
Abstract
Stigma is accepted as the most important obstacle to the appropriate treatment and rehabilitation of those suffering from mental illness [1]. The community has been regarded as the most appropriate basis for the development of mental health programmes and studies have shown that the community attitude to mental illness and its treatment is a vital prerequisite to the realization of successful anti-stigma programmes [2], [3].
Although it is clear that stigma is common, there are conflicting reports on the correlates of stigmatizing attitudes towards mental illness. While the explanatory power of sociodemographic variables is quite poor, there seemed to be a positive association between familiarity with mental illness and the acceptance of people with mental illness [4]. Most studies have concluded that stigmatizing attitudes towards mental illness are strongly correlated with views about causation [5–7], and with the belief that the mentally ill are dangerous and violent [8] and the view that mental illness is chronic, difficult to treat and has a poor prognosis [9]. Although earlier studies had claimed that stigmatizing attitude towards the mentally ill is less evident in non-Western culture [10], recent studies in sub-Saharan Africa have suggested that stigmatizing attitudes may be common [11–13]. Unfortunately there is still a paucity of research on mental illness stigma in sub-Saharan Africa. The available studies had been limited by small sample size, narrowed scope and hospital-based sampling. Prior to embarking on an active anti-stigma programme in the region, the attitude of the community and its associated factors should be estimated.
Next to loss of status or discreditation, social distance represents the most significant aspect of stigmatization [8]. The aim of the present study was to assess the public attitude (social distance) towards people with mental illness in southwestern Nigeria and examine the factors correlating with such attitudes.
Methods
Participants and sampling technique
Participants were selected though a multistaged probability sampling technique from three selected communities in Nigeria (urban; semi-urban; rural). The selected communities conformed to the classification in the 1991 population census in Nigeria [14]. The first stage consisted of random selection of seven enumeration areas from each of the three communities. The enumeration areas are geographical units demarcated by the National Population Commission, with each area consisting of approximately 100–120 household units. The second stage involved enumeration of the houses in each area. When more than one household member was found in a house, one household was selected by balloting. The third stage involved the selection of one adult (above 18 years) from each household for the interview. From this a total of 2342 participants were targeted for the interview.
Instruments
The participants completed a semi-structured questionnaire enquiring about the following.
Sociodemographic data
Information on age, sex, marital status, religion, ethnicity, highest education obtained and occupation, were obtained.
Familiarity with mental illness
The participants were asked whether they had ever had any contact or ever cared for the mentally ill and whether he/she had a family member/friend who has or has had mental illness.
Causal attribution
Respondents’ attributions of the possible causal factors of mental illness were assessed by responses to a nine-item questionnaire detailing possible causes of mental illness. The causes included psychosocial factors (substance and alcohol misuse, life stresses, personal deficit or failure/lack of willpower), supernatural factors (witchcraft/sorcery/evil spirits, God's will/divine punishment, destiny/bad luck) and biological factors (heredity, brain injury, contact with mentally ill/childbirth). Using a 4-point Likert scale (‘not a cause’, ‘rarely a cause’, ‘likely a cause’ and ‘definitely a cause’), the respondents were asked to indicate how relevant they considered each potential cause to be. Responses of ‘likely a cause’ and ‘definitely a cause’ were counted as endorsing a cause. For clearer presentation, the average endorsement on each group was computed and, based on this, participants endorsing more than the mean (+2SD) for each group were regarded as significantly endorsing the causal group. This led to endorsement of more than one item in a group being regarded as significant endorsement of the group.
Perceived personal attributes
The respondents’ perceived attributes of persons with mental illness was assessed using a questionnaire designed by Angermeyer et al. covering two important stereotypes of mental illness: perceived dangerousness and perceived dependency [15]. The perceived dangerousness stereotype included five attributes: ‘unpredictable’; ‘lacking self control’; ‘aggressive’; ‘frightening’ and ‘dangerous’. The perceived dependency stereotype included three attributes: ‘needy’; ‘dependent on others’ and ‘helpless’. Respondents were asked to indicate if these attributes applied to the mentally ill. Again, for clear presentation of results and ease of computation, the sample was dichotomized based on the average endorsement of each of the stereotype group. Participants scoring more than the mean (+2SD) on each stereotype group were considered to have significant endorsement of that stereotype group. From this, endorsement of more than two items on the perceived dangerousness stereotype group (with five items) and more than one item on the perceived dependency group (with three items) were regarded as significant endorsement of that stereotype group.
