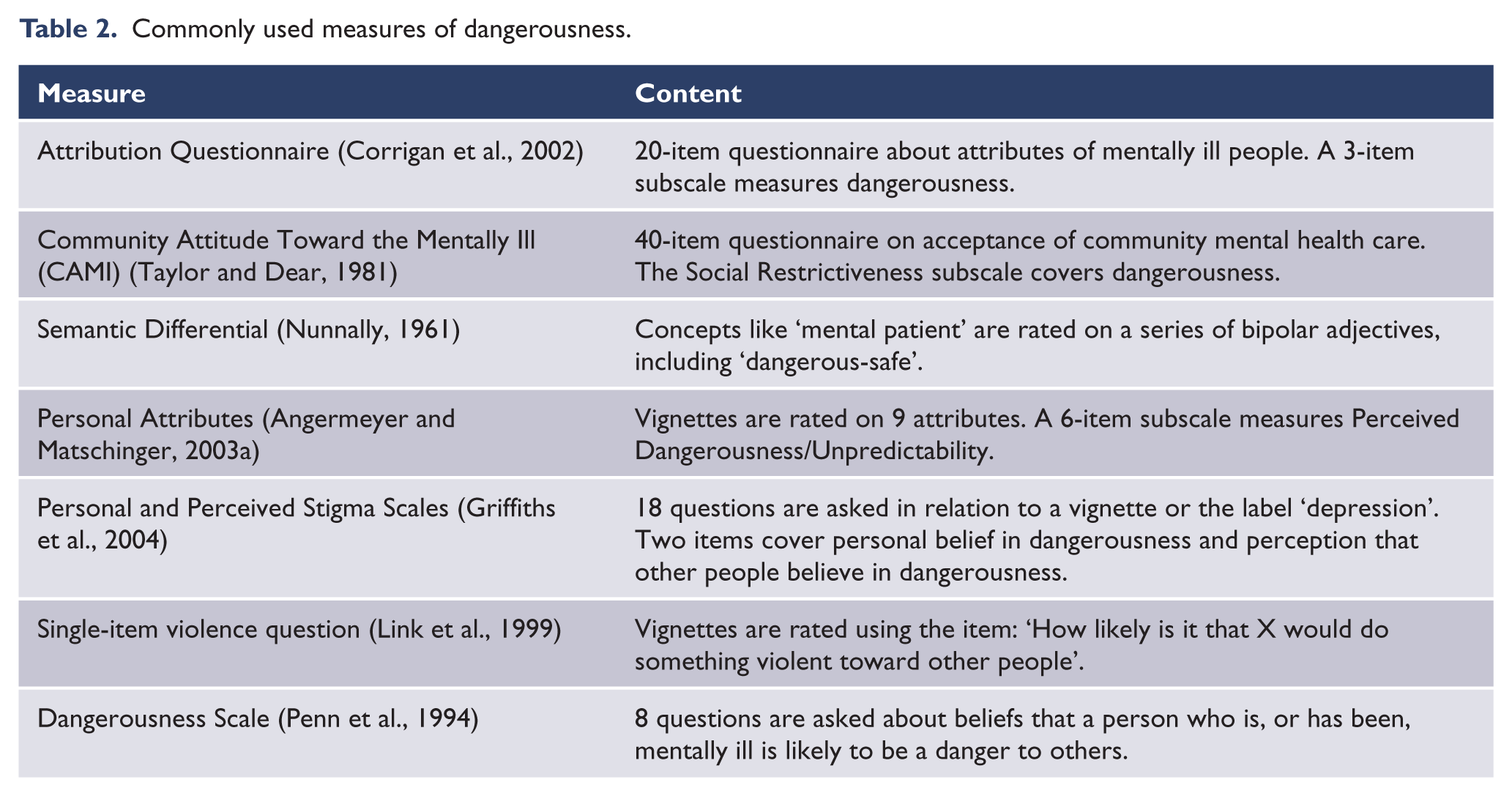
Belief in dangerousness has been measured in a variety of ways, with no particular measure predominating. Some studies use a single question about dangerousness, others use a general stigma measure which contains one or more questions on dangerousness, or a multiple-item dangerousness scale. The more commonly used measures are shown in Table 2.
Commonly used measures of dangerousness.
Many studies have used factor analysis, principal components analysis or cluster analysis on sets of stigma items and these have commonly found a clearly identifiable ‘dangerousness’ factor (Angermeyer and Matschinger, 2003a; Cooper et al., 2003; Corrigan et al., 2002; Dietrich et al., 2006b; Furnham and Chan, 2004; Furnham and Rees, 1988; Furnham and Wong, 2007; Furnham et al., 2008; Jorm and Wright, 2008; Lauber et al., 2006; Levey and Howells, 1995; Norman et al., 2008; Robbins et al., 1988; Romney and Bynner, 1985; Shurka, 1983; Wilkinson, 1982; Wolkenstein and Meyer, 2009). Other attributes that are commonly found to load on this factor are: violent, unpredictable, frightening, untrustworthy, lacking in self-control, and need to be institutionalized. A number of other studies have not found a dangerousness factor, but these have generally had poor representation of this domain of content (Brockington et al., 1993; Cohen and Struening, 1962; Furnham and Igboaka, 2007; Griffiths et al., 2008; Hogberg et al., 2008; Tanaka et al., 2004; Watson et al., 2005b). In some of these studies, a ‘dangerous’ item is found to load on a broader factor of stigmatizing attitudes (Cohen and Struening, 1962; Griffiths et al., 2008; Hogberg et al., 2008).
