
Abstract
Objective:
‘Mental illness’ is a common label. However, the general public may or may not consider various conditions, ranging from major psychiatric disorders to stress, as mental illnesses. It is unclear how such public views affect attitudes towards people with mental illness and reactions to one’s own potential mental illness, e.g. in terms of help-seeking or disclosure.
Methods:
In representative English population surveys the classification of six conditions (schizophrenia, bipolar disorder, depression, drug addiction, stress, grief) as a mental illness was assessed as well as attitudes towards, and contact with, people with mental illness, intentions to disclose a mental illness and to seek treatment.
Results:
A factor analysis of how strongly respondents perceived the six conditions as a mental illness yielded two factors: (i) major psychiatric disorders and (ii) stress- and behaviour-related conditions including drug addiction. In regression analyses, higher scores on the first, but not the second, factor predicted less perceived responsibility of people with mental illness for their actions, and more support for a neurobiological illness model and help-seeking. Classifying stress-related/behaviour-related conditions as mental illnesses, as well as not referring to major psychiatric disorders as mental illnesses, was associated with more negative attitudes and increased social distance, but also with stronger intentions to disclose a mental illness to an employer. Negative attitudes and social distance were also related to ethnic minority status and lower social grade.
Conclusions:
Referring to major psychiatric disorders as mental illnesses may reflect higher mental health literacy, better attitudes towards people with mental illness and help-seeking. A broader concept of mental illness could, although increasing negative attitudes, facilitate disclosure in the workplace. Public views on what is a mental illness may have context-dependent effects and should be taken into account in anti-stigma campaigns.
Introduction
What is a ‘mental illness’? Current psychiatric classifications describe hundreds of conditions as mental illnesses, but the concept remains fuzzy in the public mind. The difficulty with defining mental illness has long been alluded to by philosophers (Bolton, 2008) and sociologists alike (Link and Phelan, 2001). Still, the label ‘mental illness’ is commonly used and whether members of the public think certain conditions are or are not a mental illness is determined less by scientific classification systems than by personal views and sociocultural trends (Jaspers, 1997).
Qualitative researchers have long pointed out that an individuals’ idiosyncratic views of a condition are crucial to how they will react towards others with the condition or to falling ill themselves (Hahn, 1995; Weiss, 2001). These views have consequences. Whether the public tends to label certain conditions such as schizophrenia, drug addiction or stress a ‘mental illness’ may have beneficial or harmful effects, both for public attitudes towards people with mental illness (Link et al., 1999) and for persons with mental illness and how they react to their condition (Rose and Thornicroft, 2010). As far as its positive consequences are concerned, an illness label can carry important information and facilitate help-seeking and communication between people with mental illness and mental health service professionals (Wright et al., 2007). Jorm and colleagues (2006a) use the term mental health literacy, referring to the recognition of mental illnesses and knowledge about symptoms and available treatments. Improved mental health literacy over time was associated with stronger intentions to seek appropriate help (Jorm et al., 2006b). On the other hand, the label of mental illness can have negative effects. With respect to public attitudes, labelling of an initially unlabelled psychiatric case vignette was associated with increased desire for social distance and with less perceived responsibility of people with mental illness for their condition (Angermeyer and Matschinger, 2005). Among people with mental illness, labels can increase the expectation and experience to be discriminated against by others and individuals with mental illness may not seek help in order to avoid the label (Corrigan and Rüsch, 2002; Rüsch et al., 2009). Labels can also induce self-stigma if individuals with mental illness agree with negative stereotypes associated with the label (Ben-Zeev et al., 2010; Rose and Thornicroft, 2010).
Research on effects of labelling has mainly used vignettes, describing persons with mental illness with or without the label of mental illness or a specific diagnosis attached. With this method, the recognition of symptom patterns as a mental illness has been used to evaluate knowledge or mental health literacy, and the effects of labels on attitudes and behaviour have been examined. It is, however, less clear which specific conditions the public associates with the generic term ‘mental illness’ and how public views about whether or not certain conditions are a mental illness shape reactions towards others with a mental illness and towards one’s own potential mental illness. From a medical perspective, major psychiatric disorders such as schizophrenia or depression, as well as drug addiction, are classified as mental illnesses. Reactions to external stressors, e.g. adjustment disorders, have also been included in diagnostic manuals. The public may have a different perspective, though. In a US survey (Link et al., 1999), when prompted by an interviewer, the vast majority of respondents labelled subjects described in a vignette as having specific disorders (e.g. 98% for alcohol dependence, 95% for major depression, 85% for schizophrenia). However, fewer respondents considered it somewhat or very likely that these conditions were mental illnesses (88% for schizophrenia, 69% for major depression, 49% for alcohol and 44% for cocaine dependence). Likewise members of the public who correctly identified case vignettes of children with mental health problems as cases of depression or attention-deficit hyperactivity disorder in part rejected the mental illness label (Pescosolido et al., 2008). Labelling these conditions as mental illnesses was associated with stronger intentions to seek help, but also with greater perceived dangerousness (Pescosolido et al., 2007). From the perspective of people with mental illness, in qualitative studies some participants with depression rejected the mental illness label not only because they expected discrimination as its consequence, but also because they considered their symptoms a normal reaction to life stressors (Wittkampf et al., 2008). On the other hand, some welcomed the label because they preferred that their condition was recognised as a ‘real’ illness (Barney et al., 2009).
