
Abstract
Keywords
Introduction
Research to date has consistently demonstrated that eating disorder pathology and anxiety disorders frequently co-occur (for a detailed literature review see Swinbourne and Touyz, 2007). The prevalence of anxiety disorders amongst bulimia nervosa (BN) samples has been reported in a number of investigations (Brewerton et al., 1995; Bulik et al., Hudson et al., 1983, 1987; Laessle et al., 1989; Piran et al., 1985; Powers et al., 1988; Schwalberg et al., 1992) with lifetime prevalence rates of at least one anxiety disorder ranging from 25% (Keck et al., 1990) to 75% (Schwalberg et al., 1992). Similarly, prevalence amongst anorexia nervosa (AN) samples has also been investigated (Deep et al., 1995; Halmi et al., 1991; Herpertz-Dahlman et al., 1996; Laessle et al., 1987) with lifetime prevalence rates ranging from 23% (Laessle et al., 1987) to 75% (Deep et al., 1995). Studies have shown that the onset of an anxiety disorder often precedes the onset of an eating disorder (Brewerton et al., 1995; Bulik, 2003; Deep et al., 1995; Godart et al., 2003; Schwalberg et al., 1992). These findings have led some researchers to speculate that early-onset anxiety disorders may represent a potential genetically mediated pathway toward the development of an eating disorder (Kaye et al., 2004) and at the very least suggest that early-onset anxiety disorders may in some way predispose individuals to the development of an eating disorder (Bulik et al., 1996).
Although the specific nature of the relationship between eating disorders and anxiety is unclear, Godart et al. (2003) implicate three possible explanations for the observed comorbidity between eating and anxiety pathology. Firstly, that anxiety may be a risk factor for the development of an eating disorder. Secondly, that anxiety may be secondary to eating pathology, and thirdly that both disorders may share common vulnerability factors.
This area has been notoriously difficult to investigate due to the inherent problems associated with prospective studies of at-risk populations (Serpell et al., 2002). Although a number of studies have considered the temporal relationship between eating disorders and anxiety disorders, many of these have been retrospective. The retrospective research has focused on reporting the temporal relationship between the onset of both disorders and drawing inferences about aetiological links (Pallister and Waller, 2008). The methodological limitations associated with assessing the age of onset of psychiatric diagnoses by retrospective recall have been raised by a number of authors (Godart et al., 2000, 2003; Toner et al., 1988). Certainly prospective studies have the benefit of fewer potential sources of bias and confounding than retrospective studies, however there are few available prospective studies investigating the comorbidity between anxiety and the onset of eating pathology. Whilst retrospective data must be interpreted with caution, the results may nevertheless provide extremely useful information about the vulnerability factors that may be associated with the development of an eating disorder.
It is important to note that anxiety disorders do not always precede the onset of eating pathology. Godart et al. (2000) found that obsessive–compulsive disorder (OCD), generalised anxiety disorder (GAD) and panic disorder typically occurred simultaneously or following the onset of the eating disorder. Kaye et al. (2004) also reported from their sample that post-traumatic stress disorder (PTSD), panic disorder and agoraphobia tended to have an onset simultaneous or later than the eating disorder. These findings led to speculation that eating disorders may lead to or exacerbate anxiety symptomatology (Pallister and Waller, 2008). Once again, this gives rise to the possibility that anxiety symptomatology may be secondary to eating disorder pathology, such as malnutrition, rather than a distinct anxiety disorder diagnosis. Consequently, research in this area must be careful to clearly delineate between the anxiety symptoms related to eating pathology and those that represent a distinct anxiety disorder.
Understanding the relationship between eating disorders and anxiety pathology becomes more complicated when one considers the possibility that both may result from common vulnerability factors (Godart et al., 2003; Wonderlich and Mitchell, 1997). This theory proposes that early negative experiences may give rise to risk factors for the development of both disorders. Pallister and Waller (2008) describe this model in detail, suggesting that underlying vulnerability cognitions lead to harm avoidance cognitions which result in the implementation of safety behaviours comprising disordered eating and anxiety behaviours.
The suggestion that childhood anxiety may play an aetiological role in the development of eating disorders has stemmed from the possibility that excessive fear about certain events or situations may lead into excessive concerns about eating, shape and weight and subsequently lead to the development of eating pathology (Pallister and Waller, 2008). It is clear that further research needs to be conducted into the interaction between anxiety and specific prodromal symptoms of eating disorders (Jacobi et al., 2004).
As previously mentioned, the limitations inherent in the research in this area have impaired the utility of the results. In particular, there are difficulties establishing accurate prevalence rates for eating and anxiety disorder comorbidity, due to much of the previous research focusing on AN and BN, despite the indication that the residual category of eating disorder not otherwise specified (EDNOS) is at least, if not more common in clinical practice (Fairburn and Harrison, 2003; Fairburn and Walsh, 2002). A number of studies have also been limited by problems with sample sources and selection (extensive exclusion criteria, the use of small sample sizes and the use of mixed gender samples) and assessment procedures where adequate diagnostic instruments were not used.
A further limitation in the comorbidity research is that much of the research focuses on only a few of the anxiety diagnoses, often excluding PTSD, despite the suggestion that trauma is a risk factor for the development of eating pathology (Black Becker et al., 2004). A number of studies have demonstrated a positive association between child sexual assault (CSA) and clinical eating disorders (Fallon and Wonderlich, 1997; Johnson et al., 2002; Root and Fallon, 1989; Steiger and Zanko, 1990; Vize and Cooper, 1995; Welch and Fairburn, 1994). Links have also been proposed between a history of CSA and specific eating disorder symptoms, specifically bingeing, vomiting and negative body image (Waller, 1992; Waller et al., 1993). It has also been suggested that abuse may act as a moderator between a range of causal factors and eating disorder pathology (Van Gerko et al., 2005). Despite this, there is a distinct lack of research examining the prevalence of eating disorders among patients presenting with anxiety disorders. Consequently the frequency of eating disorder pathology amongst patients presenting to specialty anxiety clinics remains unclear, as does the question of whether eating disorders are associated with some anxiety disorders more than with others (Black Becker et al., 2004). Subsequently, without this information, it is difficult to clearly understand the pattern of comorbidity between eating and anxiety disorders (Pallister and Waller, 2008).
The clinical implications of this are significant, raising the possibility that eating disorders may go unidentified and untreated, particularly given that eating disorder assessment and treatment is often viewed as a clinical specialty (Black Becker et al., 2004). The absence of formal eating disorder assessment in anxiety treatment settings is also indicated by the lack of eating disorder assessment items in assessment instruments for the anxiety disorders. An example of this is the Anxiety Disorders Interview Schedule (ADIS-IV; Brown et al., 1994), arguably one of the best structured interviews available for the assessment of anxiety disorders, which does not include an assessment of eating pathology in the sections that screen for other Axis I disorders commonly comorbid with anxiety disorders.
The only study, to our knowledge, which has investigated eating disorder rates amongst women presenting to an anxiety clinic is that by Black Becker et al. (2004). They found that 12% of 257 women presenting to an anxiety clinic met criteria for a possible eating disorder. Other studies have investigated eating disorder rates amongst specific anxiety disorders (Brewerton et al., 1993; Lipschitz et al., 1999) or amongst individuals with sexual abuse trauma (Faravelli et al., 2004; Pribor and Dinwiddie, 1992; Waller, 1992; Waller et al., 1993) and war veterans (Striegel-Moore et al., 1999).
Among female OCD patients, eating disorder comorbidity estimates have ranged from 11% to 42% depending on the type of eating disorder and the method of assessment (Bulik, 1995). Fahy et al. (1993) found that 11% of their OCD patients also had comorbid AN. Brewerton et al. (1993) reported that 20% of women with social phobia met the criteria for an eating disorder. Lipschitz et al. (1999) found 25% of adolescent mixed-gender PTSD inpatients met the criteria for an eating disorder. Wittchen et al. (1999) investigated rates of social phobia and related comorbidities amongst a large mixed-gender sample. They reported significantly higher rates of eating disorders (generally EDNOS) amongst individuals with social phobia (15%) compared to those without (2.6%).
The objective of the present study was to investigate the prevalence of comorbid eating and anxiety disorders amongst an eating disorder and anxiety disorder sample using well standardised, internationally accepted measures. The researchers attempted to avoid problems with sample sourcing and selection by including only female patients and minimising exclusion criteria.