Dangerousness has also been found as a theme in qualitative studies. A qualitative study on nurses’ attitudes to people with borderline personality disorder found a core theme labelled ‘destructive whirlwind’ which included the concept of dangerousness (Woollaston and Hixenbaugh, 2008). Similarly, a study of nurses and nursing assistants in forensic mental health settings found a theme of dangerousness (Lammie et al., 2010). A study using focus groups with the Jamaican public found a theme of ‘emotional responses towards those with mental illness’, with a fear of dangerousness being the most commonly expressed emotional response (Arthur et al., 2010).
Dangerousness shows differentiation from another major stigma component, social distance. Where correlation coefficients between dangerousness and social distance scales have been reported, the median is 0.4, with correlations typically higher for schizophrenia than for depression (Corrigan et al., 2001; Horch and Hodgins, 2008; Link et al., 1999; Marie and Miles, 2008; Markham, 2003; Norman et al., 2008; Penn et al., 1994; Phelan and Basow, 2007).
Prevalence of belief in dangerousness
Public belief in dangerousness is common
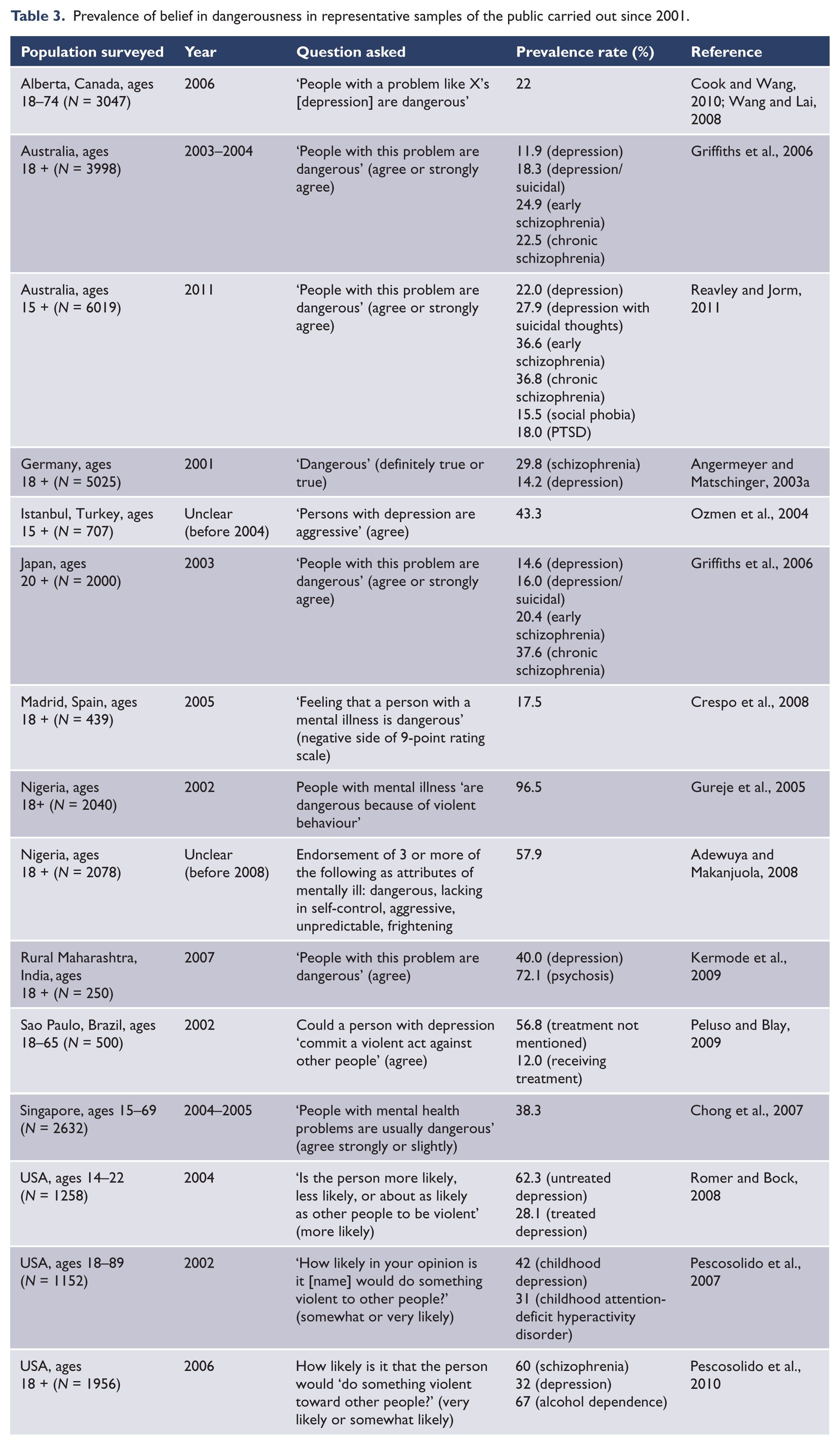
Table 3 summarizes the findings from representative samples of the public carried out since 2001. It can be seen that the prevalence of belief in dangerousness varies considerably from study to study, and that it is influenced by the particular mental disorder asked about and whether the person is receiving treatment. However, belief in dangerousness is relatively common in all communities.
