
Abstract
Objective:
This study aimed to compare the effectiveness of computerised cognitive behaviour therapy (CCBT) with a wait list control (WLC) for the treatment of patients with an anxiety disorder (social phobia, panic disorder, generalised anxiety disorder) referred to a specialist, publically funded, outpatient anxiety service.
Method:
Patients with social phobia (n = 37), panic disorder (n = 32) or generalised anxiety disorder (n = 14) were randomised to treatment with either CCBT (n = 40) or WLC (n = 43). Self-report rating scale assessments were conducted at baseline, 12 and 24 weeks.
Results:
Compared with WLC, the CCBT group improved significantly on approximately half of the self-report primary (the Work and Social Adjustment Scale) and approximately half of the secondary measures at both 12 and 24 weeks (the Liebowitz Social Anxiety Scale, the Penn State Worry Questionnaire, the Generalised Anxiety inventory and the Fear Questionnaire). Effect sizes in this study were moderate.
Conclusion:
This is one of the few studies to investigate CCBT for anxiety disorders in patients in a secondary care service. The results show that CCBT in this secondary care setting has the potential to be beneficial and confirms and extends the findings from previous studies of self-referral or primary care settings.
Introduction
Recent mental health surveys report that anxiety disorders are highly prevalent conditions which are associated with considerable disability (Wells et al., 2006). There is a robust evidence base for the treatment of these disorders with cognitive behaviour therapy (CBT) and most international guidelines recommend this as a first-line treatment. Despite these recommendations, epidemiological surveys indicate that the majority of people with these disorders do not seek, or are not having, treatment for them. Several reasons for this have been identified which include therapist availability and cost, the stigma involved with accessing mental health providers, and, particularly for anxiety disorders, a fear of attending treatment centres. In response to these issues a variety of computerised CBT (CCBT) programmes for the treatment of anxiety disorders have been developed, with a growing body of literature supporting their efficacy (Spek et al., 2007). These findings have been reflected by the National Institute for Clinical Excellence (NICE) recommending two CCBT systems for the treatment of anxiety and depression (NICE, 2006), and for CCBT to be included in the clinical guidelines for the management of adults with anxiety in community, primary and secondary care (NICE, 2004). It is important to note, however, that most of the literature in this area has involved participants who were recruited via media advertisements, community notices and/or web-links (Carlbring et al., 2005, 2006; Farvolden et al., 2005; Gega et al., 2004; Gilroy et al., 2000; Gruber et al., 2001; Harcourt et al., 1998; Jacobs et al., 2001; Kirkby et al., 1999; Klein et al., 2006; Knaevelsrud and Maercker, 2007; Lange et al., 2003; Newman et al., 1997; Richards and Alvarenga, 2002; Richards et al., 2006; Titov et al., 2008a, 2008b, 2008c, 2009), with a few studies recruiting participants via general practice and/or other health services (Cavanagh et al., 2006; Gega et al., 2004; Grime, 2004; Kenardy et al., 2003; Kenwright et al., 2001; Marks et al., 2004; Proudfoot et al., 2003, 2004).
It is not known how similar these patients are to patients with an anxiety disorder who have been referred to secondary care services under usual circumstances. However, by definition, patients are typically accepted into secondary care services if they are severely unwell and/or have complex or treatment-resistant difficulties. It has also been noted that patients recruited via media advertisements, community notices and/or web-links have had higher levels of education than might be expected from the general population (Carlbring et al., 2006). Therefore, it is unclear how well the findings from previous studies generalise to other care settings (Mataix-Cols et al., 2006), and in particular to secondary care settings. This has important clinical implications for recommendations about where CCBT is best placed in a stepped care approach to treatment.
This study was conducted in a real-world, clinical setting and aimed to be the first controlled study to investigate CCBT for anxiety disorders in patients who had been routinely referred to a secondary care, specialist anxiety disorders service (a naturalistic, uncontrolled study of eight sessions of CCBT in a specialist CBT centre in the UK has reported benefits (Learmonth et al., 2008)). The aim was to compare the effectiveness of CCBT with a control condition (remaining on the waiting list) for patients with a current primary anxiety disorder. It was hypothesised that in these patients CCBT would be an effective intervention and that those participants randomised to receive CCBT compared with those remaining on the waiting list would have a greater reduction in measures of anxiety symptoms and an improvement in their overall functioning.
Method
Overview
This randomised clinical trial was conducted in collaboration with the Anxiety Disorders Unit (ADU), a publicly funded, specialist, outpatient anxiety service in Christchurch, New Zealand. Patients with a current primary diagnosis of generalised anxiety disorder (GAD), panic disorder or social phobia were potentially eligible to participate in the trial. Following screening and a clinical assessment, suitable patients were invited to participate in the trial, while waiting to be assessed by the ADU (usual waiting time for a non-urgent assessment is approximately 9 months). Eligible and consenting participants were randomised to either treatment with CCBT or the wait list control (WLC) condition. Treatment involved CCBT using the CRUfAD programme (described in Acknowledgements) with participants having four to six sessions of CCBT to complete over 12 weeks. The WLC condition involved no active treatment. Assessments were conducted at baseline, 12 weeks (the end assessment) and at 24 weeks (the follow-up assessment) for all participants in the trial.
Recruitment
The participants for this study were recruited between June 2006 and November 2008 from referrals to the ADU. Patients were referred to this service by general practitioners and mental health clinicians. At the time of referral the referrers were not aware that suitable patients would be offered participation in the study, which meant that participants were not pre-selected for trial suitability by the referrer. The unit does not accept self-referrals.