Thus the public does not necessarily refer to major psychiatric disorders as mental illnesses. On the other hand, conditions such as stress may be considered a mental illness. These public views are crucial for our understanding of how the label ‘mental illness’ can shape behaviours, a vital piece of the puzzle for future anti-stigma campaigns (Evans-Lacko et al., 2012). Current campaigns in part focus on specific disorders, e.g. schizophrenia in the World Psychiatric Association’s campaign (www.openthedoors.com), but more frequently attempt to improve knowledge, attitudes and behaviours towards people with mental illness in general (e.g. Time to Change in England; Evans-Lacko et al., 2010; Henderson and Thornicroft, 2009). When the target of such efforts is ‘mental illness’, we need to know what is seen as a mental illness by the public. This study’s aim is not to contribute to ongoing discussions about psychiatric classification systems, but rather to determine empirically at a population level public views and their consequences. Our aim was three-fold: first, to determine patterns in the way the public classifies conditions as mental illnesses; second, to examine the effects of these patterns on public attitudes towards others with mental illness; and third, to assess the link between views on what is a mental illness and reactions towards one’s own potential mental illness.
Using data from a large nationally representative English population survey, we therefore set out to examine the degree to which members of the general public view major psychiatric disorders (schizophrenia, bipolar disorder, depression), drug addiction and stress-related conditions (stress, grief) as a mental illness, expecting the ways different conditions are seen as a mental illness to fall into different clusters. We then analysed the association of public views on what is a mental illness with (i) two key attributions, diminished responsibility of people with mental illness for their actions and a neurobiological illness model; (ii) sociodemographic characteristics; (iii) attitudes towards others with a mental illness; and (iv) reactions to one’s own potential mental illness in terms of disclosure and help-seeking.
Methods
Participants
Survey data from 3496 adults across England were obtained from the Department of Health, UK (www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4079110). The survey was conducted by Taylor Nelson Sofres plc in January 2009 (n = 1751) and January 2010 (n = 1745) as part of the Omnibus Survey, following similar surveys from 1994 onwards, and was carried out using a quota sample, with sample points selected by a random location methodology. Survey methods were identical in 2009 and 2010. Census small area statistics and the Postcode Address File were used to define sample points which were stratified by Government Office Region and social grade (for sample characteristics see Table 1; for definition of social grade see Table 1, footnote a). Interviews were carried out in the participant’s home by fully trained personnel using computer-assisted personal interviewing and demographic information was collected at the end of the interview. Data were weighted for gender and social grade to match the general population, and sampling weights were used in the regression analyses.
Unweighted sample characteristics (n = 3496, before weighting).
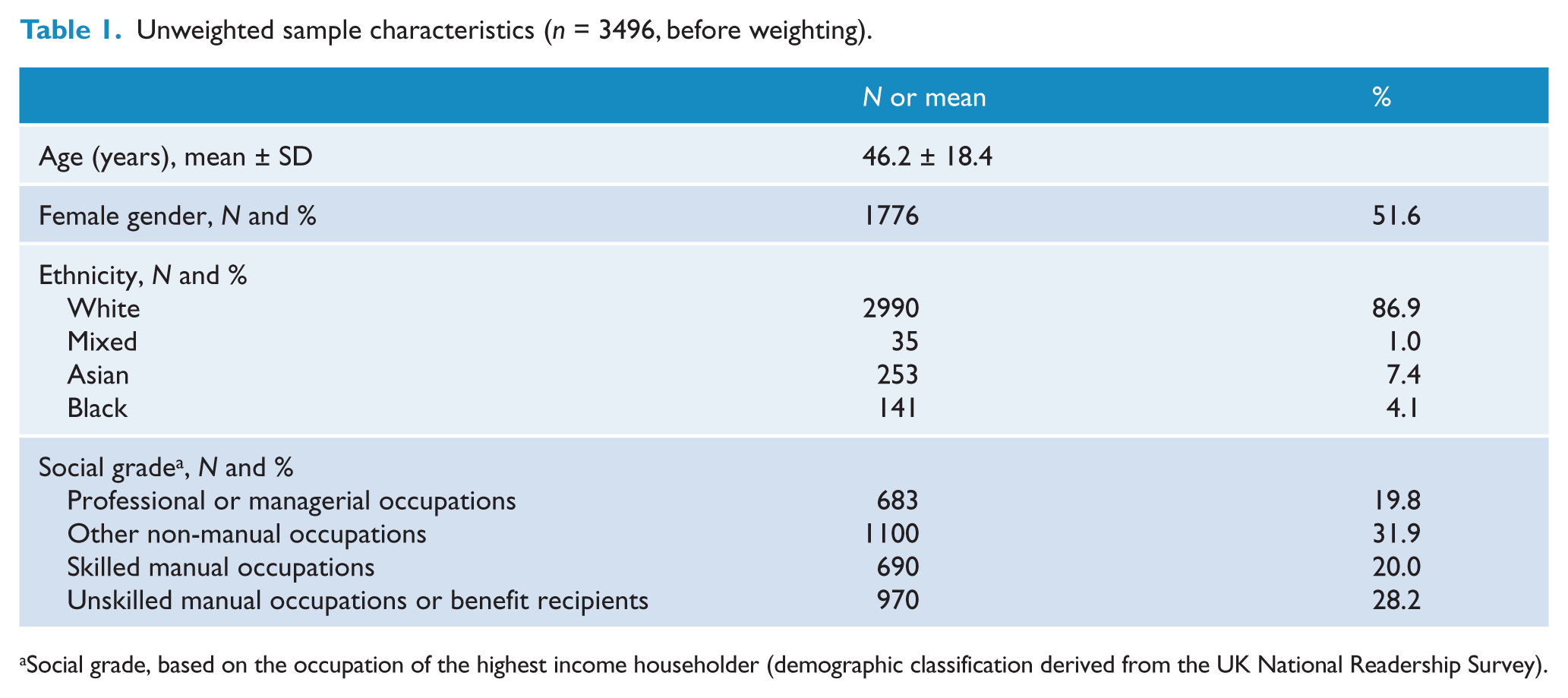
Social grade, based on the occupation of the highest income householder (demographic classification derived from the UK National Readership Survey).