Methods
Sample
The inclusion criteria for participants with eating disorders included a current DSM-IV diagnosis of AN, BN or EDNOS, aged 18 years or over and not subject to serious medical complications resulting from their eating disorder. It should be noted that individuals presenting with a diagnosis of binge eating disorder were not included in this study. The inclusion criteria for participants with anxiety disorders included a current DSM-IV diagnosis of an anxiety disorder and aged 18 years or over.
A total of 198 women who appeared to meet study criteria were approached to participate, and of these, 152 women were recruited for this study. The subsequent sample represents 76.8% of patients who were approached to participate. There were several reasons for excluding individuals from the study including not providing consent to participate (n = 43), incorrect completion of questionnaires (and unable to contact the individual) (n = 1) and a diagnosis of binge eating disorder (n = 2). A consort diagram (Figure 1) details the flow of participants throughout the study.
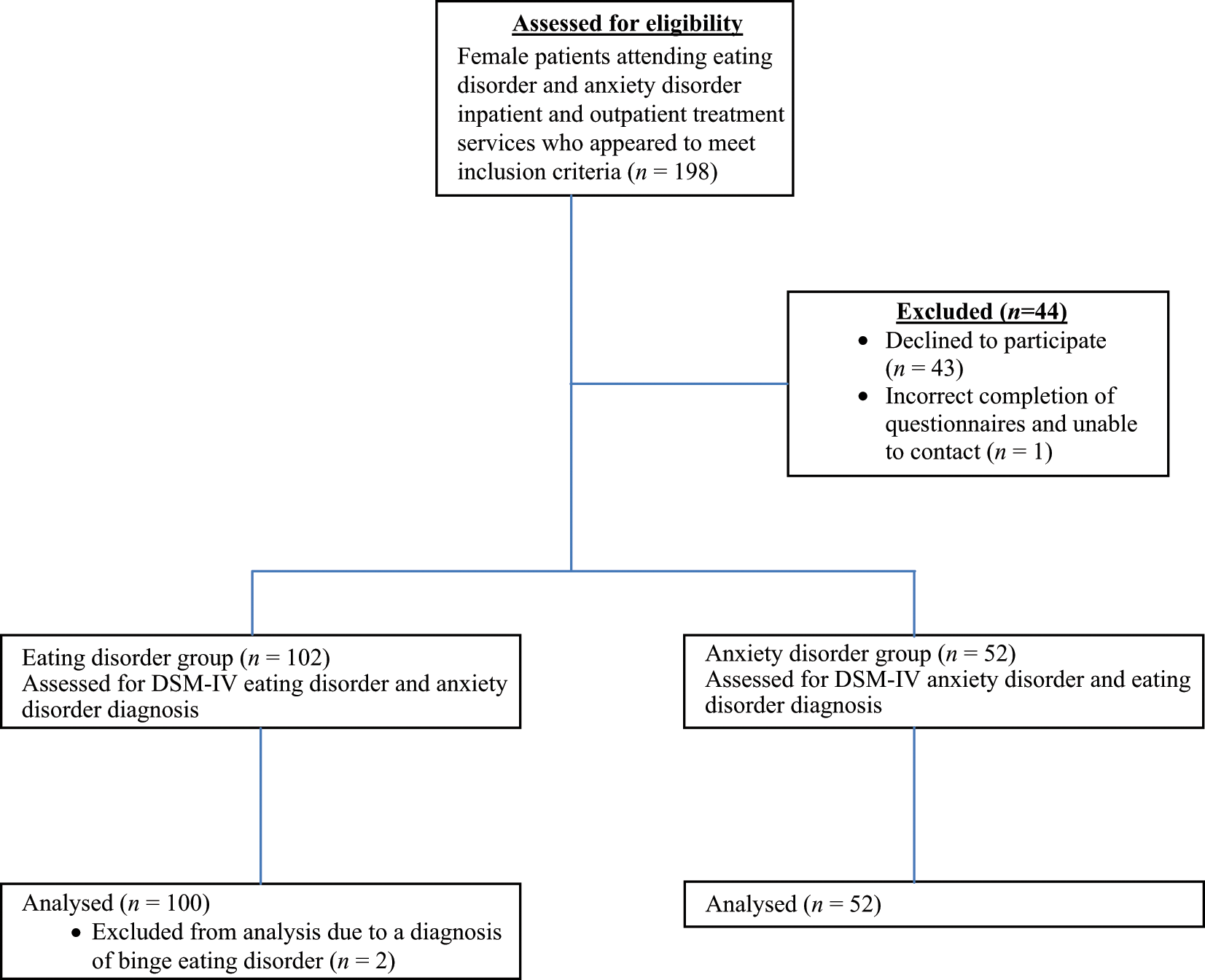
Consort diagram.
Eating disorder sample
A total of 136 women presenting for treatment of an eating disorder who met the inclusion criteria were invited to participate in this study. Of these, 100 female participants agreed to participate in this study and the subsequent sample represents 73.5% of patients who were approached to participate. The sample included 50 inpatients from two university teaching hospitals and 50 outpatients from two day treatment programs (29 patients), a university psychology clinic (16 patients) and private psychiatry/ psychology (5 patients) treatment services.
Anxiety disorder sample
A total of 62 consecutive female patients entering the Anxiety Treatment and Research Unit of the Sydney West Area Health Service and the University of Sydney Psychology Clinic who met a current DSM-IV diagnosis of an anxiety disorder and were aged 18 years or over were approached to participate in the current study. Of these, 52 anxiety disorder outpatients agreed to participate in this study, representing 84% of patients who were approached to participate.
All 52 female participants met DSM-IV criteria for an anxiety disorder: 28.8% (n = 15) for social phobia, 23.1% (n = 12) for OCD, 17.3% (n = 9) for GAD, 17.3% (n = 9) for panic with agoraphobia, 5.8% (n = 3) for specific phobia, 5.8% (n = 3) for PTSD and 1.9% (n = 1) for ASD. Secondary anxiety diagnoses were diagnosed in 25% (n = 13) of the participants.
Ethical approval
Ethics was granted by the University of Sydney Human Research Ethics Committee, the South West Sydney Area Health Service Human Research Ethics Committee and the South West Sydney Area Health Service Scientific Advisory Committee and Northside Clinic.
Assessment instruments
Eating Disorder Examination (EDE; Cooper and Fairburn, 1987; Fairburn and Cooper, 1993). The EDE is a standardised, investigator-based interview for the assessment of eating disorders (Garner, 1995). It investigates the frequency of key behavioural and attitudinal aspects of eating disorders during the preceding 28 days. The EDE evaluates the major areas of eating disorder psychopathology on four subscales: Restraint, Eating Concern, Shape Concern and Weight Concerns. Inter-rater reliability for the global EDE score has been estimated to be 0.97–0.99 (Wilson and Smith, 1989). Furthermore, the four subscales have good discriminant validity in distinguishing between individuals with eating disorders and controls (Fairburn and Cooper, 1993; Fairburn and Beglin, 1994). The Weight and Shape Concern subscales also have good discriminant validity in distinguishing between individuals with eating disorders and restrained eaters (Wilson and Smith, 1989). The EDE was used to evaluate the eating disorder specific psychopathology and to elicit the clinical DSM-IV eating disorder diagnoses. The researcher [JS] was trained in the use of the EDE, and conducted all EDE interviews. The EDE was used to evaluate the eating disorder specific psychopathology and to elicit the clinical DSM-IV eating disorder diagnoses.
Eating Disorder Examination – Questionnaire (EDE-Q; Fairburn and Beglin, 1994). The EDE-Q is a self-report version of the EDE (Cooper and Fairburn, 1987; Fairburn and Cooper, 1993) and assesses attitudinal and behavioural aspects of eating disorders, over a 28-day period. The EDE-Q consists of the same four subscales as the EDE, including Shape Concern, Weight Concern, Dietary Restraint and Eating Concern. The EDE-Q yields scores on each of these subscales as well as a Total Scale score. These subscales have demonstrated excellent test–retest reliability over a 2-week period with coefficients ranging from 0.81 to 0.94 (Luce and Crowther, 1999). It also contains items enabling the assessment of binge eating and compensatory behaviours in terms of the number of days each behaviour occurred and the number of distinct episodes on each day. The EDE-Q appears to be useful as a screening measure for eating disorder pathology, and its generally good convergent validity with the EDE suggests that it may be used as a substitute for the EDE (Fairburn and Beglin, 1994). Nevertheless, given that it may indicate a higher frequency of problematic eating disorder symptoms, it was decided that this measure alone would not be utilised to identify eating disorder diagnoses. Subsequently, this measure was purely used to identify any eating disorder pathology, and where indicated, the EDE was then utilised to confirm diagnoses.
