
Abstract
Eating disorders are believed to have low lifetime prevalence. Large community studies of DSM-III-R and DSM-IV eating disorders in white women have found a lifetime prevalence for anorexia nervosa (AN) ranging from 1.4% to 2% [1–3] with inclusion of ‘partialsyndrome’ cases for AN resulting in overall lifetime prevalence ranging from 2% to 3.3% in the absence of amenorrhea [3, 4] to close to 4% formore broadly defined syndromes [1, 5]. The commensurate lifetime prevalence rates for bulimia nervosa (BN) range from 1.1% to 4.6% [1–3,6,7].
It has been suggested that epidemiological research in this area is hampered by the lack of empirically-based classification of eating disorders that takes into account the full spectrum of disturbance that exists in the community [8]. There are few data on the prevalence of the residual DSM eating disorder diagnosis ‘eating disorder not otherwise specified’ (EDNOS), mainly due to the lack of agreed diagnostic criteria [9]. The prevalence of the provisional DSM-IV diagnosis binge eating disorder (BED) has been estimated at 0.6% [3] and 2.7% [2]. One study investigated recurrent purging (meeting criteria for BN purging type except that objective binge eating was not present), the lifetime prevalence of which was 1.1% [3]. Previously, no difference with respect to dietary restraint or psychopathology has been found between women who purge but experience either objective binges or subjective binges [10].
Although many studies exist that examine the long-term course of eating disorders after treatment, suggesting recovery for 50% of women with AN [11], and 70% of women with BN [12], a second limitation in the epidemiological research of eating disorders has been the relative lack of studies of the natural course of eating disorders in community samples. A significant exception is the 5-year prospective study of the natural course of BN and BED that showed that the disorders have markedly different prognoses with BED showing a tendency to remit whereas BN tended to persist [13]. Very little is known about the natural course of other forms of EDNOS. Existing community studies have reported follow-up of their cohort when they are still relatively young, in their earlyto mid-20s [1, 14]. As eating disorders are still developing in early adulthood, such description of outcomes must necessarily be truncated.
The lack of knowledge about the prevalence and longterm course of the full spectrum of eating problems that exists in the community is disturbing because EDNOS cases constitute the majority of referrals to eating disorder clinics [9]. Research to date suggests that those individuals with EDNOS experience similar levels of disability, impairment and distress to individuals who meet strict criteria for threshold AN or BN [4, 10]. Thus, the purpose of the current study was twofold. The first was to investigate the lifetime prevalence of eating disorders, including EDNOS, in a large community adult female sample of twins. Second, we examined the longterm course in those women who had a lifetime eating disorder. We therefore offer a contribution to the sparse knowledge about prevalence and long-term outcome for the full spectrum of eating disorders that exists in the community.
Method
Participants
Female–female twins who had participated in at least one of two previous waves of data collection [15] were approached to participate in the present study. Written informed consent was obtained after the procedures had been fully explained. In all, 2320 twins (1140 complete pairs) were approached by the Australian Twin Registry over 2001–2003, of whom 1083 twins consented to participate (47%), 568 did not agree to participate (24%) and 669 did not respond (29%). At least one further telephone call or letter was used to contact the non-responders. This sample represents 45% of thosewomen who participated at the first wave of data collection, and 40.2% of those women who participated at the second wave. Participation at Wave 3 was not predicted by the number of eating problems at Wave 1 (t[960] = 1.00, p = 0.32), using questions that have been published previously [16]. The mean age of the women at the time of the data collection was 34.97 years (SD = 2.11), ranging from 28.10 years to 39.98 years. The total protocol consisted of two parts, a telephone interview and a self-report questionnaire. Here we report results from the interview completed by 1002 women. The Flinders Clinical Research Ethics Committee approved the data collection process.
Assessment of prevalence
The telephone interview consisted of the Eating Disorder Examination (EDE) 14th edition [17]. Thus, the assessment included questions relating to behavioural features of DSM-IV eating disorders as well as dietary restraint, eating concern, shape concern and weight concern over the last 28 days. In addition, all diagnostic questions addressed a 3-month time frame. Agreement between telephone and face-to-face diagnostic interviews has been found to be excellent and is likely to be highest for behaviourally anchored items [18]. To allow for the assessment of lifetime disorders using DSM-IV diagnostic criteria, the EDE was also revised with insertion of lifetime questions, including the age range during which the behaviour occurred in order to assess the co-occurrence of features.