Prevalence of belief in dangerousness in representative samples of the public carried out since 2001.
The public perceive belief in dangerousness to be more common in other people than in themselves
Surveys of the public in Australia, Germany and Japan have asked respondents about both their own personal beliefs and what they think most other people’s beliefs are (Griffiths et al., 2006; Reavley and Jorm, 2011; Wolkenstein and Meyer, 2008). In all these surveys, the public perceived that other people believed in dangerousness more than they did themselves.
Characteristics of people who believe in dangerousness
Belief in dangerousness has no consistent association with age or gender
In community surveys of adults covering a broad age range, most studies find no association with age (Angermeyer and Matschinger, 1996; Anglin et al., 2006; Cook and Wang, 2010; Gureje et al., 2005; Jorm and Griffiths, 2008; Levey and Howells, 1995; Peluso and Blay, 2009; Pescosolido et al., 1999, 2007; Schnittker, 2000). However, some studies have found that belief in dangerousness is greater in older people (Brockington et al., 1993; Chong et al., 2007; Link and Cullen, 1986; Mojtabai, 2010; Wolff et al., 1996a), one study has found it less likely (Crisp et al., 2000), and one has found a curvilinear relationship, with belief in dangerousness higher in both younger and older adults (Phelan and Link, 2004). In young people, one study found that belief in dangerousness was higher in young adults than in adolescents (Jorm and Wright, 2008), but other studies of adolescents have found no association with age or grade (Dietrich et al., 2006a; Minnebo and Van Acker, 2004).
Gender differences in beliefs have been examined in a wide range of samples and most studies report no difference (Angermeyer and Matschinger, 1996; Brockington et al., 1993; Cook and Wang, 2010; Crisp et al., 2000; Dietrich et al., 2006a; Gureje et al., 2005; Jorm and Griffiths, 2008; Lauber et al., 2006; Levey and Howells, 1995; Link and Cullen, 1986; Norman et al., 2008; Pescosolido et al., 1999, 2007; Phelan and Link, 2004; Phelan et al., 2000; Schnittker, 2000; Webb et al., 2009; Wolff et al., 1996a). The few studies that do report a gender difference are not consistent in their findings (Mojtabai, 2010; Peluso and Blay, 2009).
Belief in dangerousness tends to be lower in better educated people
Numerous studies have found that belief in dangerousness is lower in better educated people (Aghukwa, 2009; Brockington et al., 1993; Chong et al., 2007; Cook and Wang, 2010; Jorm and Griffiths, 2008; Link and Cullen, 1986; Mojtabai, 2010; Nunnally, 1961; Pescosolido et al., 1999; Phelan and Link, 2004; Psarra et al., 2008; Rao et al., 2007; Schnittker, 2000; Shurka, 1983). However, there are also some studies showing no association (Anglin et al., 2006; De Toledo Piza Peluso and Blay, 2009; Gureje et al., 2005; Levey and Howells, 1995; Pescosolido et al., 2007; Phelan et al., 2000; Wolff et al., 1996a) and one study showing the opposite association (Angermeyer and Matschinger, 1996).
There are some cross-national and cross-ethnic differences in belief in dangerousness
Because the way the question is asked may affect the results found, cross-national and cross-ethnic differences need to be studied using the same methodology in the groups being compared. When this has been done, a number of differences have been found. Belief in dangerousness has been reported as lower in UK samples compared to samples from various Asian countries – China, Japan and Pakistan (Furnham and Chan, 2004; Furnham and Murao, 1999; Furnham and Wong, 2007; Furnham et al., 2008). A comparison of Australia and Japan found less belief in the dangerousness of a person with chronic schizophrenia in Australia, but no difference in beliefs about early schizophrenia or depression (Griffiths et al., 2006).No difference has been reported between young people from the UK and Nigeria (Furnham and Igboaka, 2007), or between pharmacy students from six different countries (Bell et al., 2008).
In the USA, a number of studies have reported that belief in dangerousness is greater in racial minority groups (Anglin et al., 2006; Pescosolido et al., 1999; Phelan and Link, 2004; Phelan et al., 2000; Rao et al., 2007; Schnittker, 2000; Whaley, 1997), although there are some studies which do not show an association (Granello et al., 1999; Pescosolido et al., 2007). A New Zealand student study found that Asians had greater belief in dangerousness than Europeans or Maori, while an English survey found no race differences (Read and Harre, 2001; Wolff et al., 1996b).