Eating Attitudes Test (EAT-40; Garner and Garfinkel, 1979). The EAT-40 has three subscales: Dieting, Bulimia and Food Preoccupation, and Oral Control, which are highly correlated with each other (Garner et al., 1982). This measure was originally developed to assess attitude and behaviour characteristics of individuals with AN. It not only discriminates AN samples from controls, it also discriminates BN samples from control groups (Gross et al., 1986). The EAT-40 was administered with the EDE-Q to screen for possible eating disorder pathology in women presenting for anxiety treatment. By administering the EDE-Q and EAT-40 together, both of which demonstrate sound psychometric properties, it was thought that this would reduce the likelihood of missing potential eating disorder cases amongst participants.
Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV; Brown et al., 1994). The ADIS-IV is a semi-structured clinician-administered interview designed to assess all DSM-IV anxiety disorders and commonly comorbid disorders, and has demonstrated good levels of diagnostic reliability (Grisham et al., 2004). The ADIS was used to elicit the DSM-IV anxiety disorder diagnoses for all participants.
Depression Anxiety and Stress Scale (DASS-21; Lovibond and Lovibond, 1995). The DASS-21 is the short form of Lovibond and Lovibond’s 42-item measure of depression, anxiety and stress. There is evidence the DASS scales do constitute valid measures of the constructs they were intended to represent (Crawford and Henry, 2003; Henry and Crawford, 2005; Lovibond and Lovibond, 1995). The DASS-21 has a number of advantages over the full-length DASS. As it is shorter than its full length counterpart, it is more acceptable for clients, whilst still demonstrating adequate reliability and omits items from the full DASS that have been identified as problematic (Henry and Crawford, 2005). The DASS was used to provide an indication of depressive symptomatology.
Sociodemographic questionnaire. This included date of birth, ethnic origin, marital status, number of children, occupational history, education level and medications of each participant, and was completed on assessment.
Height and weight measurements. For eating disorder participants, height and weight measurements were taken from clinical records upon entry into treatment and used to calculate body mass index (BMI). Anxiety disorder participants provided their height and weight measurements at the time of assessment in order for the researcher [JS] to calculate BMI.
Diagnostic procedure
All eating disorder participants who were invited to participate were assessed for current eating disorder and anxiety disorder diagnoses. Assessment involved the primary researcher [JS] conducting all EDE and ADIS-IV (anxiety disorders section only) interviews. Participants also completed a sociodemographic questionnaire and the DASS-21.
To screen for eating disorder symptomatology amongst anxiety participants, two eating disorder self-report questionnaires were completed (the EDE-Q and the EAT-40). Based on the eating disorder self-report measures, participants obtaining scores indicative of eating disorder pathology were invited back for a more comprehensive eating disorder assessment using the EDE.
All participants received detailed information about the procedures and aims of the study, and gave written consent.
Statistical analyses
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS, 2006) for Windows (Version 15.0). Significant mean group differences for parametric variables were analysed using t-tests and one-way analysis of variance (ANOVA) statistical procedures. In place of t-tests, Mann-Whitney tests were conducted in cases where the t-test normality assumption was violated (determined by skewness and kurtosis) and sample sizes were small. Chi-square (χ2) tests for categorical independent variables were also conducted. Furthermore, Fisher’s exact test was used when the minimum expected cell size was five or less and Craméres V was used when independent variables had more than two categories. For all statistical analyses reported, the alpha was set at p < 0.05, unless otherwise indicated.
Results
Eating disorder sample
One of the primary aims of this study was to investigate the prevalence of comorbid anxiety disorders amongst an inpatient and outpatient eating disorder sample. This aim included establishing which of the anxiety disorders were most prevalent, the temporal relationship between the disorders, and any differences in clinical characteristics between individuals with comorbid anxiety disorders and those without. These results have been summarised and presented in Figures 2 and 3 and Tables 2 - 5 for the inpatient and outpatient eating disorder samples.
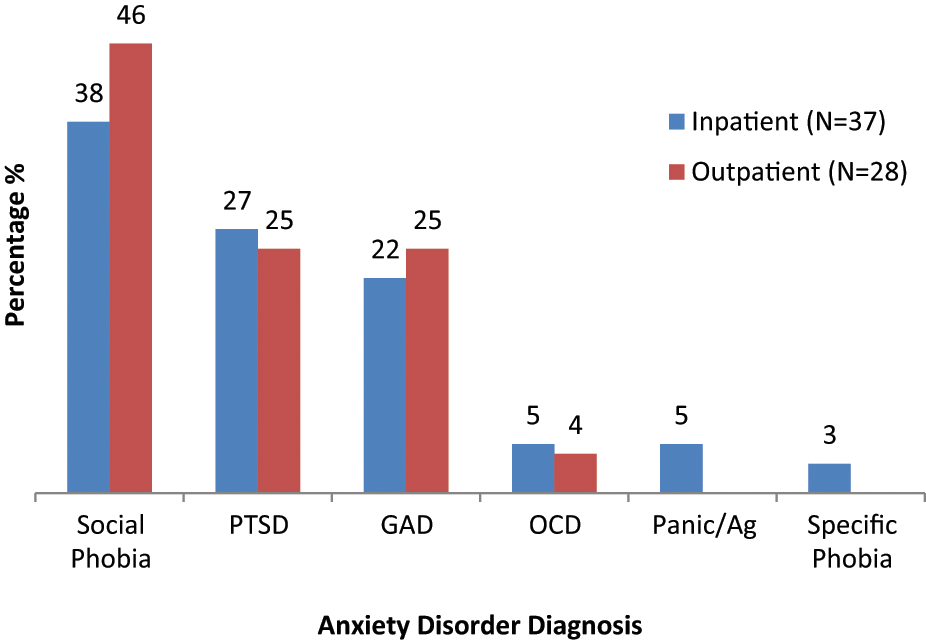
Prevalence (%) of primary anxiety disorders diagnosed across the inpatient eating disorder and outpatient eating disorder comorbid sample.
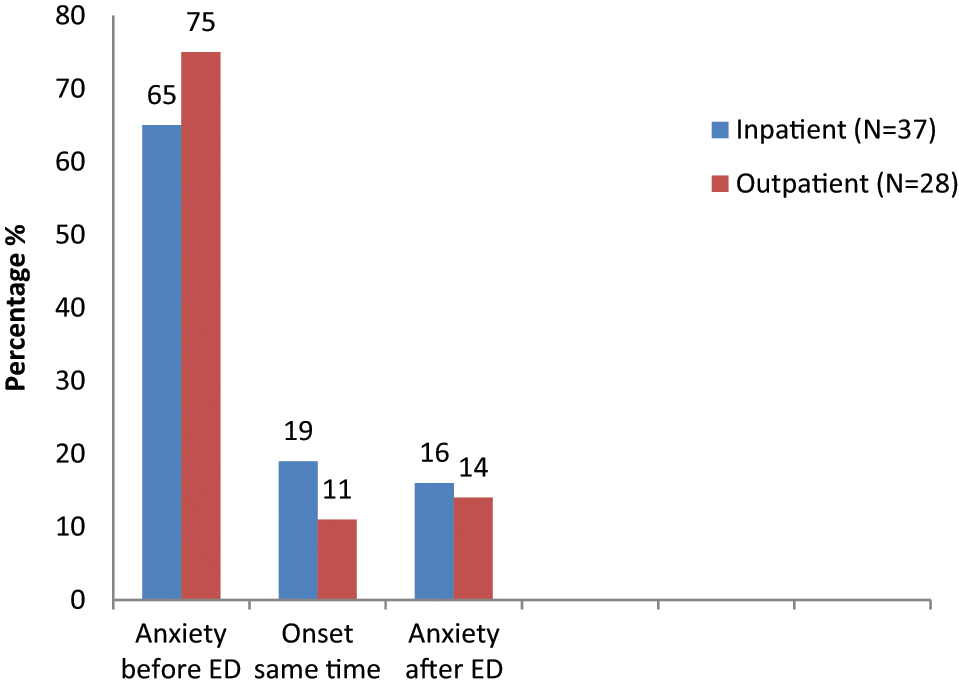
Reported temporal relationship between eating disorder and anxiety disorder onset across the inpatient eating disorder and outpatient eating disorder comorbid sample.