All interviewers were postgraduate Clinical Psychology trainees who had been trained in use of the EDE by the first or second author. Each of the interviews was taped. Each new interviewer submitted these tapes as they were completed to the second author (JB) who listened to them and provided any required corrective feedback until it was felt that the interviewer had fully grasped the skills required to complete the interview independently. When interviewers were unsure of coding they requested a second opinion. The first two authors made the final coding decisions.
Several measures were taken to ensure interview fidelity, including monthly group meetings with TW and JB to discuss the interview process and independent ratings by the first author (TW) of a subsample of taped interviews (n = 36) of women who had lifetime AN. The inter-rater reliability (Pearson's correlation) of the four subscales of the EDE (last 4 weeks) was high: 0.96 (weight concern), 0.98 (shape concern), 0.93 (eating concern) and 0.93 (dietary restraint). Another rater assessed the presence of lifetime objective binge episodes, using a random selection of 22 taped interviews (nine featuring lifetime BN, five with BED and eight where purging had occurred in the absence of objective binge episodes). There was agreement about the absence or presence of objective binge episodes on all occasions except one (a woman with BN), due to some ambiguity about the exact amount of food consumed when the person was feeling out of control with their eating.
Assessment of long-term course
The long-term coursewas assessed in threeways. First, the number of women currently meeting criteria for an eating disorder was examined. Second, the current weight, shape and eating concern, dietary restraint and body mass index (BMI) for each of the eating disorder groups was compared to women who had no lifetime eating disorder. Third, Cogley and Keel [19] have suggested that weight and shape concern as assessed by the EDE provides a good indicator of general outcome such that clinical levels of these cognitive substrates (≥4) indicate poor outcome, and lower levels indicate better outcome with respect to depression, anxiety, body dissatisfaction and social adjustment. We therefore constructed six levels of outcome for the purpose of this study, each using bothweight and shape concern and presence of any threshold eating behaviours from the last 28 days. Each level is described in Table 3.
Statistical analyses
To examine any significant differences across diagnostic groups, general linear modelling was used for continuous data, and chi-squared statistics were used with dichotomous data. When comparing the current eating and weight of the diagnostic groups to women without a history of an eating disorder, independent variables were entered simultaneously into a multivariate logistic regression to produce odds ratios (ORs) with 95% confidence intervals (CIs). An alpha level of 0.05 was used for all statistical tests.
Results
Women with lifetime anorexia nervosa
A total of 19 women (1.9%, 95% CI = 1.1–2.7) met full criteria for lifetime AN. Sixteen additional women (1.6%, 95% CI = 0.8–2.4) met the criteria for AN with the exception of amenorrhea (‘partial AN’). A further eight women also met AN criteria but their amenorrhea status was less clear, as five were using oral contraceptives at the time of their low weight, two women recalled missing fewer than three consecutive menstrual cycles, and one woman could not remember the number of cycles missed. Therefore, a total of 43 women (4.3%, 95% CI = 3.0–5.6) met the criteria for lifetime AN (either full or partial).
Table 1 provides a breakdown of the type of AN experienced. As well as having had lifetime AN, 10 women met criteria for another eating disorder at a separate time over their lifetime, eitherBN(n = 5) or eating disorder not otherwise specified purging type (EDNOS-p). This latter category refers to a state characterized by purging behaviour at threshold levels in the absence of objective bulimic episodes. Of the five women who fulfilled these criteria, all had engaged in self-induced vomiting and two had also misused laxatives. The majority of the women had restricting type AN (n = 18), followed by 15 women with purging type AN, where AN had concurred with purging behaviour occurring at threshold levels: self-induced vomiting (n = 11), laxative abuse (n = 7) and diuretic use (n = 4). Only onewoman in this group also experienced concurrent objective binge eating episodes. Of the restricting type AN, six women (35%) had experienced binge or purge behaviours (selfinduced vomiting or laxatives) at an experimental level (for fewer than 2months or on only a couple of occasions). There were no significant differences among the AN groups with respect to lowest BMI (F[3, 39] = 0.60, p = 0.62), age of onset (F[3, 39] = 1.06, p = 0.38), months at low weight (F[3, 39] = 0.65, p = 0.59), or frequency of amenorrhea (χ2[3] = 0.65, p = 0.89).