Experiences associated with belief in dangerousness
Contact with people who have had mental disorders tends to be associated with less belief in dangerousness, but depends on the quality of the contact
One of the most researched correlates of belief in dangerousness is contact with people who have experienced mental disorders, a concept often referred to as familiarity. Typically, contact has been through having family or friends who are affected by a mental disorder. Reports of contact have been found to be associated with less belief in dangerousness across a broad range of populations (Angermeyer et al., 2004; Brockington et al., 1993; Corrigan et al., 2001; Grausgruber et al., 2007; Link and Cullen, 1986; Penn et al., 1994; Phelan and Link, 2004; Read and Harre, 2001; Read and Law, 1999; Thompson et al., 2002; Whaley, 1997), but there are many studies that do not report such an association (Beiser et al., 1987; Crisp et al., 2000; Granello et al., 1999; Jorm and Griffiths, 2008; Jorm and Wright, 2008; Levey and Howells, 1995; Marie and Miles, 2008; Phelan and Basow, 2007; Van Dorn et al., 2005; Wang and Lai, 2008; Wolff et al., 1996b; Wolkenstein and Meyer, 2009). It is notable, however, that no study has found that contact is associated with greater belief in dangerousness. It has been proposed that the inconsistent findings in the literature occur because quality of the contact is important (Couture and Penn, 2003), but quality has not been assessed in these studies. However, there is evidence that negative experiences, such as being threatened or physically harmed, are associated with greater belief in dangerousness (Phelan and Link, 2004), which may sometimes offset the positive benefits of contact.
Although there is evidence that contact can be associated with reduced belief in dangerousness, the causal interpretation of this association is unclear. Good-quality contact might reduce belief in dangerousness, but it is also possible that people who believe in dangerousness avoid contact. One study attempted to clarify the causality by distinguishing between contact that is likely to be affected by belief in dangerousness (e.g. chosen contact such as volunteering work or visiting a hospital) and contact that is unlikely to be (e.g. knowing someone who was once hospitalized) (Link and Cullen, 1986). This study found that both types of contact were associated with less belief in dangerousness, but the association was stronger with unchosen contact, supporting a causal role for contact.
The only sure way to test whether contact is causal is to have an experimental intervention. Only one randomized trial has been carried out (Corrigan et al., 2002). This compared contact with an educational intervention and no intervention in US college students. Contact was found to reduce belief in dangerousness more than no intervention, supporting a causal role, but the effects were not maintained at 1 week follow-up.
Mental health professionals have less belief in dangerousness
If involuntary contact does lead to less belief in dangerousness, then it would be expected that mental health professionals would have less belief, because contact is required by their work. Indeed, a number of studies have found that mental health professionals have less belief in dangerousness than the public (Brockington et al., 1993; Grausgruber et al., 2007; Lauber et al., 2004; Van Dorn et al., 2005), although there are others showing no difference (Cook and Wang, 2010; Jorm and Griffiths, 2008; Lauber et al., 2006). Similar findings emerge from studies comparing mental health professionals with other health professionals, which all show less belief in dangerousness in the mental health professionals (Bjorkman et al., 2008; Calicchia, 1981; Markham, 2003). Importantly, no study has found that professional contact increases belief in dangerousness.
Training experiences of student health professionals do not generally reduce belief in dangerousness
Studies of university students training to be health professionals are also relevant in this regard. One survey of medical students found that they had less belief in dangerousness than the public (Thompson et al., 2002), but another survey of nursing and psychology students found no difference (Levey and Howells, 1995). Studies looking at changes in attitudes as a result of students’ training (which includes contact with people with mental disorders) have consistently found no reduction in belief in dangerousness (Ay et al., 2006; Bell et al., 2006; Fabrega, 1995; Wilkinson, 1982). Indeed, one study found that medical students had increased belief in the dangerousness of people with schizophrenia (Ay et al., 2006). These negative findings may reflect the quality of the contact that students have, often involving acutely unwell people.
Personal experience of mental disorders has a weak association with less belief in dangerousness
Some surveys have found that people with personal experience of mental disorders have less belief in dangerousness than other community members (Angermeyer et al., 2004; Brockington et al., 1993; Walker and Read, 2002; Wolkenstein and Meyer, 2009), but more studies report no association (Beiser et al., 1987; Cooper et al., 2003; Levey and Howells, 1995; Romer and Bock, 2008; Van Dorn et al., 2005; Wolff et al., 1996b). If an association exists, it is likely to be weak.
Exposure to reports in the media of violent crimes committed by people with mental disorders can increase belief in dangerousness
There have been two studies where the public were surveyed before and after violent crimes that were widely reported in the media. The first study involved a survey in England a few months before the Hungerford massacre, with follow-up surveys carried out 2 weeks and 6 months after (Appleby and Wessely, 1988). There was no change in belief that mentally ill people are likely to be violent, however there was a temporary increase in the belief that people who commit horrific crimes are likely to be mentally ill. The second study involved surveys of the German public before and after two widely reported violent attacks on politicians by people with schizophrenia (Angermeyer and Matschinger, 1996). This study found an increase in belief in dangerousness, which reduced again in the following 2 years.