Measures
Classification as ‘mental illness’
To assess the degree to which six conditions were considered a mental illness by the public, participants were asked, ‘Please say to what extent you agree or disagree that each of the following conditions is a type of mental illness’. No case vignettes or other information was added, participants just responded to the following labels; six conditions were rated from 1 (disagree strongly) to 5 (agree strongly): depression (M = 4.2, SD = 1.0), stress (M = 3.4, SD = 1.4), schizophrenia (M = 4.6, SD = 0.7), bipolar disorder (manic depression) (M = 4.5, SD = 0.8), drug addiction (M = 3.0, SD = 1.5), grief (M = 3.1, SD = 1.4). Two other items, both rated 1 (yes) or 0 (no), examined whether participants thought people with mental illness were characterised by lacking responsibility for their actions and by being born with a brain abnormality (see Table 3 for item wording).
Rates of agreement with six conditions being a mental illness a and exploratory factor analysis (yielding two factors with eigenvalues > 1). Loadings, following varimax rotation, presented at the top and factor characteristics at the bottom.
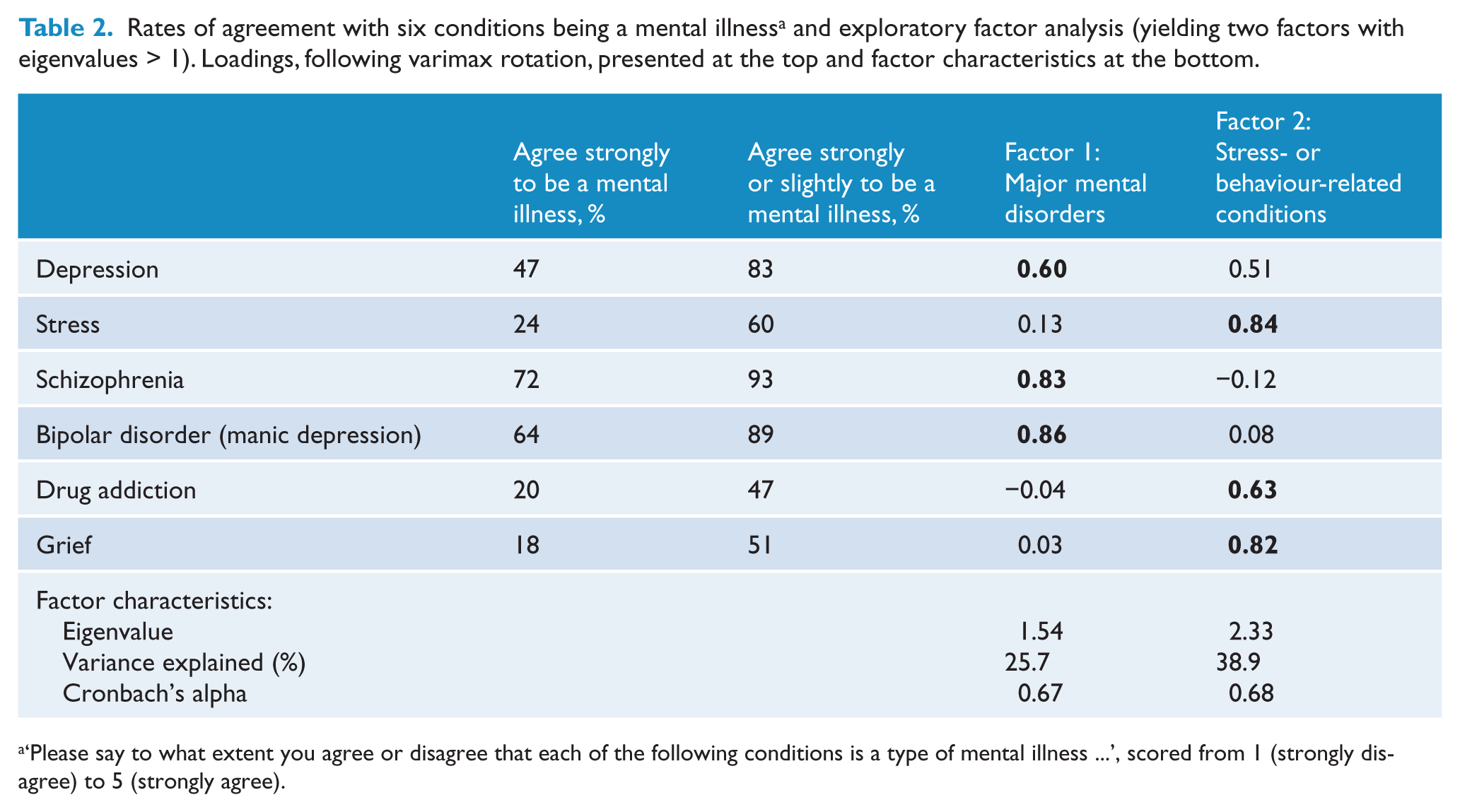
‘Please say to what extent you agree or disagree that each of the following conditions is a type of mental illness …’, scored from 1 (strongly disagree) to 5 (strongly agree).