Demographic and clinical characteristics of the eating disorder and anxiety disorder participants
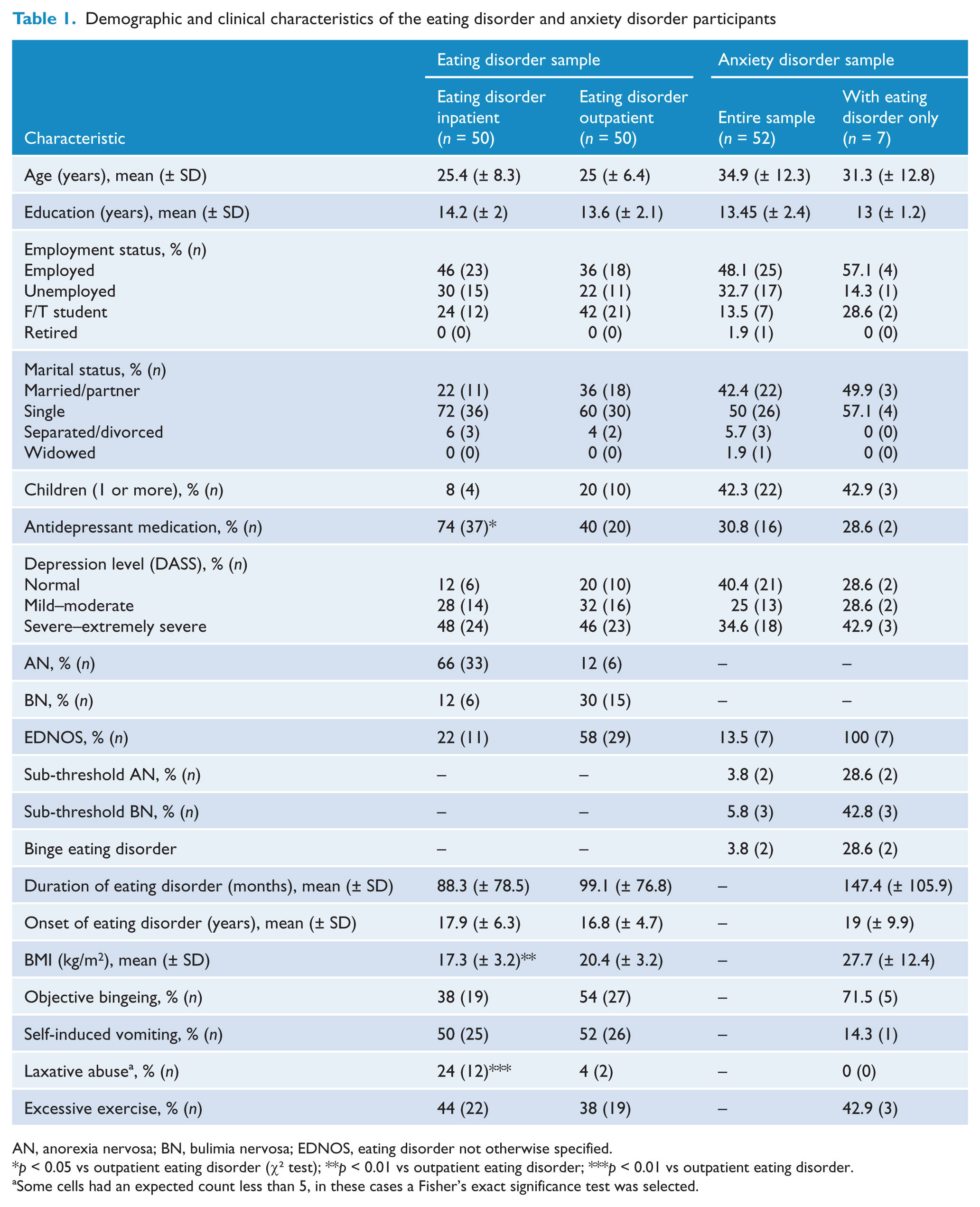
AN, anorexia nervosa; BN, bulimia nervosa; EDNOS, eating disorder not otherwise specified.
p < 0.05 vs outpatient eating disorder (χ2 test); **p < 0.01 vs outpatient eating disorder; ***p < 0.01 vs outpatient eating disorder.
Some cells had an expected count less than 5, in these cases a Fisher’s exact significance test was selected.
Current prevalence of anxiety disorders across the inpatient eating disorder sample
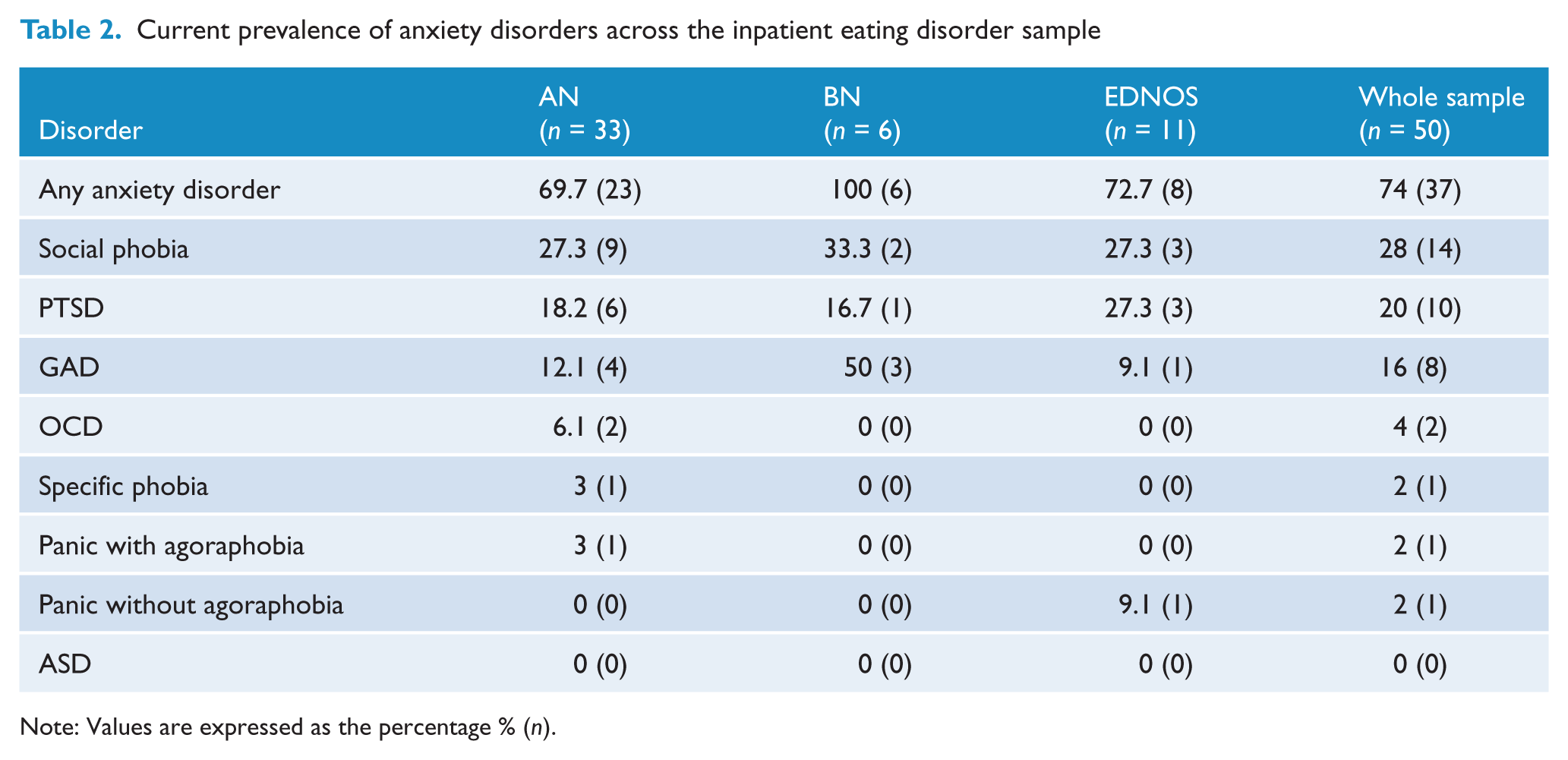
Note: Values are expressed as the percentage % (n).