Eligibility criteria
For participation in the study, participants were required to have a current primary DSM-IV diagnosis of GAD, panic disorder (with or without agoraphobia) or social phobia, to be aged between 18 and 65 years of age, to have access to a computer, and to have sufficient competency with the English language to manage the requirements of the computer programme and questionnaires. Patients were not eligible for the study if they required urgent intervention, if there was active suicidal ideation, or if their current primary anxiety disorder was obsessive compulsive disorder, post-traumatic stress disorder or a specific phobia (because the computer programme used in the study did not have specific treatment packages for these conditions). Patients were also not eligible for the study if they had a current diagnosis of substance dependence, psychotic illness, bipolar I disorder, or a significant or disabling cardiac, respiratory or neurological condition (which would make participation in the trial medically unwise). Regarding their treatment status, participants were not eligible if they were currently receiving CBT for their anxiety disorder or had started on, or changed the dose of, an antidepressant in the previous 6 weeks.
Procedure
Referrals to the ADU were reviewed by clinicians (CB, HC) at a standard, clinical triage meeting. Patients were excluded from the study if the referral indicated that the patient met one or more of the exclusion criteria. Following these exclusions, potentially suitable participants were sent a letter providing information about the trial and asking them to contact a clinician (HC) at the ADU if they wished to have no further contact about the study. Patients who had not opted out of further contact were then telephoned by the research assistant (CBo, WM) and invited to participate in a screening telephone interview. The purpose of this was to identify exclusion criteria at this stage. Patients who appeared to be suitable for the trial were then offered an assessment with an experienced clinician (CB, HC, FC) either in the participant’s own home or at the clinical research unit (CRU), depending on the participant’s preference.
At this baseline assessment, demographic and clinical information was collected and all patients participated in a structured clinical interview for DSM-IV Axis I disorders (SCID-I/P) to determine eligibility for the trial and to identify the current primary anxiety disorder (GAD, panic disorder or social phobia). Eligible patients provided written, informed consent to participate in the study. They were then randomised to either CCBT or the WLC, using a stratified block design for the primary diagnosis (GAD, panic disorder or social phobia). The stratified randomisation list was generated by a statistician (CF) who was not involved in implementation of the study. The allocation list and envelopes containing the allocations were held by the CRU coordinator (who was not involved directly in implementation of the study) to ensure that the clinicians and the research assistant involved in assessment and enrolment were not biased in the enrolment process. Participants were randomised in a 1:1 ratio to the computerised programme and WLC.
All participants in the trial were then given a battery of self-report questionnaires to complete over the following week. Participants who had been randomised to CCBT were provided with an individualised computer log in for the CCBT programme for their specific disorder. All participants in the trial (both those randomised to CCBT and those to WLC) were contacted by the research assistant at two-weekly intervals across the treatment phase of the study (six times over the 12 weeks). Self-report questionnaires were collected at 12 weeks (end assessment) and 24 weeks (follow-up assessment). All self-report questionnaires were returned by post. Following receipt of the final self-report questionnaires at 24 weeks, participants were given $150 in recognition of the time spent in participating in the trial.
The trial was registered with the Australasian Clinical Trials Registry as ACTRN012606000349549 and was approved by the Upper South B Regional Ethics Committee, Christchurch, New Zealand: URB/06/05/039.
Measures
All participants in both CCBT and WLC conditions completed the self-rated questionnaires described below at baseline, 12 weeks (end assessment) and 24 weeks (follow-up assessment). The primary outcome measures were self-report scores on the Work and Social Adjustment Scale (WSAS) (Mundt et al., 2002) as measures of the global severity and impact on functioning of the anxiety disorder, and a self-report scale of anxiety severity, the Patients Global Impression (PGI) scale (Guy, 1976), a Likert scale with a score range from 1 (not a problem) to 7 (extreme problem). These measures were chosen because they measure symptomatology and functioning across the different anxiety disorders. The secondary outcome measures were scores on measures relating to symptoms of the specific anxiety disorders: for GAD – Penn State Worry Questionnaire (PSWQ) (Meyer et al., 1990) and Generalised Anxiety Disorder Assessment Inventory (GADI) (Argyropoulos et al., 2007); for panic disorder – Panic Disorder Severity Scale (PDSS-SR) (Shear et al., 1997); and for social phobia – Liebowitz Social Anxiety Scale (LSAS) (Safren et al., 1999) and Fear of Negative Evaluation (FNE) (Watson and Friend, 1969). Measures of general anxiety were rated using the Fear Questionnaire (FQ) (Marks and Mathews, 1979) and Beck Anxiety Inventory (BAI). The tertiary outcome measures were scores on ratings of depression – Beck Depression Inventory (BDI-II) – and self-report scores from anchored Likert scales of participants’ ratings of their satisfaction with the programme (0–8) and the acceptability (0–8) of the treatment. All measures used have been shown to have established and adequate psychometric properties.