Predictors of two illness attributes: perceived responsibility and neurobiological model of mental illness (logistic regressions).
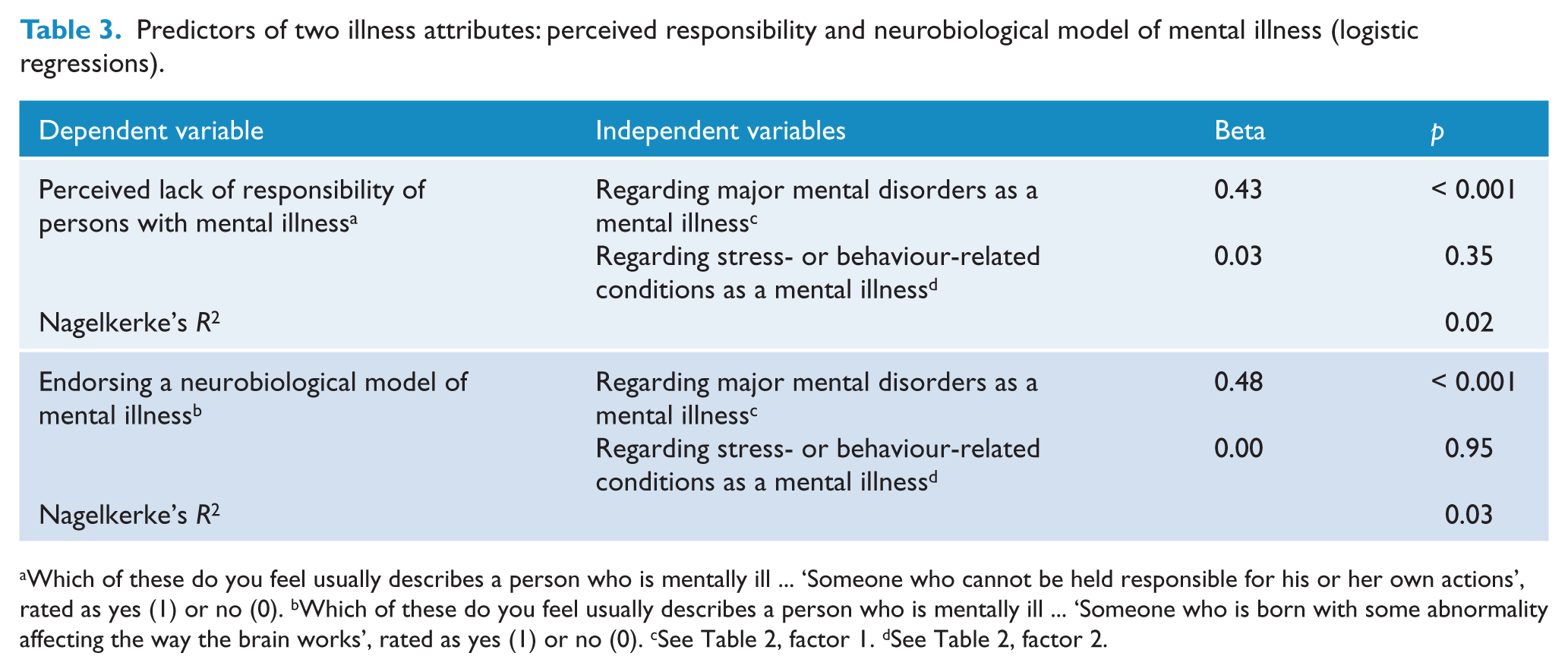
Which of these do you feel usually describes a person who is mentally ill … ‘Someone who cannot be held responsible for his or her own actions’, rated as yes (1) or no (0). bWhich of these do you feel usually describes a person who is mentally ill … ‘Someone who is born with some abnormality affecting the way the brain works’, rated as yes (1) or no (0). cSee Table 2, factor 1. dSee Table 2, factor 2.
Disclosure and help-seeking
Whether participants felt comfortable to disclose a mental illness to friends or relatives was measured by one item (‘In general, how comfortable would you feel talking to a friend or family member about your mental health, for example telling them you have a mental health diagnosis and how it affects you?’; M = 5.1, SD = 1.9) and the readiness to disclose to an employer by one item (‘In general, how comfortable would you feel talking to a current or prospective employer about your mental health, for example telling them you have a mental health diagnosis and how it affects you?’; M = 3.7, SD = 2.1), both scored from 1 to 7 and higher scores reflecting greater comfort to disclose. The latter disclosure item was available only in the 2010 survey data (n = 1745). Intentions to seek help from a GP was assessed by one item (‘If you felt that you had a mental health problem, how likely would you be to go to your GP for help?), rated on a 1-to-5 Likert scale with higher scores indicating greater likelihood to seek help (M = 4.2, SD = 1.1).