Description of women with lifetime anorexia nervosa (AN), lifetime bulimia nervosa (BN), and lifetimebinge eating disorder and eating disorder not otherwise specified purging type (EDNOS-p)
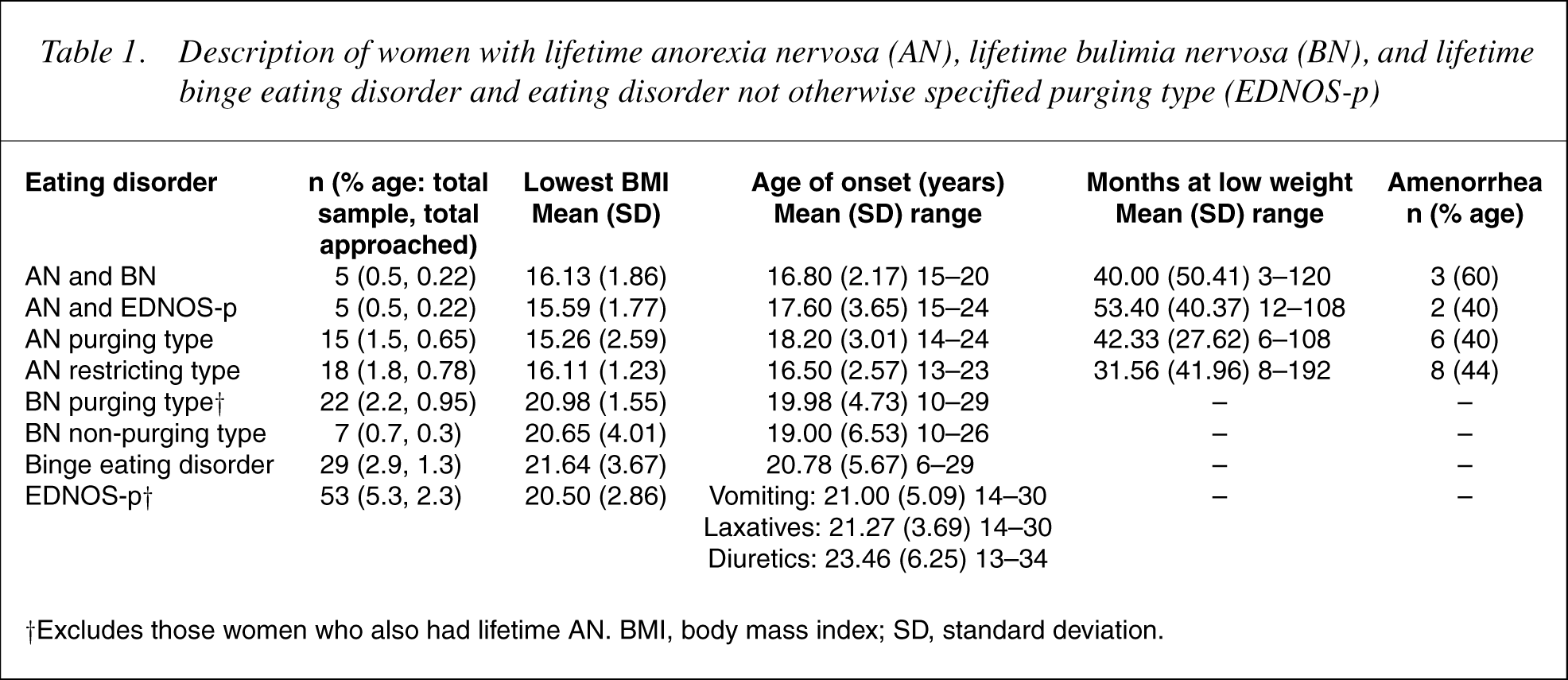
† Excludes those women who also had lifetime AN. BMI, body mass index; SD, standard deviation.