Treatment conditions
Participants randomised to CCBT were provided with treatment via the CRUfAD programme, developed by the Clinical Research Unit for Anxiety and Depression (CRUfAD) at St Vincent’s Hospital, Sydney. The content of the programme was based on best-practice, evidence-based CBT techniques (Andrews et al., 2003). The programme was structured and interactive and consisted of online lessons (GAD: four lessons; panic disorder: six lessons; social phobia: six lessons). Part of the content of each lesson was presented in the form of an illustrated story about someone with GAD, panic disorder or social phobia who successfully gains mastery over their symptoms. The lessons provided education about the symptoms and treatment of the particular disorder, gave instructions about developing an exposure hierarchy and practising graded exposure, demonstrated principles of cognitive restructuring and concluded with information about relapse prevention. Each lesson included a printable summary and homework assignment. Each lesson had to be completed to allow progression to the next lesson. Participants were encouraged to complete the lessons within 12 weeks of starting. The programme required a reading age of 11 years and no prior computer experience. Participants in the WLC condition received no active treatment. Over the duration of the study all participants (both in the CCBT and WLC groups) remained on the waiting list for assessment at the ADU, and continued under the care of their general practitioner.
Participant support
For both groups, the study involved minimal contact from the research assistant (CBo, WM), who were not clinicians. The aim of this contact was to maximise compliance while balancing the need for CCBT to be delivered in the context of a real-world, busy, clinical service. The research assistant telephoned participants in the CCBT condition every 2 weeks over the treatment phase of the study (i.e. the first 12 weeks) to ensure that they were not having difficulties accessing CCBT, and to encourage ongoing participation. In order to control for this input, the WLC group were also contacted by the research assistant every 2 weeks over the same timeframe. The content of the telephone call followed a predetermined structure for both groups and was of about 5 minutes’ duration. It involved checking if participants were having any technical problems with the programme and encouraged them to complete the sessions.
Data analysis
All data analysis was carried out according to a pre-established statistical analysis plan. Analyses of participants’ self-rated questionnaire scores were undertaken using mixed model repeated measures (MMRM) controlling for baseline scores and testing for the between-group factors of group (CCBT, WLC) and primary diagnosis (GAD, panic disorder, social phobia). The primary term of interest from these models is the time*group interaction, indicating the extent of differences in the changes over time between the two randomised groups. Additionally, the time*group*primary diagnosis interaction would provide evidence for a differential effect of treatment depending upon primary diagnosis. In circumstances where these interactions were significant, these were further explored by testing changes within groups. This analysis was completed for scores from the self-report rating scales at 12 weeks (end assessment) and 24 weeks (follow-up assessment).
Prior to the study commencing, an a priori definition of a completer of CCBT was made as being a participant who completed at least three out of a total of four lessons for GAD, and four out of six lessons for panic disorder and social phobia. This threshold was determined by the clinicians (CB, HC, FC) because it was felt to represent an adequate dose of treatment. The analyses described above for the outcome measures were repeated for the completers (as defined above) subset of CCBT and WLC.
Putative predictors of outcome were identified from the individual and group CBT literature and included six measures: the severity of the anxiety disorder as measured by the baseline PGI, the duration of the illness, the number of DSM-IV diagnoses, the BDI-II scores at baseline as a measure of depressive symptoms, medication status, and whether previous psychological treatment had been received for anxiety. These potential baseline predictors of response to treatment at 12 weeks (scores on PGI, WSAS, GADI, PSWQ, PDSS, LSAS, FNE, FQ, BAI, BDI-II) were tested statistically using independent t-tests and correlation coefficients. In addition, for the CCBT group, we tested the association between computer competence and treatment outcome using correlation coefficients.
Effects sizes for changes were calculated as Cohen’s d both between-groups and within-groups for the CCBT (to allow some comparison with previous literature), based on the pooled standard deviation from the analysis of covariance.
Based on the data from a RCT study (Marks et al., 2003), a total sample size of 80 (40 CCBT:40 WLC) was calculated to have 80% power to detect a difference change of > 1.6 on FQ Global Phobia ratings (similar to the PGI used in this study).
A two-tailed p-value of < 0.05 was taken to indicate statistical significance.
All analyses were undertaken using SPSS 13.0.
Results
Patient flow
Figure 1 shows the flow of patients through the study. The ADU received 1141 referrals over the trial period. Eligibility for the study was determined as described above. The most common reasons identified for patients not being suitable for the study were that they required urgent intervention, that their primary anxiety disorder was not GAD, panic disorder or social phobia, that they were already receiving a treatment which excluded them, or that they had another diagnosis which excluded them from the study (summarised in Table 1). This issue of suitability for the study is discussed fully in a companion paper (Carter et al., 2012). Table 2 summarises the demographic and clinical characteristics of the study participants. There were no significant differences between the CCBT and WLC groups at baseline.