Perceived prognosis of mental illness
Respondents were asked to choose, from four options, a single category to indicate their perception of the usual progression of mental illness. The options included ‘complete cure’, ‘partial remission’, ‘persistence’ and ‘deterioration’. Responses of ‘complete cure’ were classified as perceived good prognosis, ‘partial remission’, as perceived fair prognosis and ‘persistence’ or ‘deterioration’ as perceived poor prognosis.
Social distance towards people with mental illness
The respondents’ attitude towards people with mental illness was measured by assessing their desire for social distance towards people with mental illness. The participants completed a modified version of the Bogardus Social Distance Scale [16]. It included six items representing the following social relationships: marriage; sharing a room; friendship; working together; conversation; and family relationship. The six questions were rated on a 4-point scale (1 = definitely not, 2 = probably not, 3 = probably so, 4 = definitely so). It has recently been used in Nigeria to assess the attitude of the community [11] and university students’ [12] towards people with mental illness.
The study instruments were translated into Yoruba by a Yoruba-speaking psychiatrist and a Yoruba linguist. Precise idiomatic equivalents were used as much as possible. The back-translations, which were performed independently by another psychiatrist and linguist, were compared with the original translation by an independent panel and confirmed to be satisfactory before use.
Procedure
Written informed consent was obtained from the participants after the aims and objectives of the study had been explained. The Ethics and Research Committee of the Obafemi Awolowo University Teaching Hospitals Complex approved the study protocol. Research assistants who are medical students in psychiatry postings, fluent in both Yoruba language and English, administered the questionnaire to the participants. The participants could choose to complete the English or Yoruba versions of the instruments.
Data analysis
The data were analysed using the SPSS version 11 (SPSS, Chicago, IL, USA). For ease of analysis most of the variables were grouped. Results were calculated as frequencies (%), means, median and mode. Group comparisons were by χ2 test. Significance was calculated at p < 0.05. Logistic regression was used to calculate the variables independently associated with the high social distance. Odds ratio (OR) and 95% confidence interval (95%CI) were calculated.
Results
Sociodemographic variables
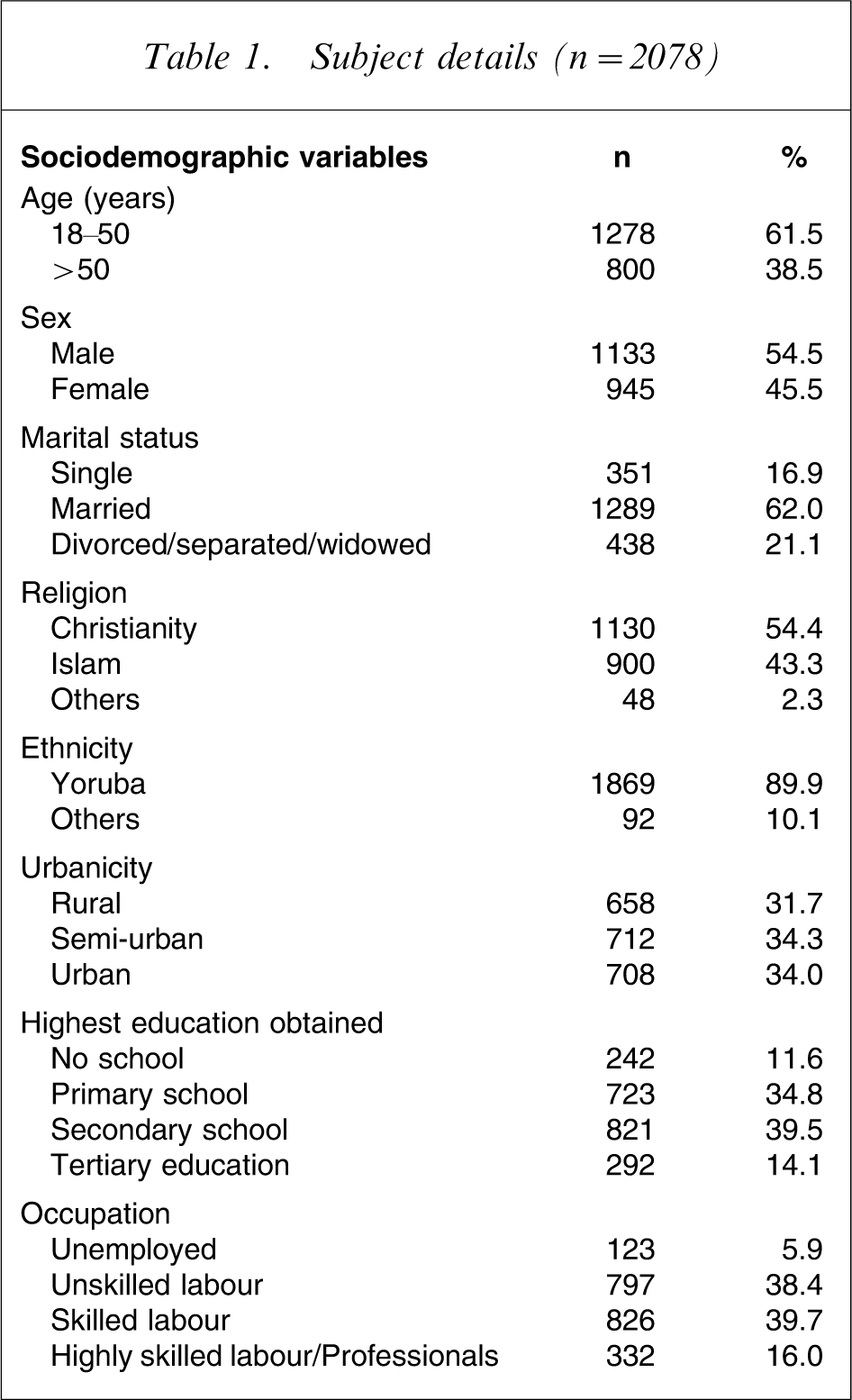
A total of 2078 respondents successfully completed the questionnaires. The sociodemographic details of the respondents (Table 1) indicate that they were mostly <50 years old (61.5%), male (54.5%), married (62.0%), Christian (54.4%) and from the Yoruba ethnic group (89.9%). A large percentage had secondary school education (39.5%) and were skilled labourers (39.7%).
Subject details (n = 2078)
Familiarity, perceived causation, stereotype and prognosis of mental illness
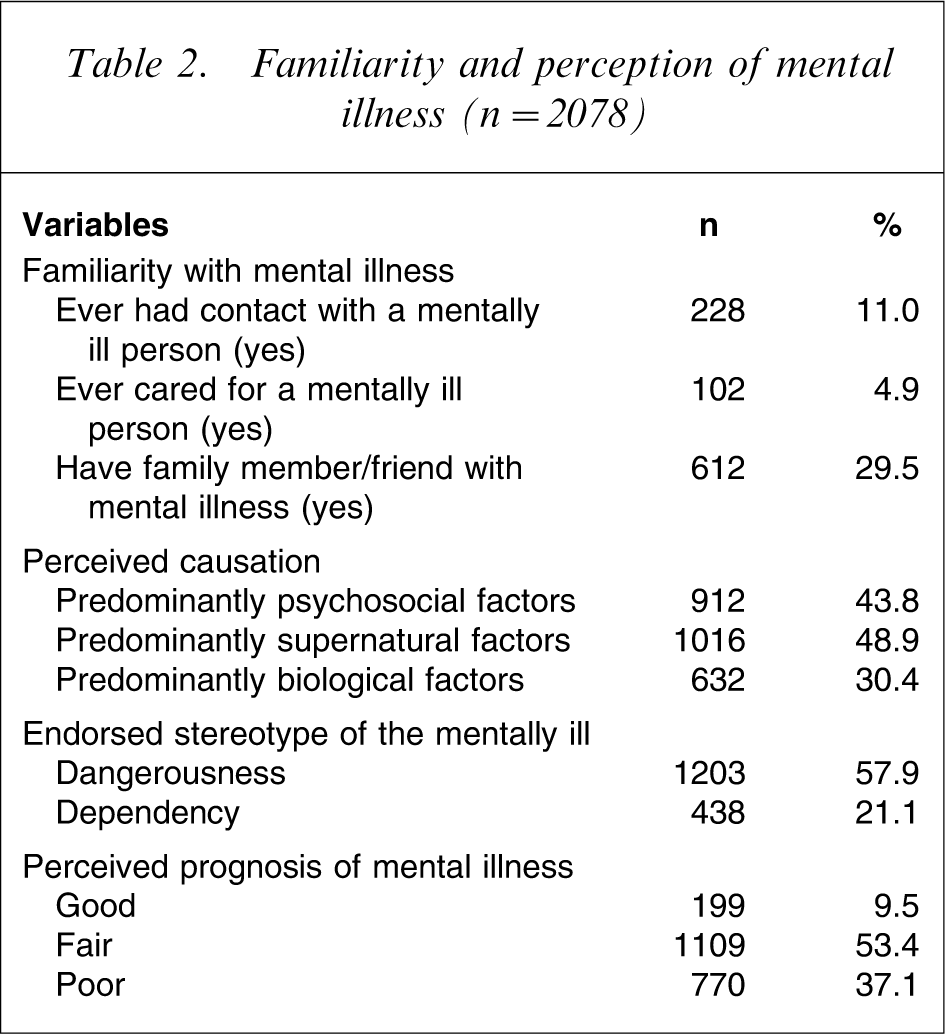
Table 2 shows that although 11.0% had had contact with the mentally ill, only 5.0% had actually cared for the mentally ill previously. Approximately one-third (29.5%) of the participants had a family member or friend with mental illness. Furthermore, while psychosocial causation of mental illness was significantly endorsed by 912 respondents (43.9%), supernatural and biological causations were significantly endorsed by 