Attitudes
The Department of Health Attitudes to Mental Illness questionnaire was developed in 1993 based on previous research in Toronto and the West Midlands. It includes 26 items from the 40-item Community Attitudes toward the Mentally Ill scales (CAMI; Taylor and Dear, 1981) and an added item on employment-related attitudes. Items refer to attitudes about social exclusion, benevolence, tolerance and support for community mental health care (for item wording see Rüsch et al., 2011) and were rated from 1 (strong disagreement) to 5 (strong agreement). A two-factor structure has been established for this scale (Rüsch et al., 2011), yielding one factor and mean score for prejudice and exclusion (in this sample M = 2.1, SD = 0.7; Cronbach’s alpha 0.84) and one for tolerance and support for community care (in this sample M = 4.0, SD = 0.5; Cronbach’s alpha 0.78).
Contact with people with mental illness
The level of past or present as well as intended future contact with people with mental illness was measured using the Reported and Intended Behaviour Scale (RIBS; Evans-Lacko et al., 2011). Its first subscale includes four items about current or past contact in the context of living or working together or having a person with mental illness as a neighbour or friend (e.g. ‘Are you currently living with, or have you ever lived with, someone with a mental health problem?’). Participants rated each item as yes, no or don’t know. Responses were dichotomised (yes = 1; no or don’t know = 0), yielding an average score between 0 and 1 with higher scores representing more past or present contact (in this sample Kuder-Richardson formula 20 = 0.60; M = 0.25, SD = 0.29). The RIBS’s second subscale measures intentions to have contact using four items (e.g. ‘In the future, I would be willing to live with someone with a mental health problem’). Items were rated on a 1-to-5 Likert scale from strong disagreement to strong agreement, with higher average scores reflecting stronger agreement (in this sample Cronbach’s alpha = 0.58; M = 4.0, SD = 0.9).
Statistics
Using six items on the classification of conditions as a mental illness, we set out to identify internally consistent factors that could be used as independent variables in the regressions on attitudes, contact, disclosure and help-seeking. For that purpose we performed an exploratory factor analysis of the six items, using principal component analysis and varimax rotation in SPSS 17.0. The resulting factors were based on the correlation structure of responses to whether the above-mentioned conditions were perceived as a mental illness. Using STATA9.2 and sampling weights, we then ran linear regressions on attitudes, contact, disclosure and help-seeking intentions; and logistic regression on perceived responsibility and neurobiological model of mental illness. Following a Bonferroni correction, only findings at the p < 0.005 level were considered significant in the ten regression analyses.
Results
Patterns of classifying conditions as a ‘mental illness’
Between two-thirds and half of respondents agreed strongly that schizophrenia and bipolar disorder or depression, respectively, are mental illnesses, while less than a quarter believed strongly that drug addiction, stress or grief are mental illnesses (Table 2). Including rates of slight agreement, agreement rates for the latter three conditions to be mental illnesses increased to about 50%, whereas a large majority of respondents slightly or strongly agreed that schizophrenia, bipolar disorder and depression are mental illnesses.
Determining patterns of classification as a mental illness, the above-mentioned factor analysis yielded two factors with eigenvalues greater than one (Table 2). Agreement with three major psychiatric disorders being a mental illness (schizophrenia, bipolar disorder, depression) loaded on factor 1, while the classification of three stress- or behaviour-related conditions (stress, grief, drug addiction) as mental illnesses loaded on factor 2. Mean scores of agreement that the conditions are mental illnesses were significantly higher for factor 1 (M = 4.4, SD = 0.7) than for factor 2 (M = 3.2, SD = 1.1; T = 63.2, p < 0.001). Both subscale scores were only weakly correlated (r = 0.28, p < 0.001) and accounted for a cumulative variance of 64.6%. The Kaiser-Meyer-Olkin measure of 0.67 suggested satisfactory sampling adequacy, and a significant Bartlett’s test of sphericity indicated that a factor model was appropriate (approximate chi-square = 4162.98, df = 15, p < 0.001).
Illness attributes and demographics associated with classifications
To examine how classifying conditions as a mental illness influenced two illness attributes (e.g. perceived responsibility of people with mental illness for their actions; neurobiological illness model), we ran two logistic regressions (Table 3). Stronger agreement that major psychiatric disorders are mental illnesses was associated with less perceived responsibility and a more neurobiological model. Considering stress-related/behaviour-related conditions a mental illness was not associated with either attribute.