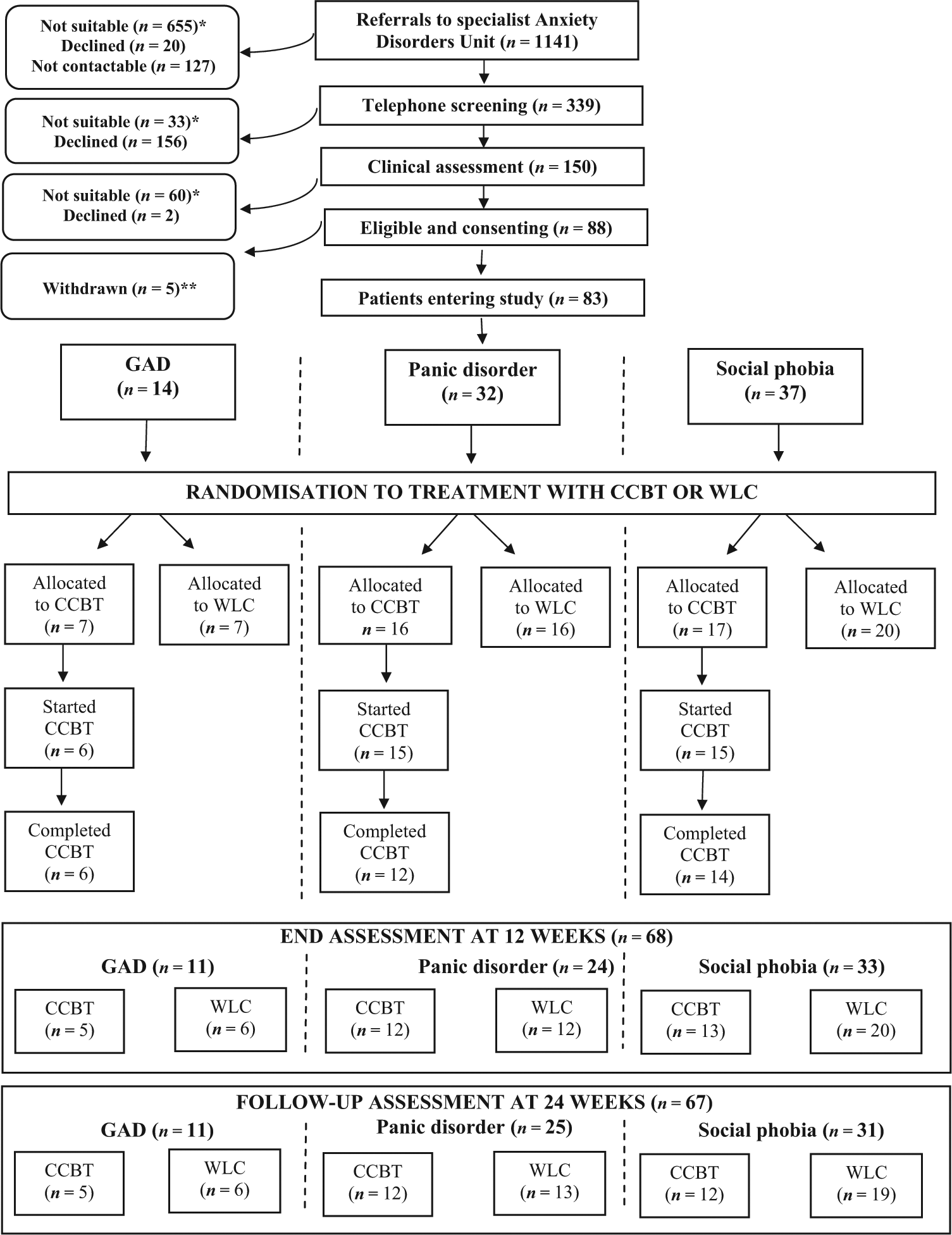
Schematic showing patient flow through the study
Summary of reasons why patients were not suitable for the study
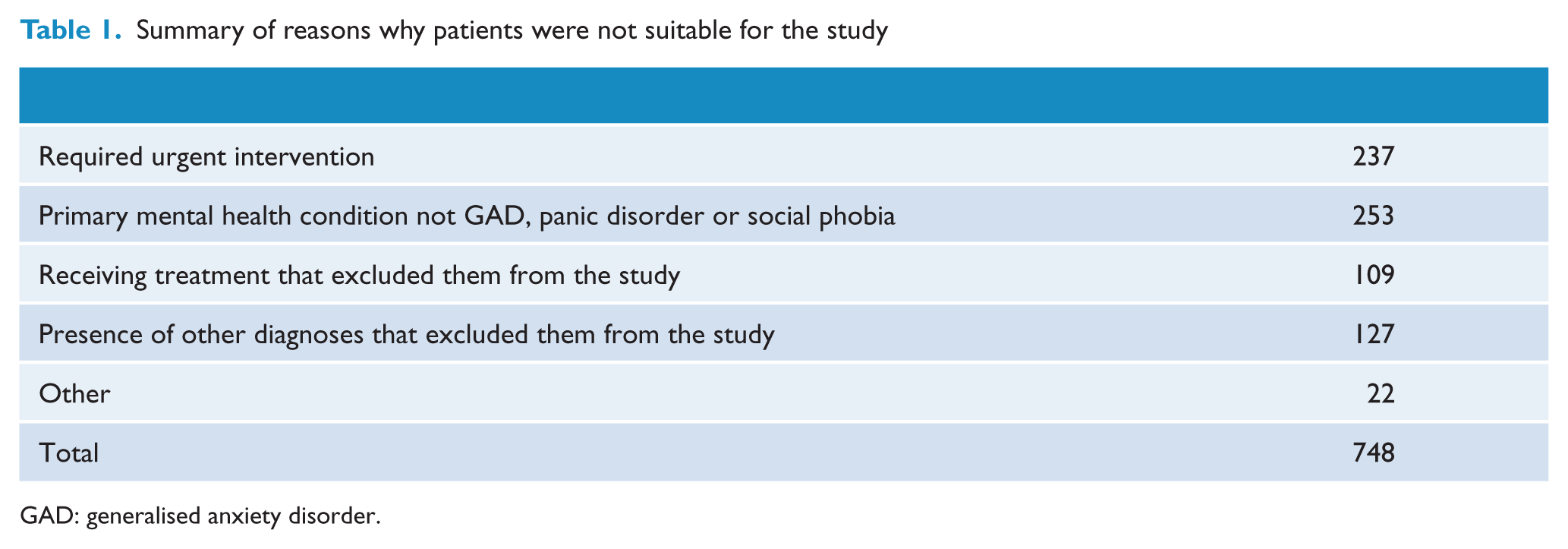
GAD: generalised anxiety disorder.