1016 (48.9%) and 632 respondents (30.4%), respectively. Also, the stereotype of ‘dangerousness’ was significantly endorsed by 1203 respondents (57.9%) while that of ‘dependency’ was significantly endorsed by 438 respondents (21.1%). Also, 199 respondents (9.5%) rated prognosis of mental illness as good, 1109 (53.4%) as fair and 770 (37.1%) as poor.
Familiarity and perception of mental illness (n = 2078)
Level of desired social distance towards people with mental illness
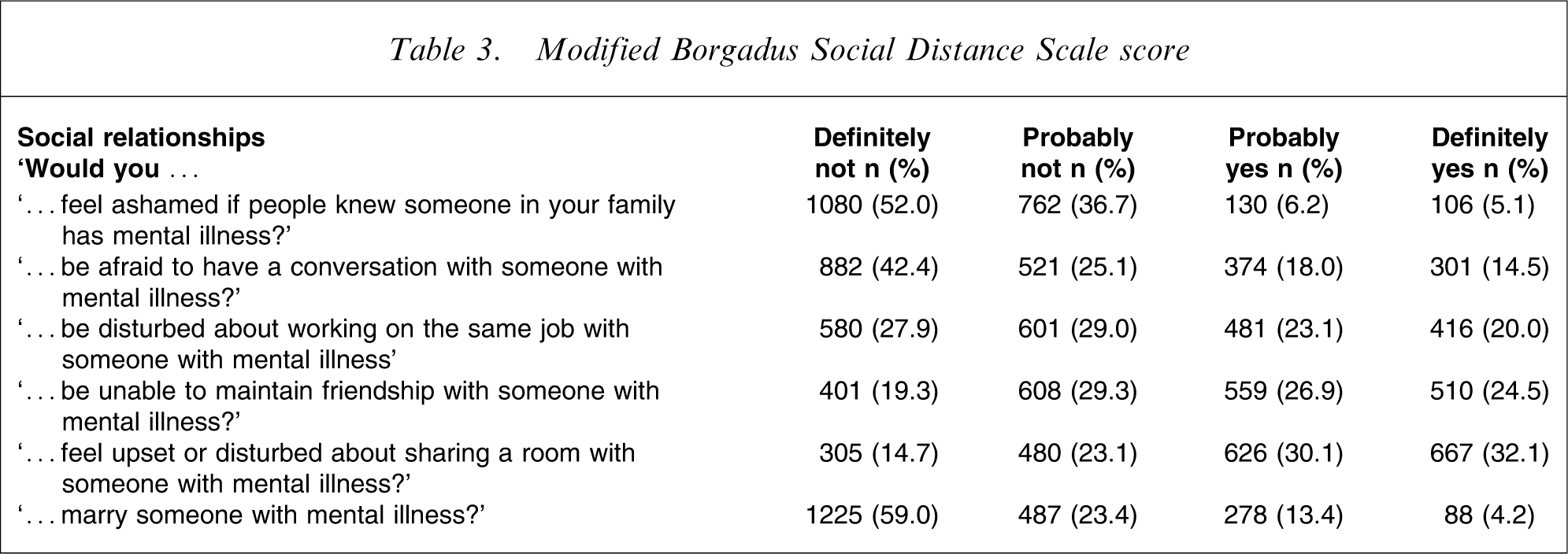
The level of desired social distance towards the mentally ill was seen to increase with the level of intimacy required in the relationship (Table 3). While 52.0% of the respondents would definitely not feel ashamed if people knew someone in their family had a mental illness, only 42.4% would definitely not be afraid to have a conversation with someone with mental illness. This percentage decreased to 27.9% for people who would definitely not be disturbed about working on the same job with someone with mental illness. Continuing along the same line, only 19.3% would definitely not feel disturbed or upset about sharing a room with someone with mental illness and only 4.2% would not be unwilling to marry someone with mental illness.
Modified Borgadus Social Distance Scale score
Several methods have been used to analyse the Social Distance Scale, but for simplicity and clarity we adopted the method used by Stuart and Arboleda-Florez [17], which have been subsequently used in the analyses of this scale in Nigeria [12]. The responses were grouped into the number of items answered desirably (‘definitely not’/‘probably not’), thus when all items were answered desirably, the participant was categorized as having low social distance, when one item was answered undesirably, he/she was categorized as having moderate social distance and when two or more items were answered undesirably, the participant was categorized as having high social distance towards the mentally ill.