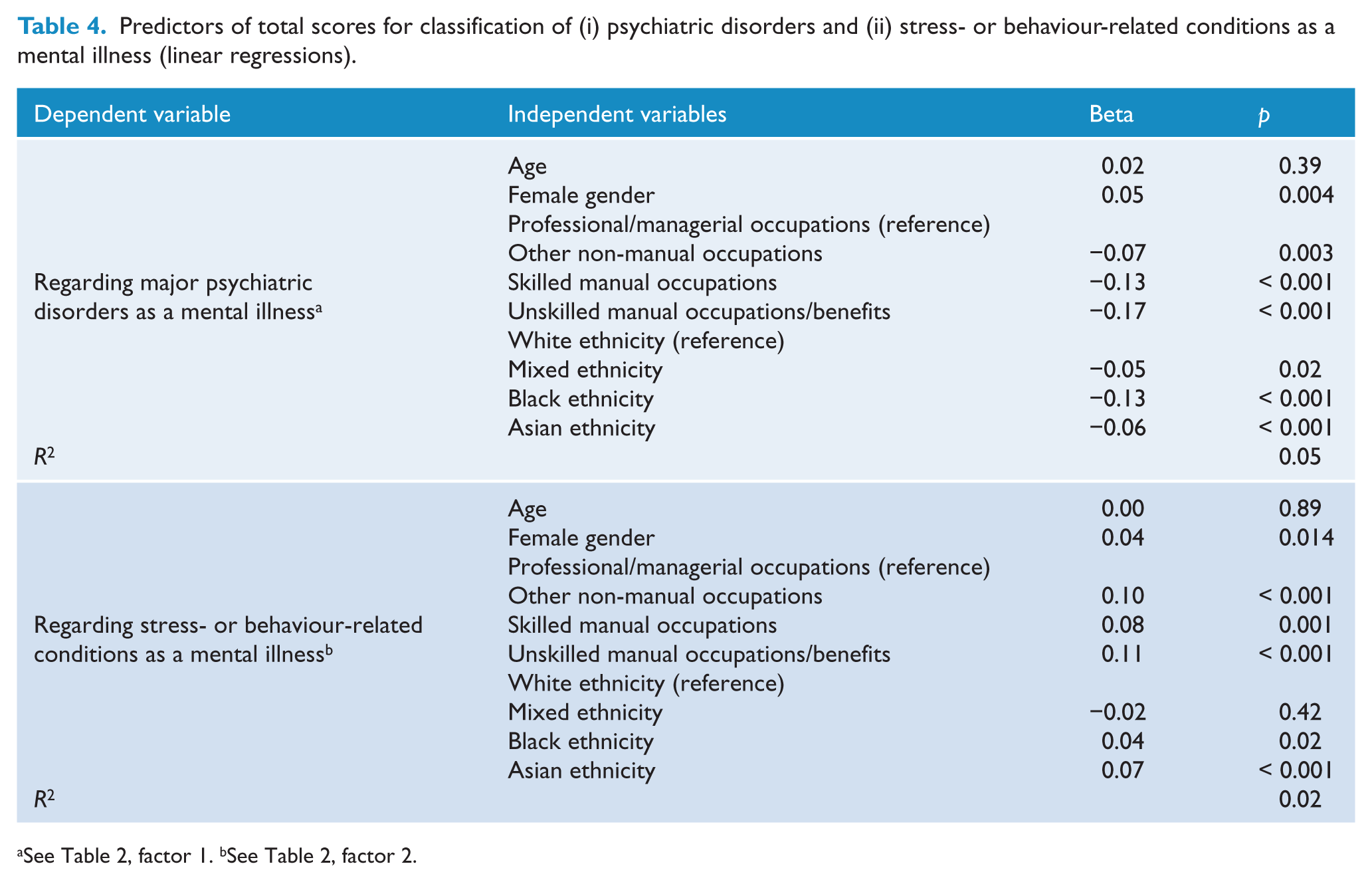
In two linear regressions we examined sociodemographic variables as predictors of the classification of conditions as mental illnesses (Table 4). Referring to major psychiatric disorders as mental illnesses was associated with female gender, higher social grade and white ethnicity. A stronger tendency to regard stress-related/behaviour-related conditions as mental illnesses, on the other hand, was predicted by lower social grade and Asian ethnicity.
Predictors of total scores for classification of (i) psychiatric disorders and (ii) stress- or behaviour-related conditions as a mental illness (linear regressions).
Classification of mental illness as predictor of attitudes, disclosure and help-seeking
We tested the influence of classification patterns in a series of multiple linear regressions, controlling for sociodemographic factors and past and present contact with people with mental illness. The tendency to classify (i) major mental disorders and (ii) stress-related/behaviour-related conditions as mental illnesses were independent variables (Table 5). Negative attitudes towards people with mental illness and reduced desire for future social contact were predicted by more disagreement that major psychiatric disorders are mental illnesses and by a tendency to classify stress-related/behaviour-related conditions as mental illnesses. Positive attitudes were associated with classifying major disorders as mental illnesses. In terms of disclosure, not considering major psychiatric disorders as mental illnesses and a higher tendency to view stress-related/behaviour-related conditions as mental illnesses predicted stronger intentions to disclose a mental illness to employers, but not to friends and family. Help-seeking intentions from a GP were associated with considering major psychiatric disorders as mental illnesses.
Regressions on attitudes, contact, disclosure and help-seeking intentions.