Women with threshold binge eating or purging eating disorders
A total of 35 women met full criteria for BN. Six of these women had also had AN, as described above, leaving 29 women (2.9%, 95% CI = 1.9–3.9) with lifetime BN only. Of all the women with lifetime BN, seven had a non-purging type while the majority had purging type. All of the non-purging type had used driven exercise and one of these had also used fasting concurrently with the objective binge episodes. Of the 22 women with purging type BN, 19 had used vomiting, six had used laxatives and two had used diuretics concurrently with the objective binge eating.
Binge eating disorder was diagnosed if the women reported experiencing objective binge episodes at least twice a week for a 3-month period without a break of more than 2weeks that was not concurrent with any threshold compensatory behaviours. Of the 29 women (2.9%, 95% CI = 1.9–3.9) who met these criteria, 18 reported no threshold weight control behaviour. A further six women had used threshold levels of weight control behaviour at a separate time from the binge eating (two fasting, one laxatives, two driven exercise and one vomiting). A further five women reported experimental and short-term use of fasting (n = 2), diuretics and vomiting (n = 1), vomiting and laxatives (n = 1), diuretics, fasting, driven exercise and laxatives (n = 1). These 11women with subthreshold compensatory behaviours could arguably be classified as some sort of partial BN, but we chose to retain them as BED given the unambiguous reporting of threshold objective binge eating in the absence of threshold weight loss behaviour.
Of those women who did not have a history of AN, BN or BED, there were 53 women (5.3%, 95% CI = 3.9–6.7) in the EDNOS-p category. Of these women, 20 (37.7%) had used vomiting, 33 (62.3%) had used laxatives and 11 (20.8%) had used diuretics. Four (7.5%) of these women had experienced subthreshold objective binge episodes. The women who used objective binge eating or purging to threshold levels are further described in Table 1. There were no significant differences among the four groups with respect to lowest BMI (F[3, 113] = 1.43, p = 0.24) or age of onset of binge eating (F[3, 113] = 0.59, p = 0.56); however, post-hoc testing revealed that the BN purging type group had attained a significantly lower BMI than the BED group (p = 0.046).
A further 43 women (4.3%, 95% CI = 3.0–5.6) reported lifetime use of threshold driven exercise or fasting in the absence of objective binge episodes or purging. A further 78 (7.8%, 95% CI = 6.1–9.5) women who did not have a lifetime eating disorder had used one of the three purging behaviours at subthreshold levels: 38 vomiting, 34 laxatives and 19 diuretics.
Long-term course
For women with a lifetime eating disorder, the EDE interview occurred a mean of 14.52 years (SD = 5.65) after initial onset: 17.26 (SD = 3.02) years since reaching a BMI < 17.5 for AN, 14.63 (SD = 5.38) years and 13.56 (SD = 6.30) years since experiencing objective binge eating for BN and BED respectively, and 11.44 (SD = 5.72) to 13.79 (SD = 5.41) years for EDNOS-p, depending on the specific purging behaviour onset. Three women (7%) with lifetime ANcontinued to have an eating disorder, one subthreshold AN, one BN, and one EDNOS-p. Two women with lifetime BN (7%) continued to meet criteria for BN. Three women (10%) with lifetime BED continued to meet criteria for BED, and three women (6%) of the EDNOS-p group continued to meet criteria for this disorder.