Using this system 310 (14.5%) of the participants were categorized as having low social distance, 511 (24.6%) as having moderate social distance and 1266 (60.9%) as having high social distance towards the mentally ill.
Correlates of high social distance towards the mentally ill
Table 4 details the χ2 analysis of the association of the various variables with high social distance towards the mentally ill. The sociodemographic variables with significant correlation with high social distance included age (p < 0.001), urbanicity (p < 0.001) and highest education obtained (p = 0.005); ever care for the mentally ill (p < 0.001) and having a family member/friend with mental illness (p < 0.0001) were the familiarity variables with significant correlation with high social distance. Other variables significantly associated with high social distance included significant endorsement of supernatural causation (p < 0.001), perceived dangerousness (p < 0.001) and perceived prognosis of mental illness (p = 0.003). When these variables were then entered into a stepwise logistic regression analysis, high social distance was associated with having never cared for the mentally ill (B = 0.261, SE = 0.102, Wald = 21.103, df = 1, p < 0.001), older age (B = 0.845, SE = 0.292, Wald = 13.174, df = 1, p < 0.001), perceived supernatural causation of mental illness (B = 0.327, SE= 0.0543, Wald = 9.371, df = 1, p = 0.001) and perceived dangerousness (B = 0.413, SE = 0.035, Wald = 7.356, df = 1, p = 0.003). The OR and 95%CI for these independent correlates are shown in Table 5.