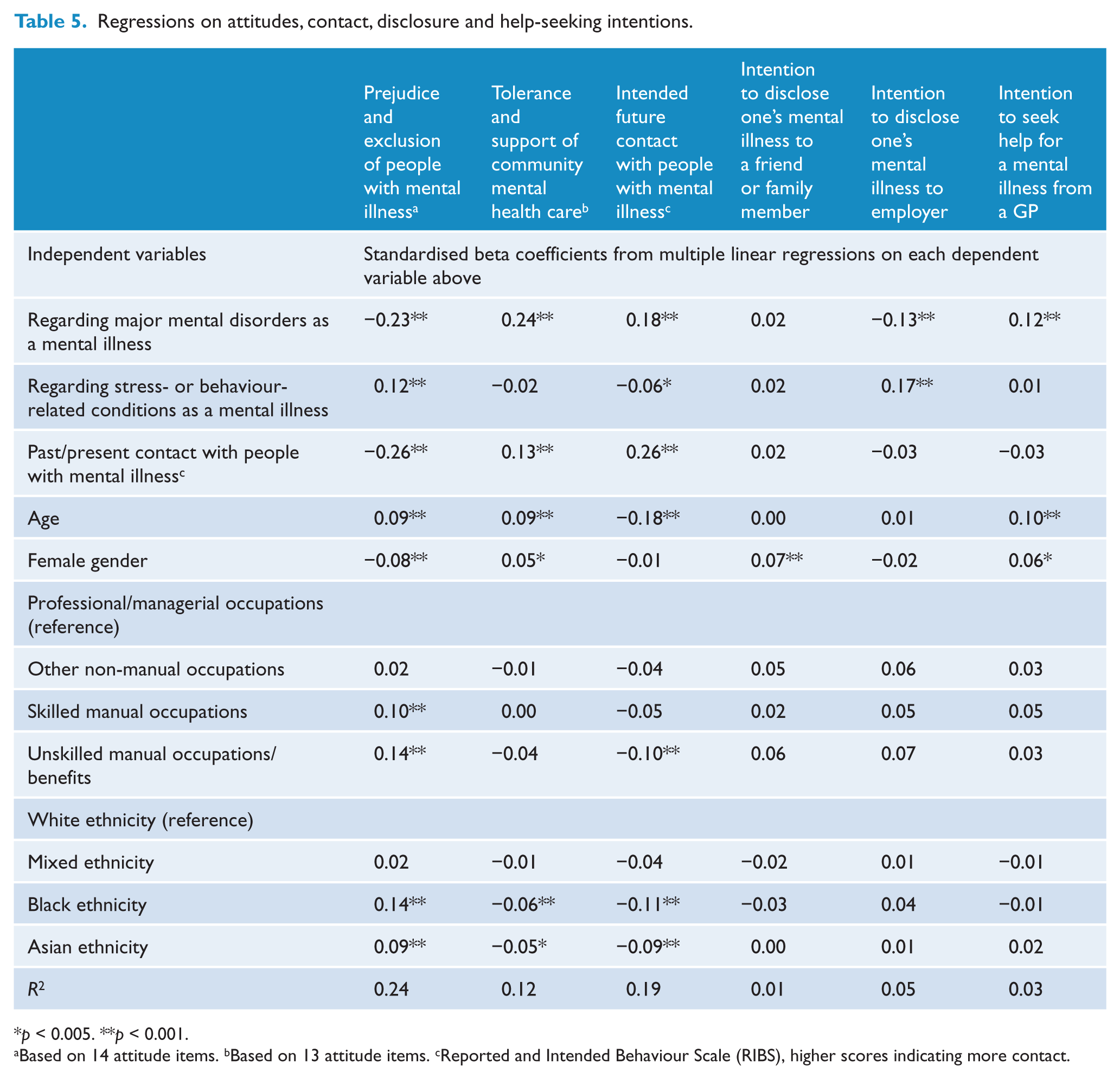
p < 0.005. **p < 0.001.
Based on 14 attitude items. bBased on 13 attitude items. cReported and Intended Behaviour Scale (RIBS), higher scores indicating more contact.
Discussion
Whether members of the general public associate certain conditions with the label ‘mental illness’ shapes their actions and reactions, both to others with a mental illness and to a potential own mental illness. We found evidence for a two-factor model of public views about which conditions are a mental illness: on the one hand the classification of major psychiatric disorders as a mental illness; on the other hand the view of drug addiction and external stressors as a mental illness, suggesting a broader and less specific concept of mental illness. The endorsement of both views was only weakly positively correlated. This is consistent with previous research on the broadening of public conceptualisations of mental illness over time (Phelan et al., 2000) and could reflect two cultural meanings of ‘mental illness’, one being more medical and the other representing a broader and partly more pejorative view (Olafsdottir and Pescosolido, 2009).
As far as attitudes towards others with a mental illness are concerned, stronger classification of psychiatric disorders as mental illnesses predicted more positive attitudes. We could speculate that considering major psychiatric disorders as mental illnesses is an, if incomplete, proxy of mental health literacy. Then it would be consistent with the concept of stigmatising attitudes as reflecting biased stereotypes or ignorance (Thornicroft, 2006) and with findings that increased mental health literacy and correct labelling leads to more positive attitudes (Griffiths et al., 2004; Kitchener and Jorm, 2006; Wright et al., 2011a).
A different picture emerged for the association between views on what is a mental illness and reactions to a potential own mental illness. Whether or not to disclose one’s own mental illness to others is often a critical decision for individuals with mental illness (Corrigan and Matthews, 2003). Coming out carries the risk of discrimination, but may end secrecy, reduce self-stigma and open new sources of social support (Corrigan et al., 2010). Our results suggest that the context matters for whether personal views on what is a mental illness influence disclosure intentions. In a workplace context, but not among friends and family, a broader and less ‘psychiatric’ understanding of what a mental illness is predicted stronger intentions to disclose a mental illness. Possibly the more people consider major psychiatric disorders a mental illness, the more they fear adverse consequences when disclosing their mental illness at work (Corrigan et al., 2012). To see stress-related conditions as a mental illness could facilitate disclosure in the workplace, possibly because they are seen as more common and transitory. Rejection by friends and family may seem less likely and other factors, such as the quality of the relationship with them, may be more relevant, overriding the importance of one’s view of what a mental illness is.