Summary of clinical characteristics of comorbid eating disorder and eating disorder only group across the inpatient sample (N = 50)
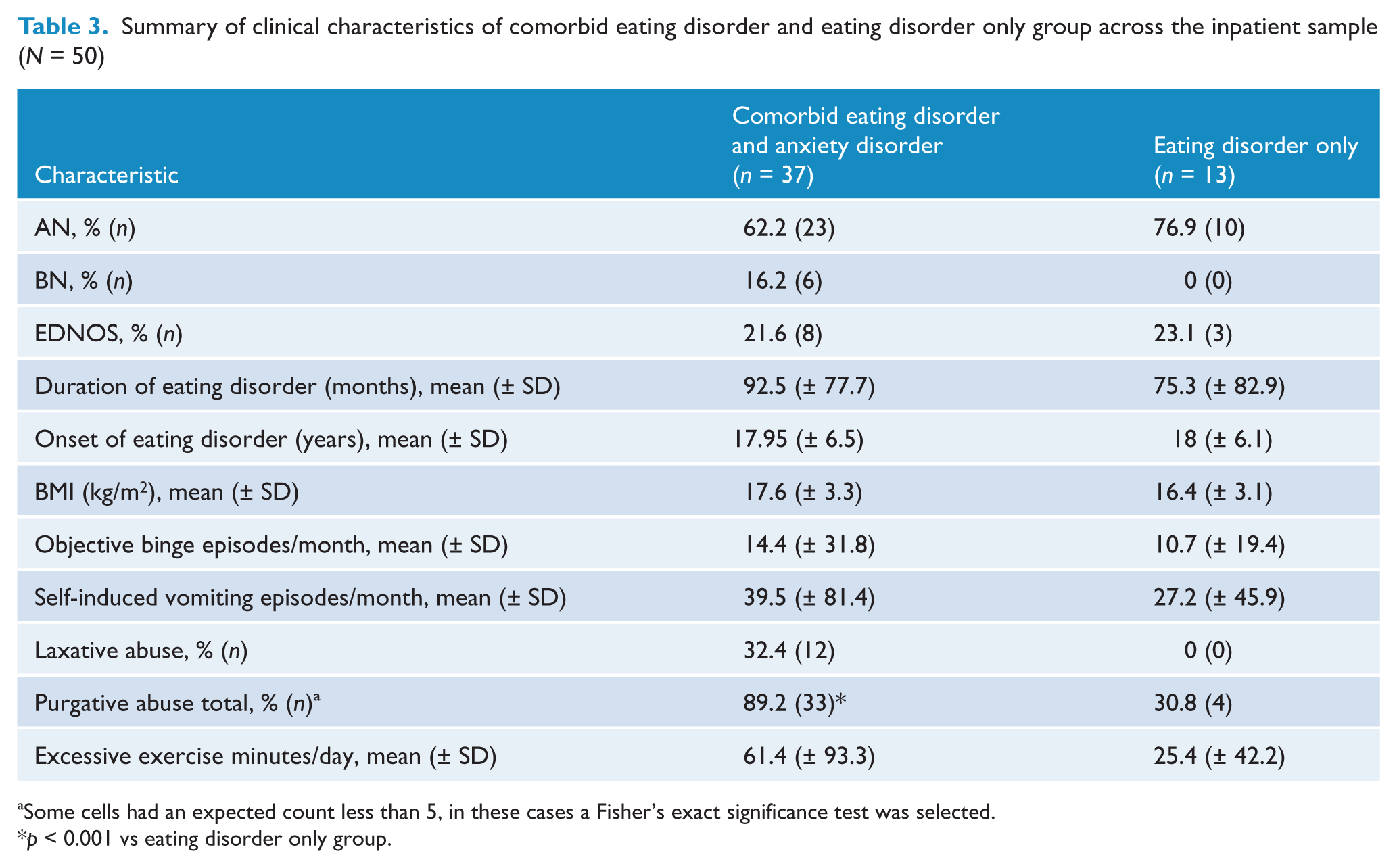
Some cells had an expected count less than 5, in these cases a Fisher’s exact significance test was selected.
p < 0.001 vs eating disorder only group.
Current prevalence of anxiety disorders across the outpatient eating disorder sample
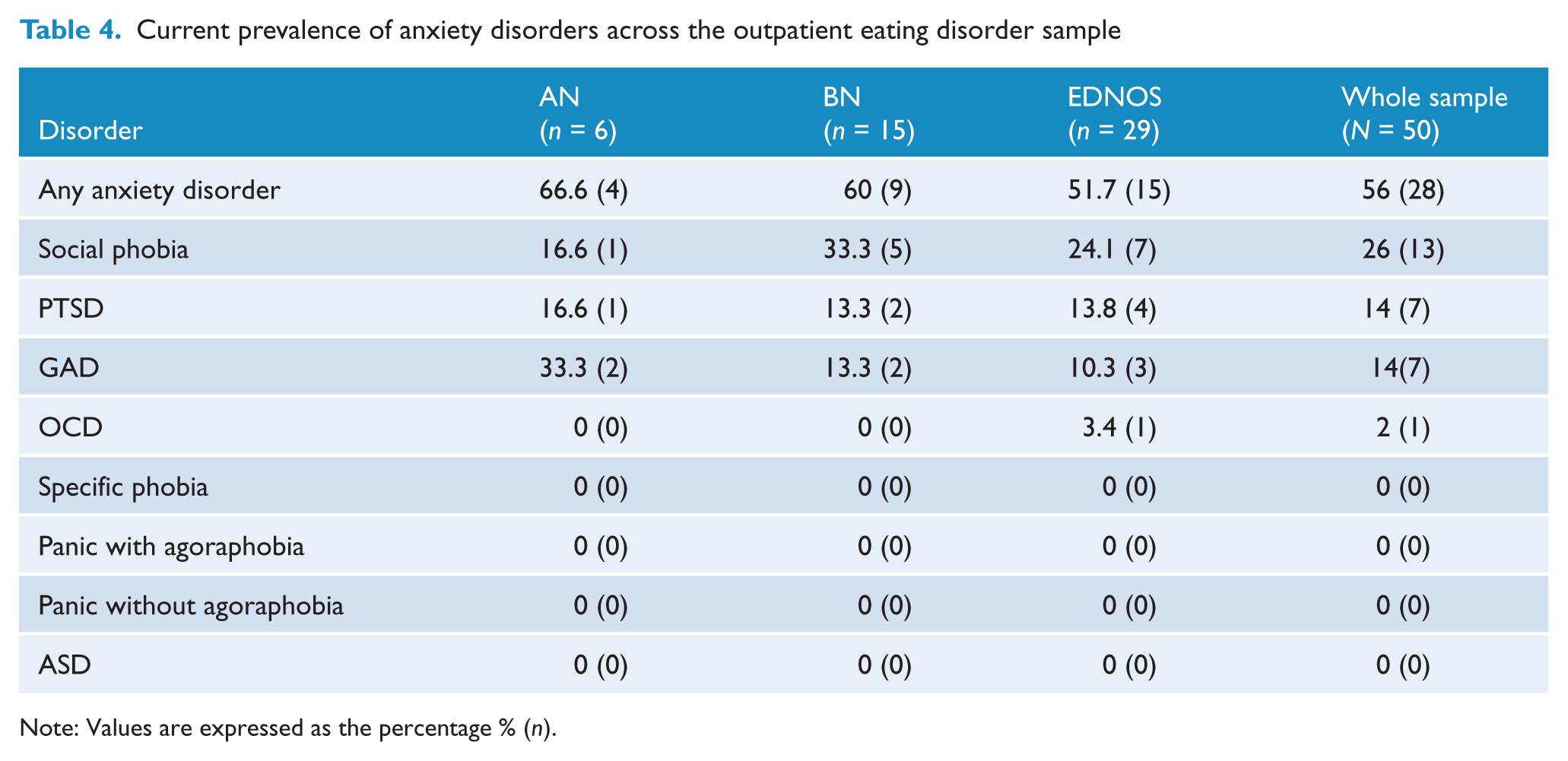
Note: Values are expressed as the percentage % (n).