There have also been experimental studies in which students have been assigned to read a newspaper article about a violent crime. One study assigned university students to read an article about a violent crime committed by a mental patient or a control article (Thornton and Wahl, 1996). There was a non-significant trend for the group reading the violent article to have greater belief in dangerousness at post-test, but unfortunately the study took no pre-test measure. A better designed study of German high school children randomized them to either read an article linking mental illness with violent crime or one providing factual information on schizophrenia (Dietrich et al., 2006a). The article on violent crime was found to lead to increased belief in dangerousness.
Media reporting of crimes may have an adverse effect on public attitudes even in instances where there is no explicit mention of mental illness as a factor in a crime. A household survey in the USA asked respondents to describe any reports on the criminally insane they had heard about in the media and found that 42% were able to name someone (Steadman and Cocozza, 1978). All the people named were high-profile murderers, but analysis of court records showed that not one of the people named had been classified as legally insane. Rather, the public tended to attribute mental illness to these murderers based on the nature of their crime. In fact, court records showed that the typical crimes committed by people with mental illness were robbery, burglary and assault rather than murder.
Characteristics of people with mental disorders that elicit belief in dangerousness
People with mental disorders are believed to be more dangerous than the average person, those with minor troubles and those with physical illnesses
Surveys of the public and students have uniformly found that people with ‘mental illness’ or a variety of specific mental disorders are believed to be more dangerous than the average person (Horch and Hodgins, 2008; Nunnally, 1961; Steadman and Cocozza, 1978), people with minor troubles or people who are stressed (Link et al., 1999; Minster and Knowles, 2006; Pescosolido et al., 2007; Phelan and Basow, 2007; Silton et al., 2011), and people with physical illnesses like asthma, cancer and heart disease (Horch and Hodgins, 2008; Martinez et al., 2011; Pescosolido et al., 2007; Ramon, 1978).
People with substance dependence are believed to be the most dangerous, followed by those with schizophrenia/psychosis, depression and then anxiety and eating disorders
The most common method for comparing beliefs about dangerousness across different disorders has been to present members of the public or students with case vignettes. Vignette studies in a variety of samples have found that people with schizophrenia/psychosis are rated as more likely to be dangerous than those with depression (Angermeyer et al., 2004; Ay et al., 2006; Griffiths et al., 2006; Jorm and Wright, 2008; Kermode et al., 2009; Link et al., 1999; Marie and Miles, 2008; Norman et al., 2008; Pescosolido et al., 1999; Silton et al., 2011; Webb et al., 2009).There has been less research on substance use disorders. However, these studies show that substance dependence is seen as more dangerous than schizophrenia (Horch and Hodgins, 2008; Link et al., 1999; Pescosolido et al., 1999; Silton et al., 2011), although milder substance abuse is not (Jorm and Wright, 2008; Marie and Miles, 2008). There is also evidence from vignette studies that mania is seen as more dangerous than depression (Wolkenstein and Meyer, 2009), and depression as more dangerous than anxiety disorders (Jorm and Wright, 2008; Reavley and Jorm, 2011; Webb et al., 2009).
Males with mental disorders tend to be seen as more dangerous than females
A number of studies have examined perceptions of dangerousness for male and female vignettes describing the same behaviours. In general, male vignettes are rated as more dangerous than female vignettes, particularly where more severe psychotic disorders are portrayed (Jorm and Griffiths, 2008; Nunnally, 1961; Pescosolido et al., 2007; Reavley and Jorm, 2011; Schnittker, 2000; Silton et al., 2011). Although some studies show no difference (Norman et al., 2008; Peluso and Blay, 2009). Where clinicians are asked to rate dangerousness in actual patients, they also tend to rate this as higher in males (Elbogen et al., 2001; Levinson and York, 1974), although whether this represents perception or a real difference was not determined. The perception of greater dangerousness in males has some grounding in reality; for example, there are higher rates of violence in males with psychosis than in females (Large and Nielssen, 2011).
Knowing that a person is receiving treatment reduces the belief that they are dangerous
Mentally ill people who are treated are seen as less dangerous than those who are not (Peluso and Blay, 2009; Romer and Bock, 2008), and those who have completed treatment less dangerous than those in treatment (Olmsted and Durham, 1976). Furthermore, people who believe in the treatability of mental illness have less belief in dangerousness (Arikan et al., 1999; Savrun et al., 2007). The belief that treatment can reduce dangerousness has some basis, because risk of violence is increased when there is non-treatment or non-adherence to treatment (Large and Nielssen, 2011; Yee et al., 2011).