The long-term course of all thewomen with respect to current weight, shape and eating concern, dietary restraint and BMI is summarized in Table 2, with the groups being mutually exclusive. It can be seen that there is a slightly different profile for each group. The women with lifetime AN had significantly higher weight and shape concern but a lower level of dietary restraint and BMI than women who had never had a lifetime eating disorder. Examination of the lifetime AN subgroups showed that the purging and restricting types of AN had significantly lower current BMI than the comparison group, and that the AN purging type had significantly higher shape concern (OR = 2.28, 95% CI = 1.15–4.49) whereas the AN restricting type had significantly higher weight concern (OR = 2.91, 95% CI = 1.32–6.41). The women with lifetime BN had significantly higher levels of eating concern and dietary restraint than women with no lifetime eating disorder. There were no differences in this pattern between the non-purging and purging types of BN. The women with lifetime BED also had significantly higher levels of dietary restraint than the women with no eating disorder history, whereas the women with lifetime EDNOS-p had significantly higher levels of shape concern. When women with current eating disorders were removed from the respective eating disorder groups, there was little change to this pattern, except that shape concern was no longer significantly higher for the women with lifetime AN, and the women with lifetime BED had a significantly higher BMI (OR = 1.07, 95% CI = 1.01–1.15, p = 0.03).
Relationships between lifetime eating disorder (ED) status and current eating and weight using logistic regression to compare women with no lifetime ED to each ED group
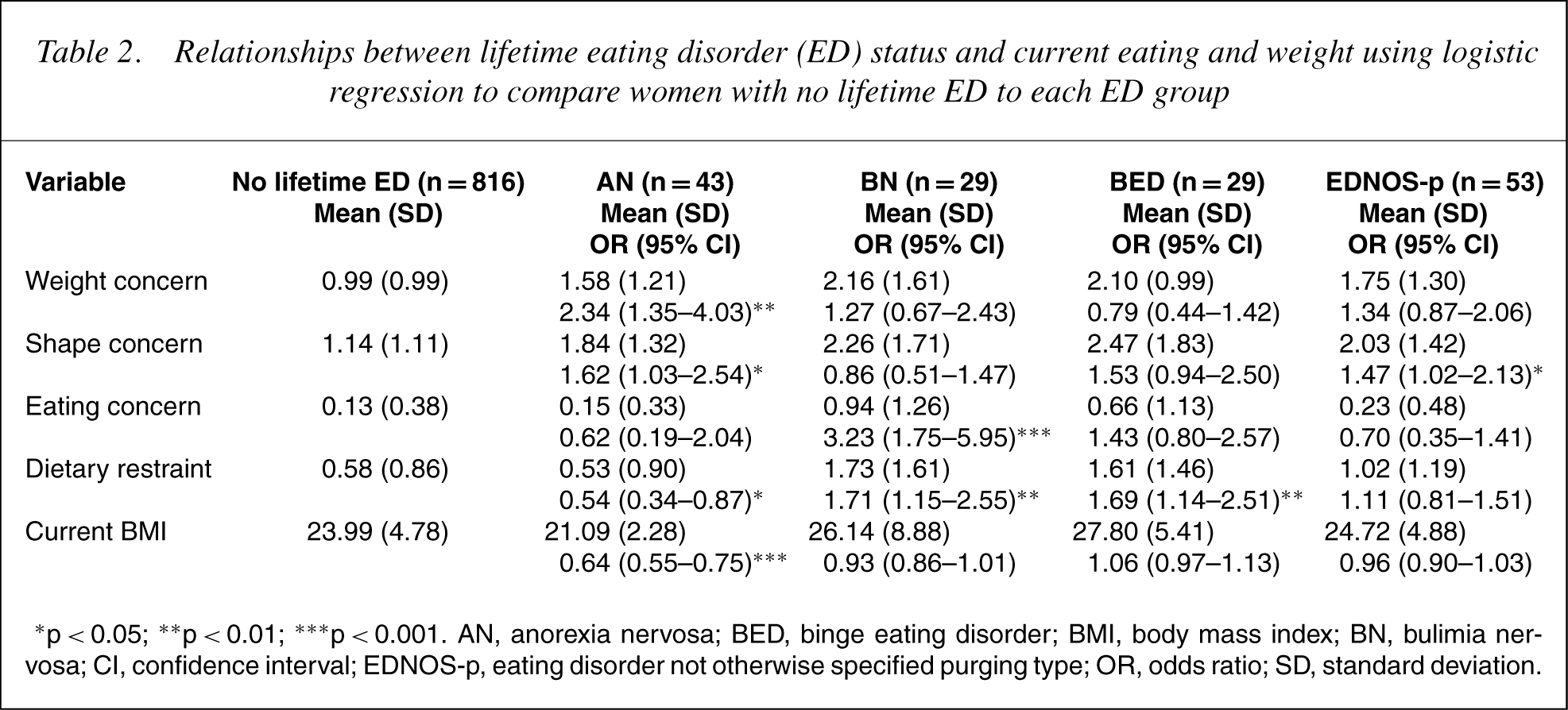
∗ p < 0.05; ∗∗ p < 0.01; ∗∗∗ p < 0.001. AN, anorexia nervosa; BED, binge eating disorder; BMI, body mass index; BN, bulimia ner-vosa; CI, confidence interval; EDNOS-p, eating disorder not otherwise specified purging type; OR, odds ratio; SD, standard deviation.