Factors associated with high social distance
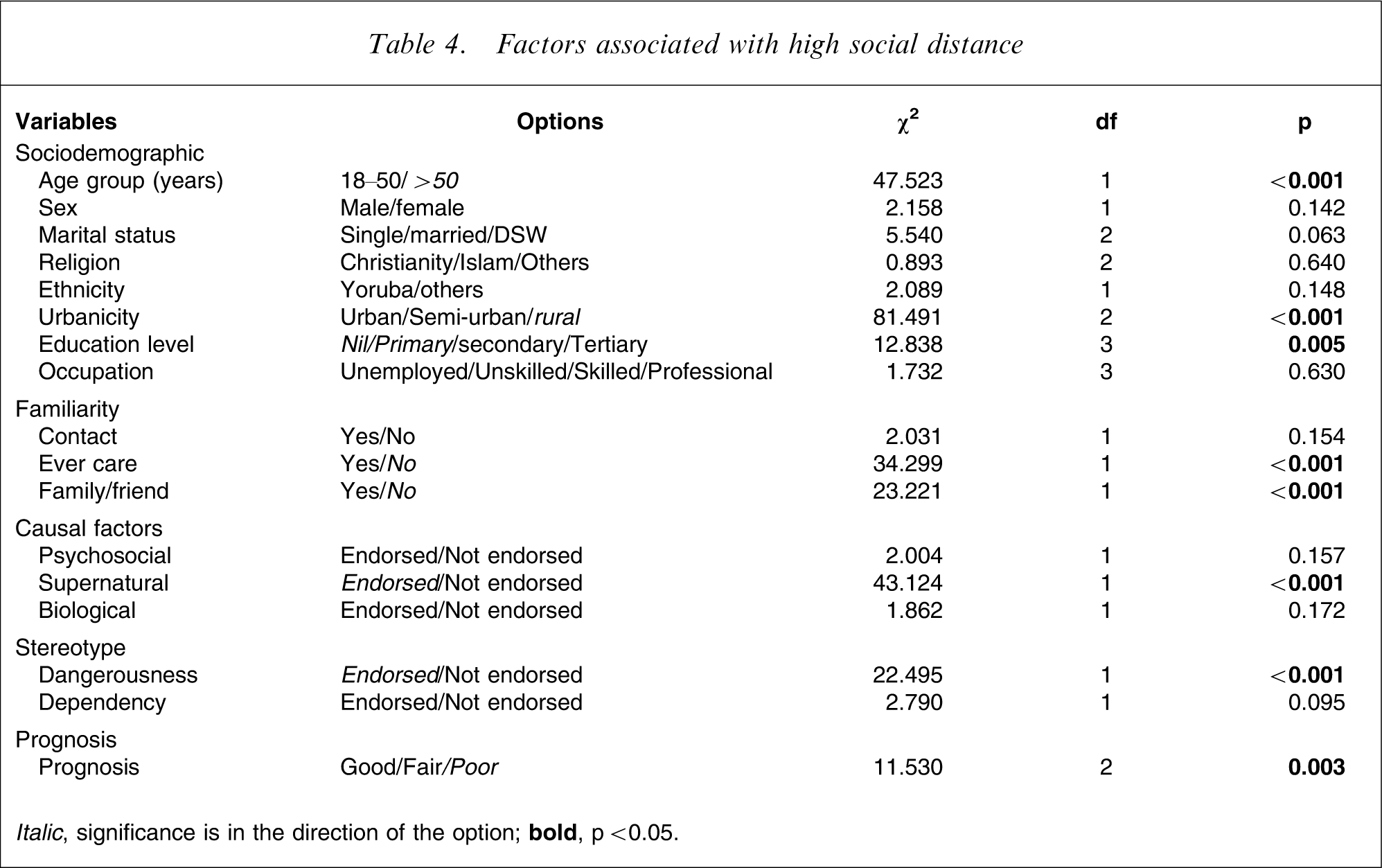
Italic, significance is in the direction of the option;
Variables independently associated with high social distance towards the mentally ill
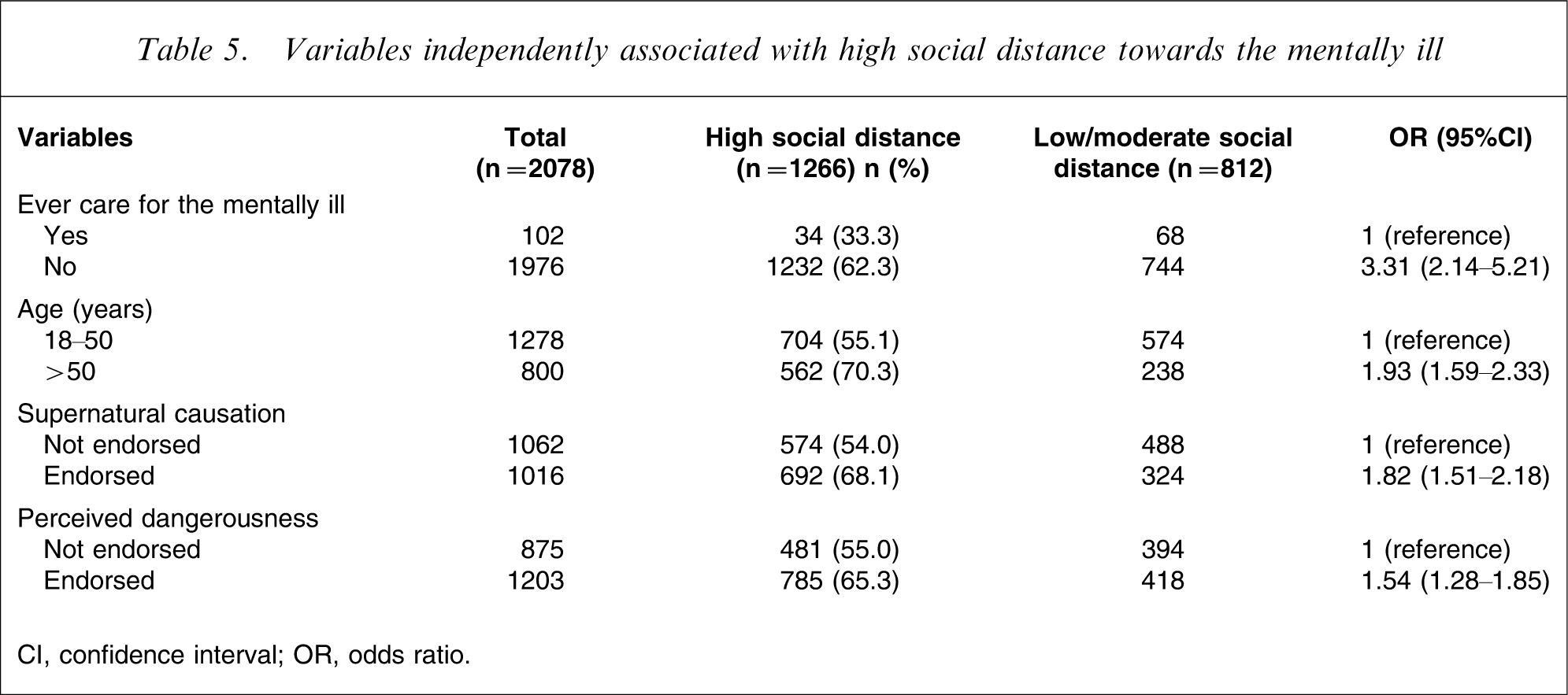
CI, confidence interval; OR, odds ratio.
Discussion
We had attempted to examine the public attitude (social distance) towards people with mental illness in southwestern Nigeria and the correlating factors. Caution, however, must be exercised in interpreting the results. We had considered mental illness in general and used this unitary concept of mental illness in describing the study and in administering the questionnaires. For example, the questionnaire relating to causes and to outcomes had forced choices and did not allow for responses that the causes and outcomes are various. This obviously had some drawbacks because it is known that the public have different views and attitudes towards different specific mental disorders.
The present findings showed that although nearly one-third had a family member or friend with mental illness only 4.9% had ever cared for a mentally ill person. The present study also found that a widespread belief in supernatural factors as the cause of mental illness was prevalent. This is in agreement with other studies both in the community [11] and even among doctors in Nigeria [13]. More than half of the population perceived the mentally ill to be dangerous and that mental illness had a fair to poor prognosis.