Summary of clinical characteristics for the comorbid eating disorder and eating disorder only groups across the outpatient sample (N = 50)
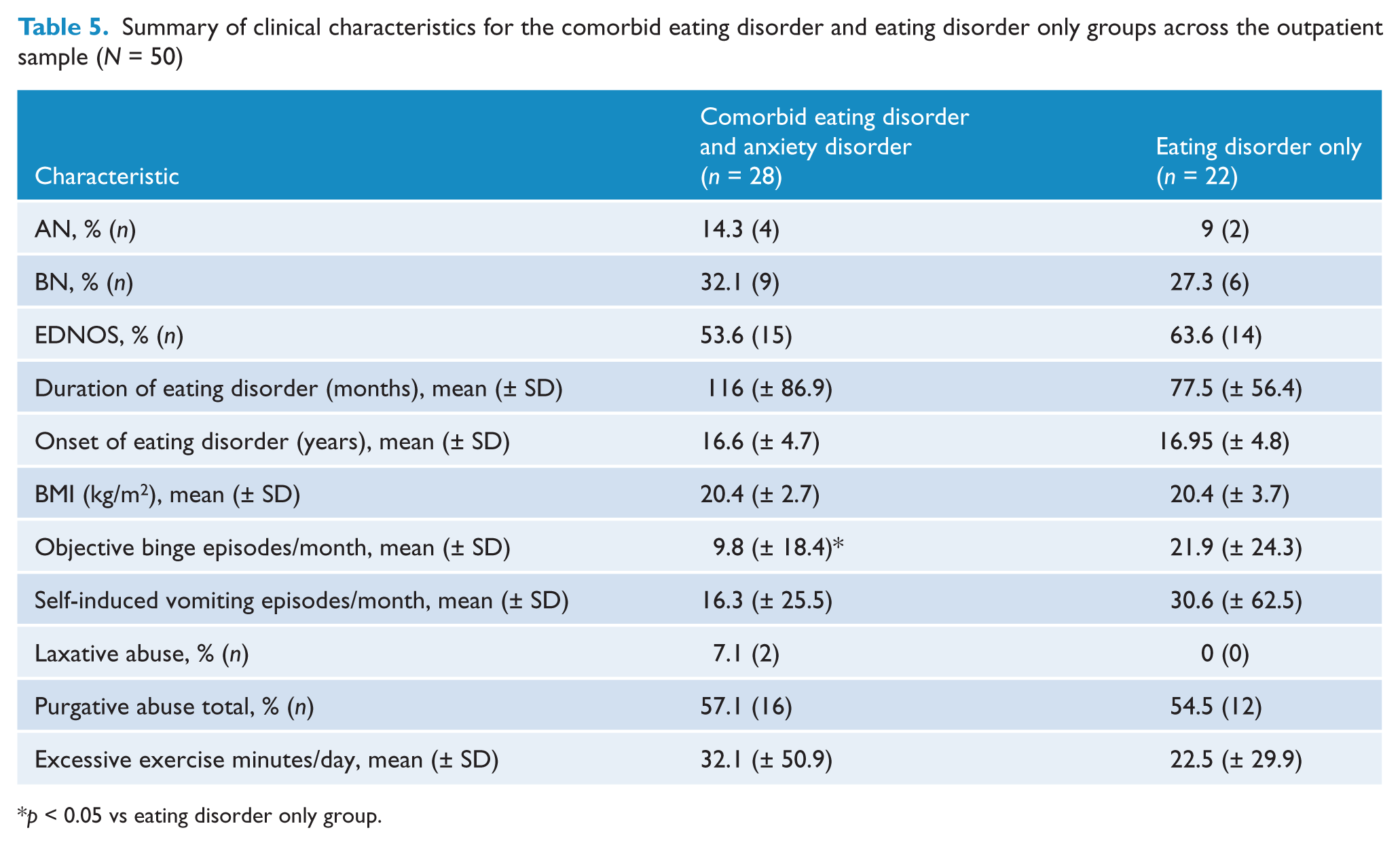
p < 0.05 vs eating disorder only group.
Anxiety disorder sample
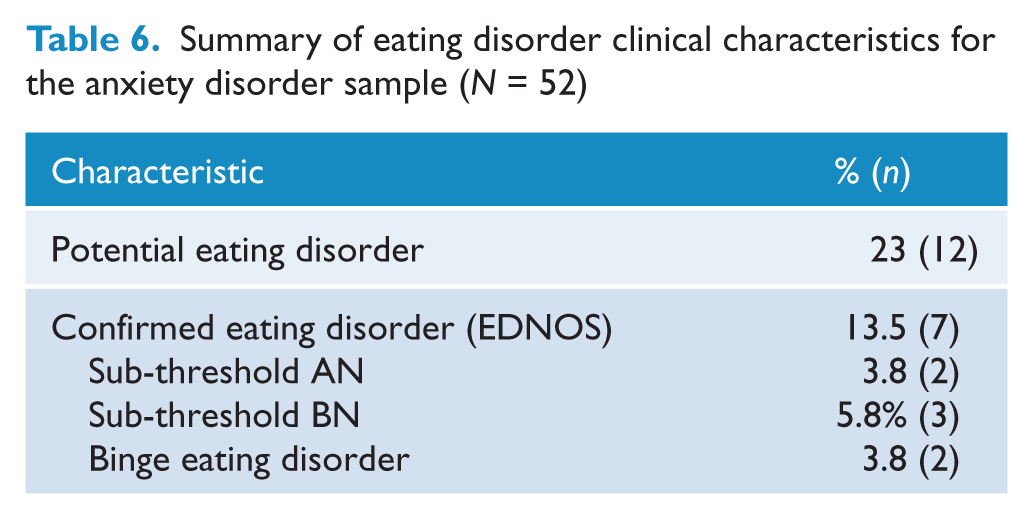
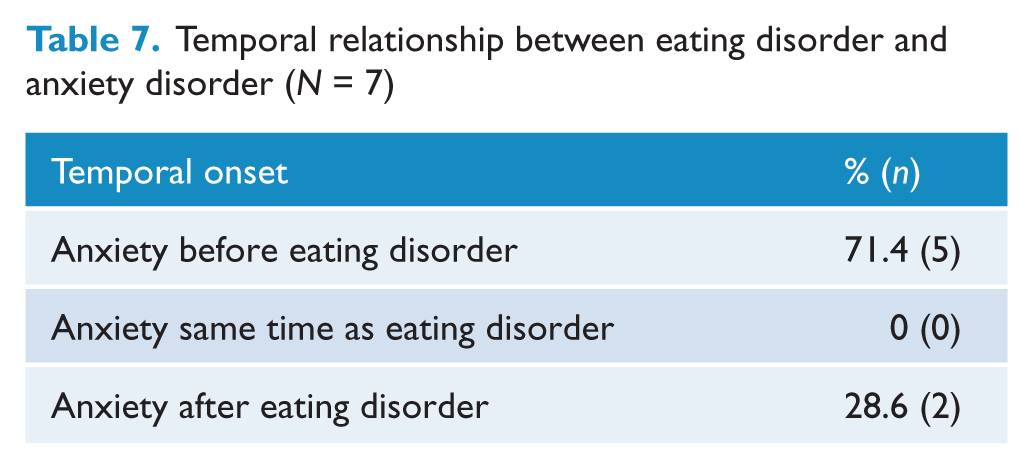
Another objective of this study was to investigate the prevalence of comorbid eating disorders amongst an anxiety disorder sample. This aim included identifying which of the eating disorder subtypes was most prevalent, the temporal relationship between the onset of the comorbid disorders as well as any differences in clinical characteristics between individuals with comorbid eating disorders and those without. These results have been summarised and presented in Tables 1, 6 and 7. It should be noted that three participants identified as having a potential eating disorder were unable to complete a further eating disorder assessment to confirm diagnosis. Two of these participants were unable to be contacted, and the other declined to participate in a further interview. For the 3 participants diagnosed with subthreshold BN, 2 participants met all criteria for BN met except binge eating and compensatory behaviour occurred less than twice a week and the third participant repeatedly engaged in chewing and spitting large amounts of food without swallowing. The 2 participants with subthreshold AN met all criteria for AN except both had a BMI higher than 17.5. The primary anxiety disorders for which participants with comorbid eating disorders sought treatment included OCD (n=3), social phobia (n=1), GAD (n=1), Specific Phobia (n=1) and PTSD (n=1).