Long-term course in terms of our six-level outcome measure is described in Table 3. Not surprisingly (except for the women who had both AN and BN), the women with no history of an eating disorder had the highest proportion of women who were asymptomatic (74%). Among the eating disorder groups, 21 women with AN (49%) and 14 (48%) women with BN were asymptomatic. Achieving good outcome or above were 84% of women with AN, 76% of women with BN, 69% of women with BED, and 89% of women with EDNOS-p, compared to 96% of the women without an eating disorder history.
Outcome associated with each lifetime eating disorder, based on weight concern (WC), shape concern (SC) and threshold behaviours† over the last 28 days
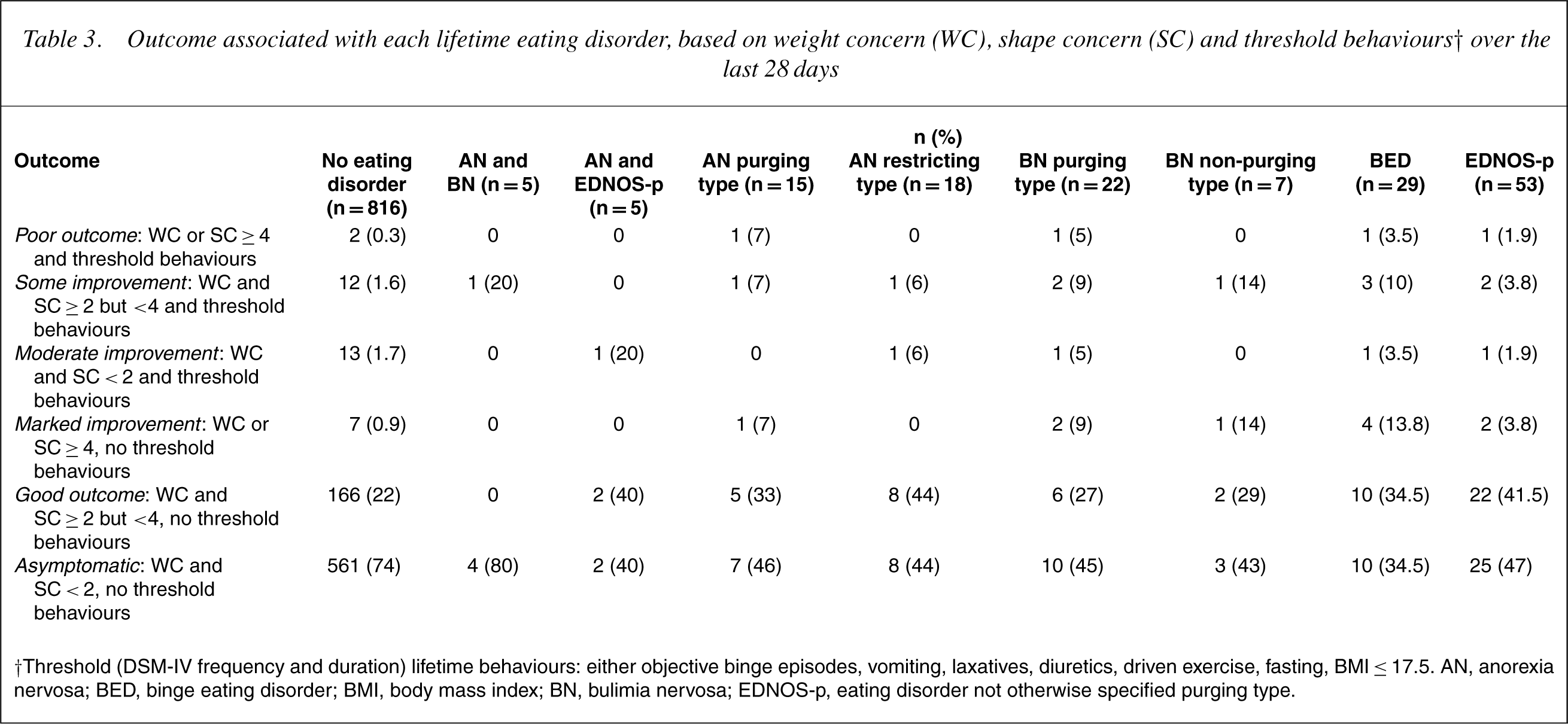
† Threshold (DSM-IV frequency and duration) lifetime behaviours: either objective binge episodes, vomiting, laxatives, diuretics, driven exercise, fasting, BMI ≤ 17.5. AN, anorex nervosa; BED, binge eating disorder; BMI, body mass index; BN, bulimia nervosa; EDNOS-p, eating disorder not otherwise specified purging type.
In addition, we examined the proportion of each group that met BMI criteria for obesity (BMI < 30). Approximately 7% of the women with no eating disorder history met these criteria whereas this was true of none of the women with lifetime AN or lifetime non-purging BN. Of the remainder, 22% of the women with lifetime purging BN met the criteria, as did 28% of the women with lifetime BED, and 15% of the women with lifetime EDNOS-p.
Discussion
Recall of lifetime psychiatric symptoms has been shown to be poor over a 6-year period using brief interview tools [20, 21] so care needs to be taken with assessing any lifetime psychiatric disorder. Psychiatric symptoms are more memorable if the disorder is severe [20], so briefer assessments of eating disorders are likely to only identify the more severe cases. The version of the EDE used in this study aimed to enhance recall of less severe states by linking current functioning to lifetime functioning using extensive content probes about eating symptoms, providing clear explanations of the concepts assessed, and conducting several checks for cooccurrence of symptoms.