The present study also found a poor attitude towards the mentally ill among the communities in southwestern Nigeria, as evident by their high level of social distance towards the mentally ill. Eighty-two per cent of respondents would not marry someone with mental illness and 62.2% would be disturbed about sharing a room with someone with mental illness. Earlier studies in Nigeria among various populations including lay communities, university students and medical doctors have reported similar findings [11–13]. The present finding is also comparable with the rates found in Western culture. Seventy-seven per cent of the respondents would not marry someone with mental illness in Germany [18] and 75.2% would not in Canada [17]. The present result lends support to the increasing evidence from studies that suggests that stigmatizing attitude towards the mentally ill is not less evident in African countries as earlier thought [11–13], [19], [20].
We found that those who had ever cared for the mentally ill were threefold less likely to have high social distance towards the mentally ill than those who had never cared for the mentally ill. Care can lessen social distance in that those who care for the mentally are less likely to believe them to be dangerous [21] and thus are less afraid of them [22]. They are less likely to respond apathetically towards the mentally ill and therefore more willing to enter into a social relationship with them [23].
The present survey also found that respondents above 50 years were nearly twofold more socially distancing from the mentally ill compared to those below 50 years. This is in agreement with earlier studies that found a positive correlation between age and social distance towards the mentally ill, both in Western culture [17], [18], [24], [25] and in non-Western culture [26], [27]. It had been hypothesized that older people are likely to place more emphasis on negative characteristics and behaviour and therefore are prone to believe that the mentally ill will disrupt their social environment [17]. In addition older people are more likely to hold pre-scientific views about the causes of mental illness that have been known to affect attitude towards the mentally ill [5].
We found a strong correlation between belief in supernatural causation of mental illness and a high social distance towards people with mental illness. This is in agreement with most studies that have shown that views about causation are strongly associated with stigmatizing attitudes to mental illness [5–7]. Belief in supernatural causation might make close association with the mentally ill unattractive and even perceived as being risky. It may also imply that Western medical care would be futile and may lead to seeking alternative methods of treatment.
The present survey found a correlation between perceived dangerousness and high social distance towards the mentally ill. This is in agreement with studies that have shown that stigmatizing attitudes toward the mentally ill correlated with the belief that they are dangerous and violent [8]. This has led to the ‘harm-looming’ model of psychiatry stigma [28]. Weaker perception of dangerousness has been noted to correspond closely with less fear of people with mental illness, which, in turn is associated with less social distance [29].
Although correlation analysis initially showed some significant association between high social distance and variables such as urbanicity, level of education, having a family member/friend with mental illness and poor prognosis, these dropped out in the logistic analysis. The reasons for this may be the high level of correlation between these variables. Analysis showed strong correlation between ‘urbanicity’ and ‘level of education’, between ‘having cared for the mentally ill’ and ‘having a family member/friend with mental illness’ and between ‘perceived prognosis’ and ‘perceived causation.’
There were some limitations to this study. Care should be taken in generalizing the present results to other regions of Nigeria or sub-Saharan Africa. There are several cultural differences in Nigeria and sub-Saharan Africa and this may affect attitude towards the mentally ill. Information is required for each cultural group and a larger, multicentred cross-ethnic study is desirable in the future. Also, caution must be taken in inferring causality because this was a cross-sectional study and the related factors were only correlates. The strength of the study was in its large sample size, in its being community based and in coming from a culture not well studied.
In conclusion, the present findings have significant implications in that they supports the emerging evidence that there is a high level of social distance and stigmatization of mental illness in sub-Saharan Africa. The World Psychiatric Association anti-stigma programme should be extended to all areas of Africa. This study can serve as the baseline of knowledge and attitudes, which are the subjects of change, in anti-stigma campaigning, in Nigeria. This study suggests the need to incorporate anti-stigma educational programmes into the mental health policies of countries in sub-Saharan Africa. Such a policy should include community education regarding the causation, manifestation, treatment and prognosis of mental illness.