Demographic and clinical characteristics.
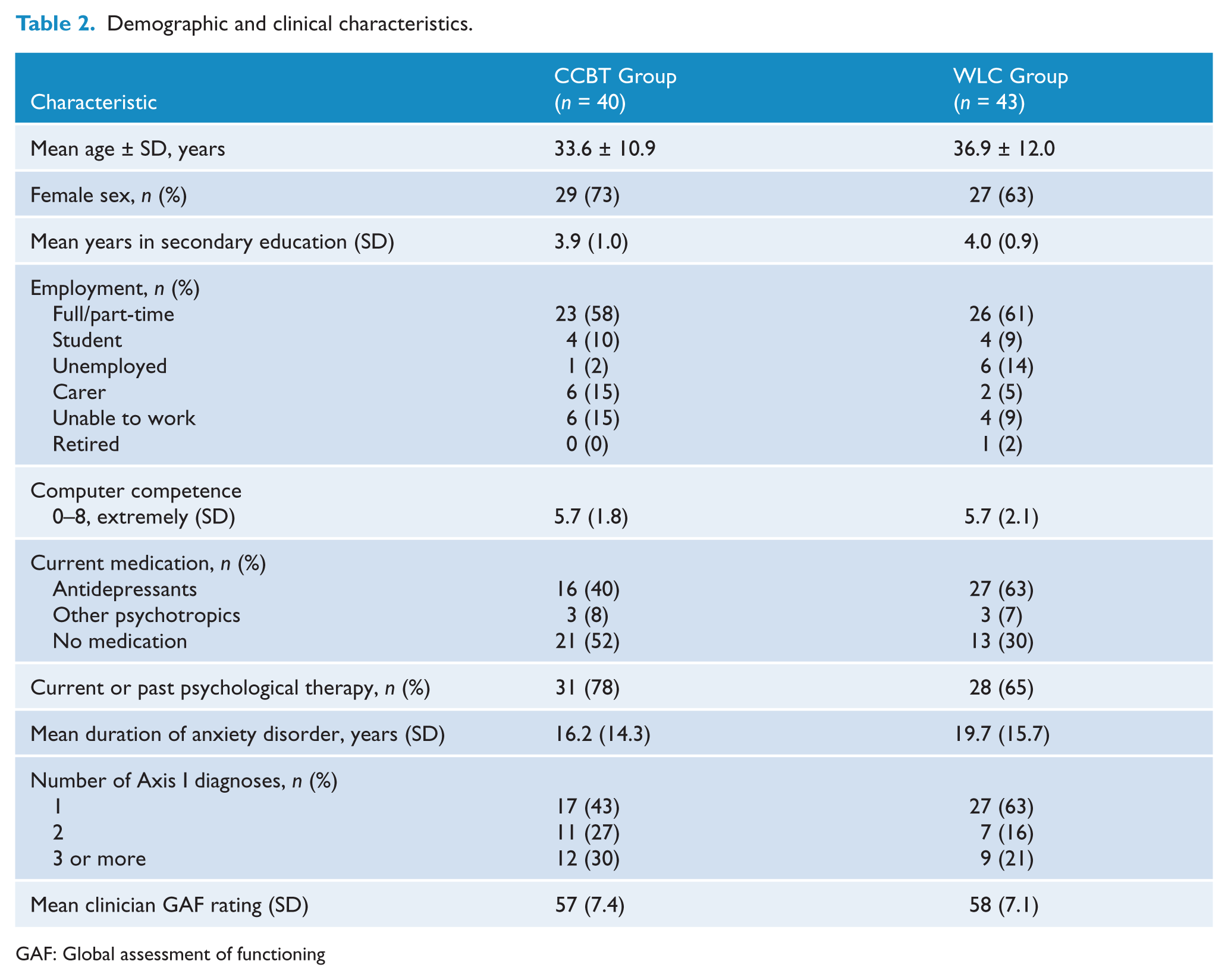
GAF: Global assessment of functioning
At the start of the study, the computer programme had a fault which resulted in a change of the computer programme. The five patients this involved were excluded from the study.
The remaining 83 participants who met inclusion criteria and gave written, informed consent for the study were allocated to a diagnostic group based on their primary anxiety diagnosis (GAD (n = 14), panic disorder (n = 32), or social phobia (n = 37)). Participants were then randomised to CCBT or WLC, within their diagnostic blocks (GAD: CCBT = 7, WLC = 7; panic disorder: CCBT = 16, WLC = 16; social phobia: CCBT = 17, WLC = 20). In total, 40 participants were randomised to CCBT and 43 were randomised to WLC.