The prevalence of AN and BN in this sample was very similar to comparable community studies. Lifetime threshold AN was diagnosed in 1.9% of our total sample compared to 1.5% [2] and 2% [3] in other community samples where comprehensive eating disorder assessments were completed. The prevalence of ‘partial’ AN (amenorrhea not required) was 1.6% compared to 1.3% in the Italian study [3]. Afurther 0.8% ofwomenwithAN had an amenorrhea status that could not be ascertained. Given that previous research indicates that amenorrhea does not meaningfully distinguish between AN cases [4], 4.3% of the sample could be said to meet substantive criteria for AN. This level is commensurate with the partial AN prevalence of 3.3% found in an Italian community sample [3] and 3.8% in young American adults [1]. The level of BN in our sample was estimated at 2.9% (omitting those women who also had AN), in the same range as found previously in other community samples: 2.3% [2] and 4.6% [3]. Consistent with some previous studies [22, 23] we found no robust differences between the subgroups of women with purging or non-purging AN or with BN.
The existing data on the prevalence of EDNOS are less consistent. This is likely to be due in part to problems of definition discussed earlier. The prevalence of BED in our sample (2.9%) was similar to that of the American sample [2] at 2.7% but was somewhat higher than the Italian sample at 0.6% [3]. It is arguable that some of our BED cases could be defined as partial BN cases, which perhaps speaks to the difficulty of distinguishing these states [24]. The prevalence of lifetime EDNOS-p (5.3%) in our sample was higher than that previously estimated in a community sample at 1.1% [3]. Given that previous investigations were of youngerwomen, and that the age of onset of EDNOS-p was albeit non-significantly older in our sample, itmay be that both studies underestimated the lifetime levels of this state. In addition, 4.3% of women had lifetime threshold levels of either driven exercise or fasting in the absence of binge eating –both this form of disturbed eating and EDNOS-p require further research.