Psychiatric labelling and belief in dangerousness
Labelling a person as having a ‘mental illness’ or ‘schizophrenia/psychosis’ is associated with greater belief that they are dangerous, however the label of ‘depression’ is not
A number of studies have presented participants with diagnostic labels and ask for ratings of likely dangerousness. These studies have been carried out with members of the public, students and a variety of health professionals. In general, studies where diagnostic labels are rated concur with the findings from vignette studies reviewed above. Dangerousness is generally seen as higher in substance dependence than in schizophrenia/psychosis (Bjorkman et al., 2008; Crisp et al., 2000; Mukherjee et al., 2002; Romney and Bynner, 1985) and in schizophrenia/psychosis than depression/anxiety (Bell et al., 2008; Crisp et al., 2000; Markham, 2003; Servais and Saunders, 2007), although there are some exceptions (Bell et al., 2006). There are fewer studies on other diagnostic labels, but some studies have found that borderline personality disorder is rated high (Markham, 2003; Servais and Saunders, 2007). By contrast, the label of bipolar disorder is not associated with dangerousness (Martinez et al., 2011), while eating disorders are rated low (Bjorkman et al., 2008; Crisp et al., 2000; Mukherjee et al., 2002). A qualitative study of public reactions to various labels found that ‘insane’ was more associated with dangerousness than ‘mentally ill’, while ‘depressed’ was the least associated (Goodfellow et al., 2010).
A limitation of the studies presenting labels alone is that they do not tease out the contribution of labelling from the contribution of the person’s behaviour to ratings of dangerousness. More relevant in this regard are studies that present a vignette and also ask the participant what is wrong with the person or whether they are likely to be mentally ill. In these studies, the findings vary depending on the label used. A number of studies have asked whether the person in a vignette has a ‘mental illness’ and have found that the person is seen as more dangerous if they are ‘mentally ill’ (Peluso and Blay, 2009; Pescosolido et al., 2007; Phelan and Basow, 2007; Wright and Jorm, 2011). Other studies have examined the effects of more specific labels. In general, when respondents apply the label ‘schizophrenia’ to a vignette they perceive the person as more likely to be dangerous, but not if they apply the label ‘depression’ (Angermeyer and Matschinger, 2003b; Jorm and Griffiths, 2008; Wright and Jorm, 2011).
Causal explanations for mental disorders and belief in dangerousness
It has been argued that promoting biological and genetic explanations of mental disorders to the public might increase stigma and that psychosocial explanations should be promoted instead (Read, 2007; Read et al., 2006). This concern has been particularly raised in relation to belief in dangerousness of people with schizophrenia. While biological and genetic explanations have been contrasted with psychosocial ones, these are not necessarily polar opposites. Factor analytic evidence suggests that public belief in these explanations is largely independent (Furnham and Rees, 1988; Read and Harre, 2001). Indeed, scientific explanations of mental disorders acknowledge the joint importance of biological and psychosocial factors.
There is some evidence that belief in dangerousness is associated with biological explanations of mental disorders
A diverse range of biological explanations have been examined in correlational studies. In a large national survey of the German public, believing that depression or schizophrenia were due to ‘brain disease’ was associated with belief in dangerousness, while belief in ‘heredity’ had a weaker association (Dietrich et al., 2006b). A large national survey of the Australian public found that ‘inherited or genetic’ was associated with belief in dangerousness for schizophrenia, but not for depression (Jorm and Griffiths, 2008). Similarly, US national surveys in 1996 and 2006 found that ‘neurobiological conceptions’ (which were defined as labelling a problem in a vignette as ‘mental illness’ and attributing cause to either a ‘chemical imbalance’ or a ‘genetic problem’) were associated with greater belief in the dangerousness of a person with schizophrenia (Pescosolido et al., 2010). However, for depression, an association was found in 2006 but not in 1996, while for alcohol dependence no association was found in either year.
Other smaller studies have used scales comprising a range of biological beliefs. Two studies on schizophrenia found no association of biological beliefs with belief in dangerousness (Furnham and Rees, 1988; Furnham and Wong, 2007). Other studies have examined associations with ‘endogenous’ causal beliefs about ‘mental illness’, with one study finding an association (Read and Harre, 2001) and another not (Read and Law, 1999).
There has also been one experimental study, where university students were assigned (non-randomly) to view different videos giving either ‘medical’, ‘psychosocial’ or ‘combined’ causal explanations of a person’s psychotic symptoms (Walker and Read, 2002). The medical video was found to increase belief in dangerousness, the combined video to reduce it, while the psychosocial video had no significant effect.
Belief in dangerousness is not associated with psychosocial explanations of mental disorders
A number of correlational studies have examined associations with psychosocial beliefs, including stressful and traumatic events, family factors and sociological factors. None of these studies has found support for the hypothesis that belief in psychosocial factors is associated with less belief in dangerousness, for either schizophrenia (Furnham and Rees, 1988; Furnham and Wong, 2007; Jorm and Griffiths, 2008), mental illness (Read and Harre, 2001) or depression (Jorm and Griffiths, 2008). There have also been two intervention studies. The first study gave university students a series of lectures presenting a psychosocial perspective (Read and Law, 1999). This study produced a decrease in belief in dangerousness, but there was no control group. The second study, reviewed above, compared videos giving various causal explanations (Walker and Read, 2002), but did not find a significant effect of the ‘psychosocial’ video.