Regarding secondary diagnoses, there was only 1 participant who was diagnosed with a secondary anxiety disorder (primary OCD and secondary GAD). There were no cases of subthreshold anxiety disorders identified in the comorbid anxiety and eating disorder group. The experience of at least 1 trauma was reported by 3 of the participants, however in only 1 of these cases was a diagnosis of PTSD met.
Summary of eating disorder clinical characteristics for the anxiety disorder sample (N = 52)
Temporal relationship between eating disorder and anxiety disorder (N = 7)
Discussion
Our findings confirm the high prevalence of anxiety and eating disorders amongst both inpatient and outpatient eating disorder samples, and across all eating disorder subtypes. The results are consistent with previously published research in this area, notwithstanding the methodological limitations inherent in many of these studies. We found 74% of our inpatient eating disorder sample and 56% of our outpatient eating disorder sample met criteria for at least one anxiety disorder. Across the entire eating disorder sample, 65% met criteria for at least one anxiety disorder.
In relation to the rates of eating disorder pathology amongst the outpatient anxiety sample, 13.5% of the sample met criteria for EDNOS. It must be noted that this rate may be an underestimate as three participants identified as having potential eating pathology were unable to be assessed further. Unfortunately there is not a comparable Australian sample with which to compare these rates. However, our findings are comparable to the 12% of probable eating disorder cases reported by Black Becker et al. (2004).
Although a greater prevalence of anxiety disorders amongst the inpatient eating disorder sample compared with the outpatient sample was anticipated, the difference was not significant. Furthermore, the inpatient and outpatient samples did not differ significantly except in regards to reported antidepressant medications (higher in the inpatient sample), BMI (lower in the inpatient sample) and laxative abuse (greater in the inpatient sample). These differences are not surprising given the well-documented observations that inpatient eating disorder samples have a greater severity of symptoms than outpatient samples. Although depression scores were not significantly different between the inpatient and outpatient samples, this may be explained by the fact that the inpatient sample reported a higher frequency of prescribed antidepressant medications than the outpatient sample, thus perhaps reducing their depression scores in the preceding 7 days. However, as a clinical assessment for a mood disorder was not conducted, prevalence of comorbid depression could not be confirmed across the sample. It should also be noted that the high use of antidepressant medication observed in the eating disorder samples may have led to a reduction in the reporting of anxiety symptoms and subsequent diagnosis of anxiety disorders. This is based on the results from research supporting the efficacy of SSRIs and tricyclic antidepressants in the treatment of anxiety disorders as well as comorbid anxiety and depressive disorders (Feighner, 1999).
In terms of anxiety disorder diagnoses, 65% of the entire eating disorder sample (74% of the inpatient eating disorder sample and 56% of the outpatient eating disorder sample) met DSM-IV criteria for a current primary DSM-IV anxiety disorder diagnosis. Similar rates of anxiety disorders were also observed across all the eating disorder subtypes (69% of the AN sample, 71% of the BN sample and 57.5% of the EDNOS sample). It is important to note that our diagnoses excluded any possible anxiety symptoms related to the eating pathology (e.g. a fear of eating and drinking in public in the case of social phobia; excessive, uncontrollable worry related to food, weight or shape in the case of GAD; panic symptoms related to food, weight or shape concerns).
Regarding the temporal onset of anxiety disorders, the majority of the sample (65% of inpatients and 75% of outpatients) reported the onset of the anxiety disorder to precede the onset of the eating disorder, and there were no significant differences between the subtypes. These results are commensurate with other studies investigating the temporal relationship between eating disorders and anxiety disorders (Brewerton et al., 1995; Bulik et al., 1996; Godart et al., 2000; Toner et al., 1988).
As predicted, the prevalence of social phobia was particularly high across the entire sample (42%) and across all eating disorder subtypes. In fact, it was the most commonly diagnosed anxiety disorder across the entire sample (inpatient 38%; outpatient 46%) and all eating disorder subtypes (AN 26%; BN 33%; EDNOS 25%). Our findings for AN are on a par with those reported by Laessle et al. (1987, 1989), Herpertz-Dahlman et al. (1996) and Kaye et al. (2004) and for BN are consistent with social phobia rates reported by Laessle et al. (1987) and Bulik et al. (1996).
The diagnosis of PTSD was also particularly high across the entire sample (26%), with just over a quarter of inpatients (27%) and 25% of the outpatients meeting criteria. Rates for PTSD across the eating disorder subtypes were also comparable (AN 18%; BN 14%; EDNOS 17.5%). This finding is particularly interesting given that PTSD has so frequently been excluded from previous studies. Furthermore, this prevalence rate is likely to be an underestimate of the true rates of PTSD, given that almost 19% of women who reported having experienced a trauma were unable to continue the assessment due to their distress. Notwithstanding the few available studies investigating PTSD in eating disorder samples, our findings are comparable to those PTSD rates reported by Turnbull et al. (1997).
The diagnosis of GAD was also high amongst the entire eating disorder sample (23%), with fairly similar rates being reported across the inpatient (22%) and outpatient (25%) samples and eating disorder subtypes (AN 15%; BN 24%; EDNOS 10%). Our findings for GAD amongst our AN and BN sample are slightly higher than those reported by Kaye et al. (2004), however our findings for the EDNOS sample were comparable to that study.
Interestingly, we found relatively low rates of panic disorder with and without agoraphobia across the entire eating disorder sample (3% AN, 0% BN) compared with the 7% (AN) and 15% (BN) reported by Godart et al. (2000). Our findings are comparable to those reported by Lilenfeld et al. (1998) of 4% across their AN and BN sample. Although many subjects initially reported experiencing panic attacks, upon further questioning most denied a fear of the symptoms or of future panic attacks, as would be expected for a diagnosis of panic disorder. Furthermore, agoraphobia was not diagnosed if fears were specific to food-related situations (supermarkets, food courts, etc.) in the absence of fear about the physiological arousal symptoms.
Similarly low rates of specific phobias were reported across the entire sample (2%), which was surprising given the previously reported rates of between 12% and 45% for AN and 12% and 46% for BN (Godart et al., 2000; Hudson et al., 1983; Laessle et al., 1987; Lilenfeld et al., 1998). Our findings were comparable to those of an earlier study by Piran et al. (1985), which found rates of phobias of 0–3% across their AN and BN sample.
In contrast to a number of previous studies reporting high rates of eating disorder samples, we found only 5% of our entire eating disorder sample met criteria for OCD. OCD rates did not differ significantly across inpatient (5%) and outpatient (4%) samples. Most of the OCD cases were identified in the AN group (5%) and there was one diagnosis of OCD in the EDNOS sample. Interestingly, we did not find a single case of OCD amongst the inpatient or outpatient BN sample. Previous studies have reported rates of OCD for AN of 9.5–69% (Fornari et al., 1992; Godart et al., 2000, 2003; Hudson et al., 1983; Iwasaki et al., 2000; Kaye et al., 2004; Laessle et al., 1987, 1989; Milos et al., 2002; Piran et al., 1985; Speranza et al., 2001; Thornton and Russell, 1997), however our reported rate for AN is lower still. Furthermore, when considering the rate of OCD amongst AN (37%) reported in another Australian study (Thornton and Russell, 1997) with a similar AN sample size, our rates appear extremely low. It should be noted that four of these aforementioned studies (Godart et al., 2003; Kaye et al., 2004; Iwasaki et al., 2000; Milos et al., 2002) have a much larger AN sample than our study, which could certainly account for the discrepancy in OCD rates. Another possibility is that some studies may have over-diagnosed rates of OCD, perhaps including obsessive and compulsive symptoms that are related to eating disorder pathology as opposed to true OCD diagnoses.
Our findings for OCD prevalence rates amongst our BN and EDNOS sample are comparable to the lowest rates presented in previous studies. Studies investigating the prevalence of OCD amongst BN samples have reported between 0% and 44% (Fornari et al., 1992; Godart et al., 2000; Hudson et al., 1983; Kaye et al., 2004; Laessle et al., 1987, 1989; Lilenfeld et al., 1998; Milos et al., 2002; Piran et al., 1985; Speranza et al., 2001; Thornton and Russell, 1997).