Assessments and number of participants completing ratings
Of the 83 participants who provided informed consent and were randomised, six patients (four from CCBT; two from WLC) withdrew after the baseline assessment, but were included in the data analysis. At the end assessment at 12 weeks, data were collected from 68 of the original sample of 83 (GAD = 11/14; panic disorder = 24/32; social phobia = 33/37). A total of 25% of participants randomised to CCBT and 12% of those randomised to WLC did not provide questionnaires at this assessment. As shown in Figure 1, four patients who did not complete the CCBT (from the a priori definition described above) participated in the end assessment. At the follow-up assessment at 24 weeks, data were collected from 67 of the original sample of 83 who participated in the assessment (GAD = 11/14; panic disorder = 25/32; social phobia = 31/37). Similar to the follow-up assessment, 28% of participants randomised to CCBT and 12% of those randomised to WLC did not provide questionnaires at this assessment. Three patients who did not complete the CCBT participated in the follow-up assessment.
Outcome measures for CCBT and WLC
The self-report measures at baseline, end assessment (12 weeks) and follow-up assessment (24 weeks) are shown in Table 3.
Mean and standard errors of outcome measures over time from ANCOVA model.
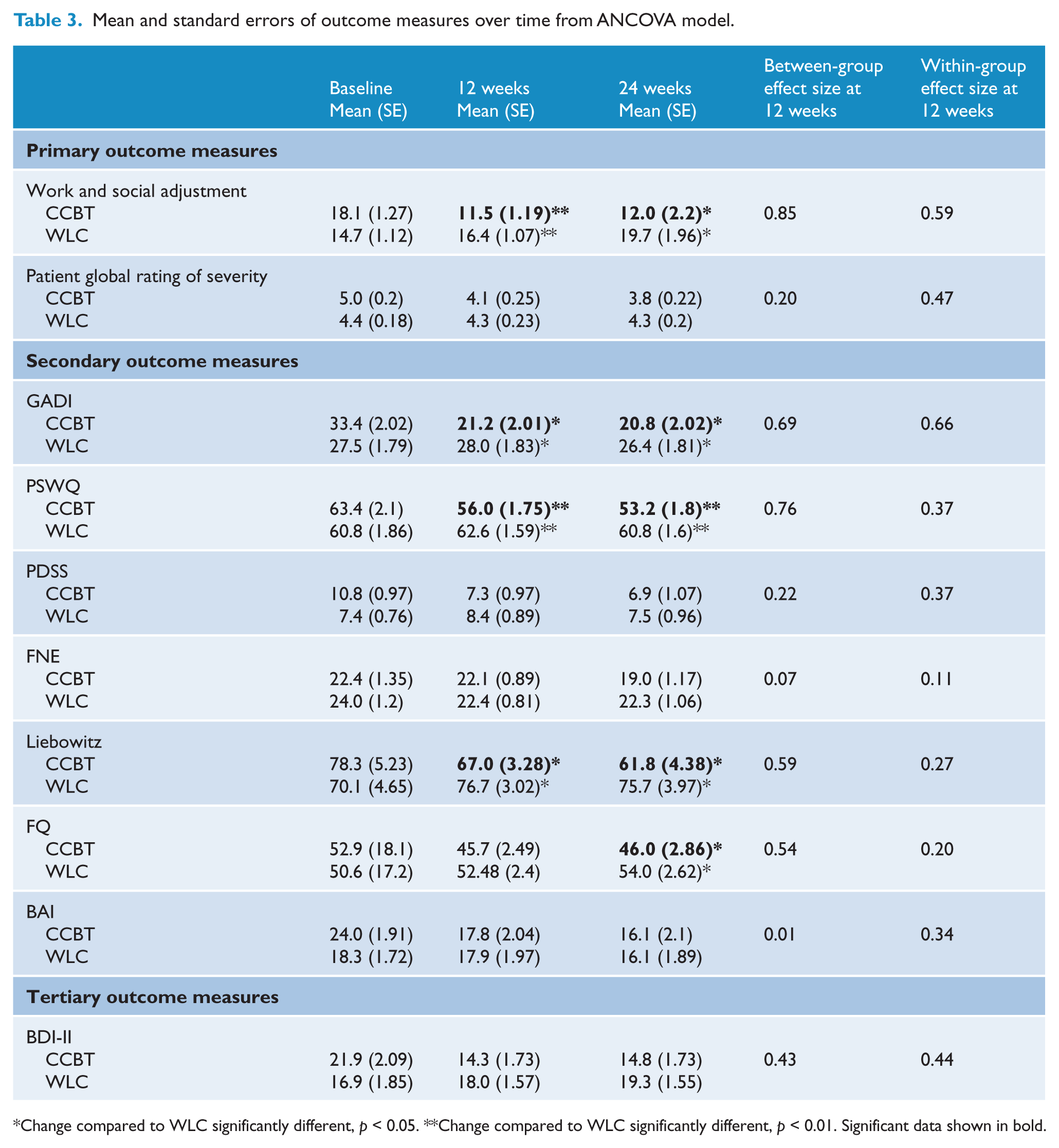
Change compared to WLC significantly different, p < 0.05. **Change compared to WLC significantly different, p < 0.01. Significant data shown in bold.
There were no statistically significant differences between the CCBT and WLC groups at baseline.
Primary outcome measures
Significant group * time interactions were obtained for WSAS scores at 12 weeks (F (1,61) = 9.3; p = 0.003) and 24 weeks (F (1,60) = 6.6; p = 0.01). Post hoc tests indicated that the CCBT group had improved significantly between the baseline pre-treatment and 12 and 24 week post-treatment assessments. No significant group by time interactions were found for the PGI scale (i.e. at 12 weeks) (F (1,61) = 0.5; p = 0.48), although they approached significance at 24 weeks (F (1,60) = 3.8; p = 0.06).