In line with previous research (Jorm et al., 2006b; Rüsch et al., 2011; Wright et al., 2011b), classifying major psychiatric disorders as illnesses predicted stronger intentions to seek professional help. This is plausible, because recognition of a condition as an illness is often the first step towards care-seeking (Wright et al., 2007). Not referring to major psychiatric disorders as illnesses was related to more perceived responsibility or blame and to a less neurobiological illness model. Previous research found that higher perceived responsibility was related to increased fear and anger and reduced pity (Corrigan et al., 2003). This could in part explain why in our study weaker classification of psychiatric disorders as illnesses predicted more negative attitudes. That considering major psychiatric disorders as illnesses was associated with a neurobiological model of illness may in part be explained by the increasing popularity of such illness concepts (Pescosolido et al., 2010; Read et al., 2006; Schnittker, 2008). Several studies have found that in particular genetic models predict more negative attitudes (Phelan et al., 2006), including implicit self-blame among people with mental illness (Rüsch et al., 2010). These negative effects are less clear for the view of mental illness as a brain disease which may have mixed effects, possibly decreasing perceived responsibility and blame while increasing perceived dangerousness (Corrigan and Watson, 2004). The fact that weaker classification of major psychiatric disorders as a mental illness and support for a broader view of what is a mental illness was associated with lower social grade and ethnic minority status may reflect reduced access to information or different cultural perceptions of illness.
Limitations of our study need to be considered. First of all, our data did not provide information on why members of the public agreed or disagreed with the six conditions being a mental illness and how they would have classified other conditions than the six in the survey; the use of open-ended questions or unlabelled case vignettes should be included in future studies. While we could examine the link between the factor structure of classifying the six conditions and the link to perceived responsibility and a neurobiological model of mental illness, the association between other attributes, such as dangerousness, and other illness models with the classification of conditions needs to be studied in future research. Second, there was some terminological variance in the survey. While attitude, classification and attribution measures referred to ‘mental illness’, help-seeking, disclosure and contact measures used the terms ‘mental health problems’ or ‘mental health diagnosis’. The latter terms are often used as broader terms in survey research, but future studies should aim to avoid such terminological variations. Third, information on the level of psychopathology as well as previous contact with health services among respondents was unavailable. Only one example of help-seeking intentions was measured and future studies should distinguish various types of service use, including non-professional support. Fourth, it is unclear how closely intentions to seek help or to disclose are related to actual behaviour. Finally, the variance explained by our regression models was small. Other predictors were not accounted for and therefore future studies should include psychopathology, perceived quality and accessibility of services, experiences with health care and, particularly as predictors of disclosure, personality variables such as rejection sensitivity and motivational goals.
Despite these limitations, our results have implications for anti-stigma initiatives. Internationally many campaigns are under way (Sartorius and Schulze, 2005), some of which focus on the stigma associated with a particular mental illness, e.g. schizophrenia, others on mental illness stigma in general (Rüsch et al., 2005). Our results suggest that what is considered a mental illness by the public cannot be taken for granted, and this has consequences for anti-stigma initiatives. First, programmes focusing on a single condition need to decide whether or not to frame the condition as a mental illness or to use another label, e.g. ‘health condition’. Some hope that the latter approach will reduce the activation of negative stereotypes such as dangerousness that are associated with ‘mental illness’ (Barney et al., 2009). This may be the case, but such subtyping of people with mental illness (in people with serious mental illnesses versus those with ‘health conditions’) could possibly worsen attitudes towards others with conditions perceived to be more serious such as schizophrenia. It may also negatively affect self-stigma among people with more serious disorders. The approach would then be unhelpful to achieve fundamental social change and reduce discrimination against people with any mental illness. At least these kinds of potential unintended side effects of relabelling and subtyping need to be examined empirically.
Second, anti-stigma initiatives which address mental illness stigma in general should define their view of what is a mental illness, compare it to public views and decide whether or not they want to change public views. Increased labelling of major psychiatric disorders as mental illnesses may improve both attitudes and help-seeking intentions. However, a broader view of mental illness that includes conditions such as stress seems to have mixed effects. Therefore it is an empirical question for future research whether broader illness concepts of anti-stigma campaigns are harmful or helpful.
Several researchers have suggested that the normalisation of psychiatric symptoms will reduce stigma (Kingdon and Turkington, 1991), which is plausible because it reduces the perceived categorical difference between people with versus without mental illness (Link and Phelan, 2001). However, a broader view of the public on what is a mental illness may lump together conditions such as stress with more stigmatised behaviours such as drug use (Schomerus et al., 2011), which could in part explain the link between this broader view and more negative attitudes in our study. Disclosure, on the other hand, may be helpful for individuals with mental illness (Corrigan et al., 2010) and supported by a broader concept. Finally, because sociodemographic and ethnic variables were in part associated with attitudes and intended behaviours, initiatives to improve knowledge and attitudes might be tailored for specific population subgroups.
In conclusion, we found evidence of patterns in how the general public categorises various conditions as mental illnesses and how these perceptions predict both attitudes towards individuals with a mental illness and reactions to a potential own illness. Future anti-stigma campaigns should reflect what the public considers a mental illness in the first place. We also need to examine empirically whether addressing the stigma of mental illness in general versus the stigma associated with a particular psychiatric disorder is more effective at reducing prejudice and discrimination against people with mental illness and to facilitate behaviours such as help-seeking and disclosure among members of the public and people with mental illness alike.
Footnotes
Funding
This study was funded in relation to a National Institute for Health Research (NIHR) Applied Programme grant awarded to the South London and Maudsley NHS Foundation Trust (GT), and in relation to the NIHR Specialist Mental Health Biomedical Research Centre at the Institute of Psychiatry, King’s College London, and the South London and Maudsley NHS Foundation Trust (GT).
Declaration of interest
The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. All authors declare that they have no conflict of interest.