In terms of age of onset of comorbid disorders, the average age of onset for the anxiety disorders in the inpatient sample was 15 years compared with almost 18 years for the onset of the eating disorder pathology. This was slightly lower for the outpatient sample, with the average age of onset for the anxiety disorder being 12 years compared with almost 17 years for the onset of the eating disorder pathology. There was no significant difference between age of onset for anxiety disorder pathology for each of the specific anxiety disorders across the inpatient and outpatient samples.
Finally, we found that significantly more of the inpatient comorbid eating disorder and anxiety sample reported purgative abuse than the eating disorder only sample. This is consistent with previous findings confirming increased vomiting (Carter and Duncan, 1984) and laxative abuse (Weltzin et al., 1995) amongst individuals with comorbid anxiety and eating pathology. Furthermore, across the entire eating disorder sample, the mean number of reported episodes of excessive exercise was higher in the comorbid eating disorder and anxiety group than in the eating disorder only group. Although there is an absence of research into the use of excessive exercise amongst individuals with eating disorders and comorbid anxiety disorders, one might hypothesise that exercise could be used in a similar manner to other avoidance or self-harm behaviours, which enable an individual to regulate affect.
Surprisingly, amongst the outpatient sample a greater number of reported episodes of objective binge eating was found in the eating disorder only sample compared with the comorbid anxiety and eating disorder group. Although this difference only just met significance, it is nevertheless surprising given the literature suggesting that increased levels of bingeing behaviour have been observed in individuals with comorbid anxiety.
Limitations and strengths of the current study
There are several limitations that can be raised regarding the current research. Firstly, it should be noted that the current study utilises a clinical sample, and as such, comorbidity may be over-represented. Du Fort et al. (1993) cited the phenomenon of Berkson’s Bias, whereby individuals with comorbid diagnoses are more likely to seek treatment than those with a single diagnosis. Nevertheless, there is a clear need for research investigating comorbidity amongst eating disorder and anxiety disorder samples in order to ensure further improvements in the assessment and treatment of these disorders.
Inherent to the design of the current study is the retrospective diagnostic procedure used to provide the time of onset for clinically significant anxiety and eating disorders. The obvious problems with this procedure, as noted in many previous studies, is the memorisation biases that may have affected the ability of someone to recognise the symptoms of a disorder and recall the time of onset (Godart et al., 2000). Furthermore, as discussed in previous research, there are difficulties associated with interpreting the appearance chronology of anxiety and eating pathology (Godart et al., 2000).
The researchers also chose to report the age at onset as the age at which all criteria for DSM-IV anxiety or eating disorders were met. In some cases, individuals may have demonstrated sub-threshold diagnoses at earlier ages. Furthermore, the present study investigated only the current diagnoses of eating and anxiety pathology. An investigation of lifetime diagnoses may have yielded higher prevalence rates.
Although the DASS was administered to assess for depressive symptomatology, we did not formally assess for the presence of a comorbid mood or substance use disorder with the ADIS-IV. Both of these disorders are clearly implicated in the eating disorders, and have been widely studied in this population. Given the already lengthy assessment process involved in the present study, the addition of these sections of the ADIS-IV to confirm mood and substance disorders may have been too great a burden on participants. Nevertheless, this is clearly a limitation of the present study.
As criticisms of previous studies have stemmed from the exclusion of certain anxiety disorders when investigating comorbidity amongst the eating disorders, this study set out to include all DSM-IV diagnoses regardless of frequency of presentation. We found that 13.5% of women presenting for anxiety disorder treatment also met criteria for a current eating disorder, and their primary anxiety diagnoses included all DSM-IV disorders except for panic disorder, agoraphobia and acute stress disorder. A limitation, however, is the small number of participants with comorbid eating and anxiety disorders in each of the specific anxiety disorder groups. This precluded tests of effects within individual diagnostic categories, thus limiting the ability to compare and draw conclusions. Indeed overall, the sample size is a limitation, especially with regards to the small cell size when dividing by individual anxiety disorders.
A significant strength of the current study is that, to the best of the authors’ knowledge, it is the first study of its kind to be conducted on an Australian clinical population. In contrast to previous research, all anxiety disorders were thoroughly investigated across all eating disorder subtypes. Furthermore, the use of well standardised, internationally accepted diagnostic instruments for the assessment of anxiety and eating pathology is also a significant strength, as it has avoided the methodological limitations of previous research failing to employ adequate assessment measures.
The few exclusion criteria the present research employed in recruitment of participants was also a significant strength. All patients who were well enough to attend the assessment were included in this study. Consequently, the current sample provides a good representation of the type of patients treated in eating disorder and anxiety disorder units. The less stringent exclusion criteria used in this study will increase the clinical efficacy of the current results.
Directions for future research
The findings of the current study raise important questions regarding the aetiological and prognostic factors associated with eating disorders, which should be addressed in future research.
Our study has raised the possibility that the diagnosis and treatment of anxiety pathology in patients with eating disorders may be crucial for successful treatment of the eating pathology. In order to address this, future studies should focus on investigating treatment response amongst individuals with comorbid anxiety and eating disorders. Of particular interest is whether individuals have better treatment outcomes when treatment includes addressing both eating and anxiety disorders, compared with treatment focusing on the eating pathology alone. Furthermore, research should also follow up patients to assess anxiety symptoms over time and post treatment.
Future research should aim to further investigate PTSD and eating disorder comorbidity, examining the type of trauma experienced, to investigate whether certain types of trauma are more likely to be associated with eating pathology. Furthermore, it would be of particular interest to examine the possibility that certain eating disorder behaviours (such as bingeing and purging) are used to regulate affect, or as a coping strategy for anxiety symptoms, such as intrusive memories.
In addition to the suggestions above, it is clear from the current study that anxiety disorders are prevalent across the full spectrum of eating disorders. Given the more recent emphasis on transdiagnostic approaches to the treatment of eating pathology, further research investigating anxiety presentations irrespective of eating disorder diagnosis may assist in broadening our current understanding of comorbidity between anxiety and eating disorders.
The current study has highlighted that eating pathology may be common in women presenting for treatment of anxiety disorders. It is clear from the current research that eating pathology and anxiety disorders often co-occur and therefore, eating pathology must also be assessed in order to adequately formulate and provide treatment for the individual presenting for anxiety treatment. Consequently, it is recommended that all future assessments of anxiety disorders include screening for eating disorder pathology. Given that the ADIS-IV does not include an assessment for eating pathology, it may be useful to follow Black Becker et al. (2004) and incorporate a skip-out condition on the EDE-Q to reduce the burden on patients. It is noted that the EDE-Q demonstrates high sensitivity and specificity for detecting eating disorder case status (Black Becker et al., 2004) suggesting that the use of the EDE-Q, which is a relatively time-efficient self-report questionnaire to complete, may be useful as a screening measure for eating disorder pathology.
Given the previously cited limitation raised in relation to the sample size of the anxiety disorder group, future research should replicate this study with larger sample sizes. Increasing the sample size in each of the specific anxiety disorder groups would enable tests of effects within individual diagnostic categories to be carried out, therefore allowing researchers to draw comparisons.
Finally, our study has indicated the importance of using standardised structured assessment instruments to thoroughly investigate the prevalence of anxiety and eating disorder comorbidity. Questions have clearly been raised regarding the methodological limitations inherent in previous research and the possibility that this has resulted in distorted prevalence rates, in particular amongst certain anxiety disorders. Future research should avoid these limitations by only using sound methodological procedures and instruments. Having consistent standards across studies will improve the ability to compare results across studies, thus improving clinical understanding of this important area.
Conclusion
To the best of the authors’ knowledge, the current research is the only Australian study, and one of a few worldwide, to consider the prevalence of comorbid eating disorders and anxiety disorders in a treatment-seeking eating disorder and anxiety disorder population. Furthermore, this study adds to previous research in this area by using thorough assessment measures to distinguish between anxiety and eating pathology, and by considering the temporal relationship between comorbid disorders. This study adds to the clinical understanding of the comorbidity between eating disorders and anxiety disorders, highlighting the importance of screening for anxiety and eating pathology in the clinical assessment of both eating disorders and anxiety disorders, respectively.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.