Secondary outcome measures
Significant group * time interactions were obtained for both GAD measures, GADI at 12 weeks (F (1,61) = 6.3; p = 0.02) and 24 weeks (F (1,60) = 4.2; p = 0.04), PSWQ at 12 weeks (F (1,61) = 7.7; p = 0.007) and 24 weeks (F (1,60) = 9.7; p = 0.003); the LSAS measure of social phobia at 12 weeks (F (1,61) = 4.6; p = 0.04) and 24 weeks (F (1,60) = 5.4; p = 0.02); and the FQ, a general measure of anxiety, at 24 weeks (F (1,60) = 4.2; p = 0.04). The other secondary outcome measures (PDSS, FNE and BAI) did not show significant differences.
Tertiary outcome measures
No significant group * time interactions were obtained for the BDI-II.
Participants rated their satisfaction and acceptability of the CCBT favourably from Likert scales (0–8) with mean scores of 5.6 (SD 1.5) and 5.9 (SD 1.8) for ratings of satisfaction and acceptability, respectively.
Effect sizes
The between-group effect sizes (pooled SD) at 12 weeks are shown in Table 3. The highest value was found on the primary outcome measure of the WSAS (Cohen’s d = 0.85). Moderate (0.4–0.8) between-group effect sizes were found on the measures of generalised anxiety (GADI and PSWQ), on the LSAS (a social phobia measure), on the FQ and the BDI-II. As shown in Table 3, the within-group effect size at 12 weeks for the PGI, WSAS and GADI were moderate while other measure effect sizes were small.
Primary diagnostic group and outcome
There was no significant differential effect of CCBT depending on primary diagnostic group (i.e. GAD, panic disorder or social phobia) for any measures.
Completion rates and effect on outcome
Of the 40 patients randomised to CCBT, 14 (35%) did not complete the treatment (as defined above) (GAD = 2/7, 29%; social phobia = 5/17, 29%; panic disorder = 7/16, 44%). Differences in dropout rates from the CCBT across the diagnostic groups were not statistically significant (p > 0.05 using chi-square). Analysis comparing the subgroup of completers of CCBT and WLC produced similar significant results as the primary analysis of CCBT and WLC with the minor exception that the FQ total was significant for the subgroup of completers (p = 0.048) but not in the primary analysis (p = 0.058).
In order to allow comparison with other CCBT studies using the same programme in different settings and with different design, the absolute completion rates of the CCBT (i.e. all sessions completed) were 4/7 (57%) patients with GAD, 9/17 (53%) patients with social phobia, and 5/16 (31%) patients with panic disorder.
Potential predictors of outcome
None of the associations between the six putative baseline predictors and the 10 outcome measures were statistically significant (all p > 0.05) (results not shown).
Computer competence was not correlated with treatment outcomes for the CCBT group (all p > 0.05) (results not shown).
There were no adverse events reported for any participants in the trial.
Discussion
Is CCBT effective in patients referred to a secondary service?
The primary aim of this study was to address the efficacy of CCBT for patients with a range of primary anxiety disorders (GAD, panic disorder or social phobia) who had been routinely referred to a secondary clinical service. The results suggest that in the setting of a specialist anxiety disorder service, CCBT with minimal contact (i.e. telephone calls from the study co-ordinator every 2 weeks) can be effective in treating these anxiety disorders. The participants in the CCBT group compared with the WLC improved significantly on some (approximately half) of the self-report measures used. In particular, the changes to the primary outcome measure of functional impairment showed significant change at both 12 and 24 weeks. These changes in the functional effects of anxiety are important. The other primary outcome measure, the PGI, however, did not change significantly, although it showed a trend towards improvement. Previous studies have reported that global measures of improvement or severity of illness have tended to change less than measures of specific symptoms or functioning (Bergstrom et al., 2010). Interestingly none of the diagnostic groups (GAD, panic disorder or social phobia) benefitted more from the treatment than any of the other diagnostic groups.
At the time the study was commenced there had been no previous controlled trials evaluating CCBT in participants recruited from a secondary care service. Over the course of the study, two studies from the Karolinska Institutet, Sweden involving CCBT for social phobia and panic disorder in routine psychiatric care were published which suggested similar positive benefits for CCBT in these settings (Bergstrom et al., 2010; Hedman et al., 2011).
Effect size
The effect sizes in this study were moderate, and lower than those reported by previous therapist-assisted CCBT studies (typically of self-referred participants) of a single disorder (e.g. social phobia), which have reported moderate to large mean within-group effects sizes of 0.8–1.0 (Aydos et al., 2009; Carlbring et al., 2005; Titov et al., 2008b). The reasons for the more modest effect sizes in our study may relate to several factors. A consistent theme reported by the CCBT literature is that studies with no or minimal therapist or study coordinator input (similar to this study) have generally reported lower effect sizes (Titov, 2007). The other possible reason for the more modest effect sizes may be a reflection of the study setting being in secondary care and therefore including participants less likely to respond to CCBT (for reasons of, for example, severity, illness duration, previous lack of treatment response). The participants in this study had anxiety of at least moderate severity and almost half of the participants had more than one DSM-IV diagnosis. This is consistent with the fact that they had been referred to a secondary care service. In comparison with other studies, particularly those of self-referred participants, there were high rates of psychotropic medication use (59% in comparison with 21–34% (Titov et al., 2008b)) and previous mental health treatment (71% in comparison with 30–40% (Titov et al., 2008b)). Participants also tended to have had fewer years of education and fewer were in full or part-time employment (60% in comparison with 75–90% (Carlbring et al., 2006; Titov et al., 2008b)). Despite these demographic indicators of severity and complexity, the generally positive outcomes reported by this study are encouraging and suggest that the previous positive findings from the literature are supported and generalisable. Interestingly, and in line with this interpretation, similar effect sizes have been reported for therapist-delivered CBT in both research and clinical settings. This suggests that clinical severity and complexity may not influence outcome to the degree previously thought (McEvoy, 2007).