We found that approximately 6–10% of the women with lifetime eating disorders had a current eating disorder. In terms of status at long-term follow-up, each of the four main eating disorder groupings had a unique outcome profile relative to the non-eating disordered controls, where the ongoing disturbances were different across the disorders. These differences were consistent with the character of the original eating disorder. It was interesting to note that, in terms of current functioning, it is the two binge eating disorders (BN and BED) where dietary restraint continues to be significantly higher than that of women with no eating disorder history and than women with lifetime AN. However, some caution regarding the reports of the AN women must be used, as the condition is highly ego-syntonic and items for current function on the EDE subscales may be under-reported. Given previous research showing women with lifetime BN are significantly more likely to have obese parents than women with a history of AN [25], our data are consistent with the idea that women with AN may have a naturally lower BMI than women with binge eating histories, thus influencing dietary restraint in an ongoing fashion.
Our examination of this community sample, where there is likely to be a mixture of community and clinic cases, suggests that 49% of the AN group were asymptomatic, similar to the 50% recovery estimated in a Swedish community sample [14]. In addition, 84% of our cases were much improved over the mean follow-up of 14 years comparable to clinic cases where 76% were assessed as being fully recovered, a process that had taken an average of 6.5 years [26]. Approximately 50% of the BN group was also asymptomatic, and 76% were much improved. This contrasts with the results of another community study which showed approximately half to twothirds of women with BN continued to have a clinically significant eating disorder at 5-year follow-up [13]. It is likely our longer follow-up period was associated with higher rates of improvement. Our data suggested that the poorest outcome was seen in those women with lifetime objective binge eating, while the lowest proportion of women with good outcome resided in the BN or BED groups, in contrast to a previous study that found good outcome for BED [13]. Although we did not ask women about their treatment history, it may be that women in the AN group were more likely to seek or be offered treatment, given the public nature of their disorder, while women with a more secretive disorder were less likely to receive treatment. Although obesity was not part of our criteria for six-category outcome measure, we found that obesity was present for 15–28% of the women with non-AN disorders. We recommend that future outcome studies attend to the development or continuation of obesity throughout the long-term course of eating disorders that involve binge eating or purging in particular.
The results need to be interpreted in the context of four limitations. First, while we have a large sample, we have a moderate response rate (47%). This rate is commensurate with other large populations studies in Australia [27] but lower than others [28]. There was no indication that a past history of disordered eating influenced response and neither did a previous study of twins using interviews focused only on eating indicate that response was biased by previous eating problems [29]. However, those with poor outcome with respect to the eating disorder may have been under-represented in the current study. Second, as in all previous studies of the prevalence of eating disorders [9], we did not include impairment secondary to the eating disorder features. Therefore, the true clinical significance of these states is uncertain. Third, our community sample was drawn from a twin population, but to date no studies indicate any differences in rates of psychopathology compared to the general population [30]. Finally, while we used a highly reliable and valid eating disorder instrument, the accuracy of this tool for reporting retrospective eating disorder symptoms is unknown. Reliability over 10 years when using brief selfreport measures of disordered eating show a kappa of approximately 0.45–0.50 [31], compared to a kappa of 0.61 for major depression over a 6-year period using a structured psychiatric assessment [20].
In summary, we found that the prevalence of AN and BN in the community was commensurate with other community studies. It is ironic that the state with the highest apparent prevalence, EDNOS-p, is the one least researched. Provision of suggested research criteria by DSM would be one way of promoting further research of this disorder, similar to the escalation of research seen when suggested research criteria were provided for BED. In addition, while outcome was relatively good, less than 50% of any eating disorder group was asymptomatic, and thus particular ways of offering more assertive treatment and intervention that may be able to lead to a better outcome are required.
Footnotes
Acknowledgements
Grant 160009 from the National Health and Medical Research Council to TDW supported this work. CGF is supported by aWellcome Principal Fellowship (046386). The authors thank the twins for their participation in this research. Administrative support for data collection was received from the Australian Twin Registry.