Belief in dangerousness is associated with moral explanations of mental disorders, such as weakness or badness of character
A number of studies have examined moral explanations of mental disorders. Belief in dangerousness has been found to be associated with the belief that mental disorders are due to being a ‘failure’, ‘bad deeds’ and lack of ‘willpower and self-discipline’ (Angermeyer and Matschinger, 2004), ‘weakness of character’ (Jorm and Griffiths, 2008), ‘bad character’ (Pirutinsky et al., 2010; Watson et al., 2005a), and the belief that the person is ‘largely to blame for their own condition’ (Chong et al., 2007).
Interventions to reduce belief in dangerousness
Brief interventions involving education or personal contact may produce an immediate reduction in belief in dangerousness, however the quality of the evidence is poor and the longer-term effects are unknown
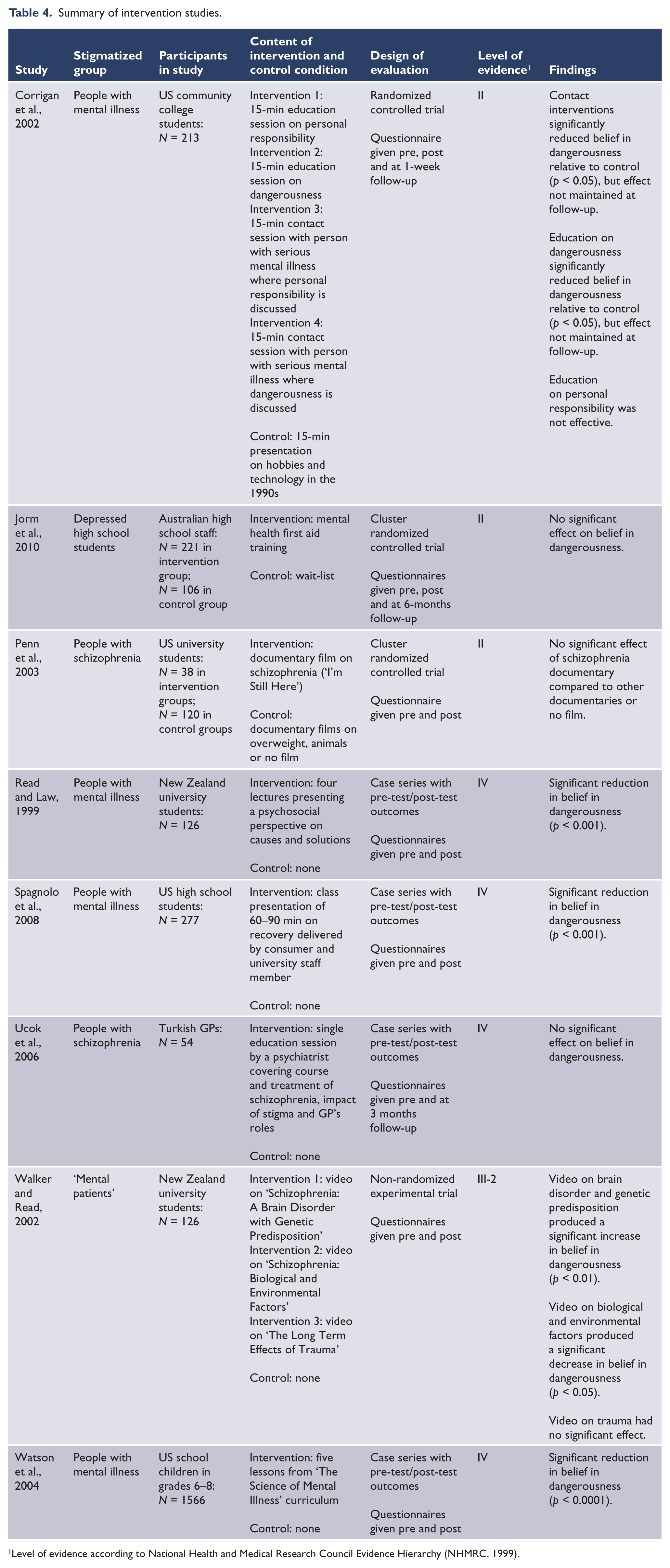
There are eight studies that have evaluated interventions for reducing belief in dangerousness (excluding studies of training programmes for student health professionals, which were reviewed earlier) (Corrigan et al., 2002; Jorm et al., 2010; Penn et al., 2003; Read and Law, 1999; Spagnolo et al., 2008; Ucok et al., 2006; Walker and Read, 2002; Watson et al., 2004). These are summarized in Table 4. Most of these studies have been aimed at changing beliefs about people with mental illness or schizophrenia. The participants in most of these studies have been school, college or university students, with one study on GPs and another on high school staff. The interventions were wide-ranging, but all involved an educational intervention, sometimes with additional consumer contact. Most of the studies did not have high-quality research designs, with only three of the eight studies involving randomized controlled trials and only one examining persistence of effects beyond 1 week. Five of the eight studies showed an immediate reduction in belief in dangerousness, but these mostly had weak designs and there was no evidence of maintenance of effects beyond post-test.