Lack of suitability for study
Although these results are encouraging, a note of caution does need to be sounded in that, for a number of reasons, a considerable number of patients were not eligible for the study. Some of these factors related to issues of the trial design, such as not including patients who were felt to require urgent intervention, and not including those with obsessive compulsive disorder, post-traumatic stress disorder or a specific phobia (because the CCBT programme did not have treatment modules for these conditions). Other factors relate to the severity and complexity of the referrals received, such as the presence of other diagnoses (e.g. substance dependence, bipolar disorder or psychosis). This issue is discussed further in an accompanying paper (Carter et al., 2012), together with the issue of the acceptability of computerized treatment, which has been recognized as a factor of key importance (Kaltenthaler et al., 2008).
Completion rates
A total of 65% of participants randomised to CCBT completed at least 75% of the lessons in the required timeframe. The 35% of patients randomised to CCBT who did not complete treatment included 10% who did not start treatment and 25% who started but did not complete CCBT. The 65% completion rate is similar to a recent review which reported that a median of 56% of patients with anxiety and/or depression completed a full course of CCBT (Waller and Gilbody, 2009). The 65% completion rate is, however, somewhat lower than that reported for CCBT with more therapist contact (i.e. 80%) (Carlbring et al., 2006). In comparison with CBT delivered entirely by a therapist or through bibliotherapy, completion rates of 62–82% and 80%, respectively, have been reported. The influence of completion rates on outcome has not been clearly established; previous CCBT studies have reported that poor completion rates are not associated with differences in treatment outcome (Titov et al., 2008b), although a bibliotherapy study reported that the amount of reading done related positively to outcome (Rapee et al., 2007). Our findings are similar to the previous CCBT literature in that there was no difference in outcome between those who completed treatment (according to our predetermined definition) and those who did not.
Predictors of outcome
For maximising the use of CCBT in a stepped care approach, it would be very helpful to be able to predict those who would be likely to benefit from the treatment and conversely those likely to do less well. For therapist-delivered individual and group CBT, several factors have been cited as predicting poorer treatment outcome (i.e. duration and pre-treatment severity of the anxiety disorder, comorbidity, personality traits of neuroticism, and pre-treatment measures of participants’ motivation and their ratings of the credibility of the treatment) (Mennin and Heimberg, 2000). As yet, however, although there has also been an increasing interest in this area, no predictors of outcome to CCBT have been consistently identified (Spek et al., 2008). Supporting this literature we found no correlation between baseline predictors and outcome. We also found that computer competence was not correlated with treatment outcome, suggesting that CBT delivered in this way is not dependent on previous computer skill.
Limitations
Although one of the strengths of this study was that it was conducted in a real-world clinical setting, the fact that we excluded patients who were felt to require urgent intervention did limit the generalisability of the findings to this non-urgent group. In addition, there may also have been some self-selection bias in that participants all opted into the trial. All outcome measures were from self-report scales and there was no clinical assessment post-treatment of diagnosis-free status (i.e. the number or percent of participants who no longer met criteria for a diagnosis of an anxiety disorder). This would have been helpful but would have involved significant clinician time which was not available at the time of the study. A longer-term follow-up assessment to determine whether benefits were maintained over a longer time period (e.g. 1 year) would also have been helpful. However, by this time, participants would have been seen by the ADU, which would have influenced outcome. We were also not able to report on the percentage of participants who then went on to require face-to-face CBT at the ADU. There are issues related to a trial design which included both groups having an extensive clinical assessment with experienced clinicians and being given a clear diagnosis, which may have been a helpful intervention in, and may have overestimated the efficacy of, the WLC. We decided to use a waiting list as the control condition in this study because of the lack of studies evaluating the efficacy of CCBT in a secondary care setting. However, this may have resulted in well-recognised issues of WLCs, such as demoralisation from remaining without treatment. This may explain some of the between-group effects but this also reflects clinical practice.
Conclusion
This is one of the few studies to investigate CCBT for anxiety disorders in patients in a secondary care service. The results show that CCBT in this secondary care setting has the potential to be beneficial and confirms and extends the findings from previous studies of self-referral or primary care settings.
Footnotes
Acknowledgements
We are grateful to the Clinical Research Unit for Anxiety and Depression (CRUfAD) at St Vincent’s Hospital, Sydney, Australia for providing the CCBT programme at no cost. Other than this, CRUfAD were not involved in the design, implementation or analysis of the study.
The authors wish to thank research assistants Cecilia Bourke (CBo) and Wendy Mayes (WM) for the management of this study. Preliminary findings from this paper were presented at the Department of Psychological Medicine Research Meeting, Christchurch, New Zealand, May 2010.
Funding
This study was supported by the Canterbury District Health Board and was financed by the Canterbury Medical Research Foundation and New Zealand Lottery Grants Board.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.