Summary of intervention studies.
Level of evidence according to National Health and Medical Research Council Evidence Hierarchy (NHMRC, 1999).
There is inconsistent evidence on whether belief in dangerousness has changed over time
Given that belief in dangerousness can be changed by various experiences, it is possible that historical changes could occur. Torrey (2011a, b) has argued that deinstitutionalization has increased the proportion of people with severe mental disorders who are untreated, thereby increasing incidents of violence and fuelling stigma. The only evidence on historical changes comes from three studies in the USA and one from Australia. The first study compared the beliefs of sociology students at one university in 1962 and 1971 (Olmsted and Durham, 1976). They found that ratings of dangerousness decreased slightly over time, but this applied equally to ratings of ‘average man’, ‘mental patient’ and ‘ex-mental patient’, with the difference between ‘average man’ and ‘mental patient’ not changing.
The second study compared surveys of the US public carried out in 1950 and 1996 (Phelan et al., 2000). Both surveys asked participants what they understood by the term ‘mentally ill’. Mentions of dangerous behaviour increased from 7.2% to 12.1%. However, this was attributable to changing conceptions of mental illness. Over time, the concept broadened to include a greater range of disorders, with psychosis becoming less prominent. However, for those who did think of mental illness in terms of psychosis, dangerousness was more often part of the description. Unfortunately, this study is limited by the use of the general term ‘mental illness’ and did not directly compare beliefs about dangerousness using case vignettes.
The third study compared surveys of the US public in 1996 and 2006 on attitudes to vignettes portraying schizophrenia, major depression and alcohol dependence (Pescosolido et al., 2010; Silton et al., 2011). No changes in beliefs about dangerousness were found.
The Australian study compared the beliefs of adults in 2003/4 and 2011 (Reavley and Jorm, in press). Over this period, belief in dangerousness increased for both schizophrenia and depression. There was no clear explanation for this increase.
Belief in dangerousness and help-seeking
Belief in dangerousness may motivate professional help-seeking for mental disorders
The literature on belief in dangerousness overwhelmingly regards this as a negative characteristic. However, belief in dangerousness may sometimes motivate a person to seek professional help. A survey of adults in the European Union found that personal belief in dangerousness, as well as living in a region where belief in dangerousness was more prevalent, was associated with greater willingness to seek professional help (Mojtabai, 2010). Similarly, in Australia it has been found that young adults who believe in dangerousness are more likely to intend to seek help if they are affected by a mental disorder and more likely to say that they would seek help specifically from a psychiatrist (Yap et al., 2010). Australian young people who believe in dangerousness are also more likely to assist someone else with a mental disorder by making an appointment for that person to see a doctor (Yap and Jorm, 2011).
Discussion
Belief in dangerousness does have some objective basis, with increased risk of dangerous behaviour across a range of mental disorders. To reduce this risk requires improvements in services and greater provision of early intervention. On the other hand, most people affected by mental disorders are not dangerous. The perception of dangerousness by the public exceeds the evidence and is not generally based on personal experience of dangerous behaviour. Indeed, members of the public who have had personal contact and mental health professionals are less likely to believe in dangerousness than the general public.
The excessive belief in dangerousness must therefore be influenced by other factors. The media is the most obvious source and there is some evidence that reports of rare extreme events can have a negative influence. Counter-balancing such reports, there is a general belief that treatment reduces risk of dangerousness. There might therefore be merit in considering guidelines on media reporting of violence by mentally ill people, analogous to existing guidelines on media reporting of suicide (Commonwealth of Australia, 2011; Pirkis et al., 2006), giving advice on how to report such events without fuelling unnecessary fear. For example, one approach might be to note any lack of treatment and to give information that treatment reduces risk.
This review has revealed a number of inadequacies in this literature. Finding effective interventions that reduce belief in dangerousness is arguably the greatest priority, but the quality of the existing evidence is poor. Very few studies involved randomized controlled trials and even fewer investigated whether any effects were maintained over time.
Another limitation involves the exclusive reliance on attitudinal measures taken in relation to labels like ‘mentally ill’ or case vignettes. Labels and vignettes are decontextualized and may not relate to attitudes to a real person with a mental illness that someone interacts with in daily life. Attitude questions are convenient to administer, but we do not know whether the attitudes translate into discriminatory behaviour or whether consumers and carers are affected adversely by these attitudes. There is also need for a focus on the potential benefits of belief in dangerousness (e.g. for getting people into treatment), in addition to the negative effects on discrimination.
Given the potential importance of stigma for the lives of people affected by mental disorders, there needs to be serious consideration to setting national goals in this area and routinely monitoring components of stigma in population surveys.
Footnotes
Funding
This research was supported by an NHMRC Australia Fellowship.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.