
Abstract
Introduction
Adolescent major depression disorder (MDD) runs a relapsing, remitting course. In the community, the course of adolescent MDD was found to have a mean duration of 26.4 weeks (Lewinsohn et al., 1994). In clinical samples MDD persists in adolescents for a mean duration of between 27.8 weeks (Rao et al., 1995) and 34.6 weeks (Strober et al., 1993) to 35.6 weeks (McCauley et al., 1993). Adolescent MDD runs a chronic course in up to 10% of cases (Strober et al., 1993). Any measure to assist the clinician in determining the course of MDD at baseline or following treatment could be used to determine who would benefit from more intensive treatment.
This paper builds on the work previously published on the psychometric properties of the Self-Efficacy Questionnaire for Depressed Adolescents (SEQ-DA), a self-report questionnaire for use in depressed adolescents (Gordon et al., 2011; Tonge et al., 2005). The purpose of this paper is to further assess the SEQ-DA’s capacity to quickly screen for MDD and assist in predicting the course of the condition in clinical subjects.
Self-efficacy is defined as an individual’s “perceived ability to produce a desired action” (Muris, 2002: 337). The person’s perception of self-efficacy will “affect how much effort people will expend and how long they will persist in the face of obstacles or aversive experiences” (Cutrona and Troutman, 1986: 1508). Self-efficacy is derived from cognitive processes, where through self-reflective observational learning, the individual forms a view of their own ability to achieve tasks to a required standard (Bandura, 1977). Self-efficacy is regarded as important in emotional regulation and self-motivation (Bandura, 1989). It has been “assigned a central role, for analysing changes achieved in fearful and avoidant behaviour” (Bandura, 1977: 193). Self-esteem is a related but broad concept, whereas self-efficacy is a more discrete concept, easier to measure and more predictive of future functioning (Connolly, 1989).
A lack of self-efficacy has been hypothesised to be a pathway into adolescent depression through a number of mechanisms including inability to meet the expected standards of others, limited control over negative thoughts, hindered development of supportive social networks, and through anticipatory apprehension when faced with challenging situations (Muris, 2002). When faced with a stressor, individuals with low self-efficacy tend to give in easily, attribute failure to internal qualities, and experience elevated anxious and depressive symptoms (Cutrona and Troutman, 1986). Low self-efficacy is a psychological concept related to Seligman’s theory of learned helplessness (Seligman, 1974) and Beck’s cognitive theory of depression (Beck, 1976). Self-efficacy has also been linked to Lewinsohn’s model where self-perception and self-evaluation are mediators of adolescent depression (Kanfer and Zeiss, 1983).
Low self-efficacy in adults has been shown to be inversely correlated with depressive symptoms (Gondoli and Silverberg, 1997; Gross et al., 1994; Howell et al., 2006; Jones and Prinz, 2005; Pakenham et al., 2007). Two self-efficacy scales for coping with and managing depressive symptoms have been developed for use in clinically depressed adults (Gopinath et al., 2007; Perraud, 2000). Self-efficacy beliefs in the person’s own ability to cope with their depressive symptoms and manage their depression have been shown to predict of the course of a depressive disorder in adults (Gopinath et al., 2007; Perraud et al., 2006). In a longitudinal, prospective study, adult patients with lower depression coping self-efficacy at discharge from a psychiatric hospital were more likely to be rehospitalised by 6–8 weeks (Perraud et al., 2006). In a 1-year observational study of 386 adult primary care patients at high risk of relapse, lower self-efficacy to manage their depression was found to be one of the major factors implicated in depressive disorder relapse (Gopinath et al., 2007).
Self-efficacy has been shown to be consistently and inversely related to depression scores in non-clinical samples of adolescents (Bandura et al., 1999; Ehrenberg et al., 1991; Muris, 2001). Low baseline self-efficacy is reported to predict depression in community adolescents at 6-month follow-up (McFarlane et al., 1995) and is correlated with depression in community populations of children and adolescents at 12-month and 24-month follow-up (Bandura et al., 1999).
However, very little research has been done on self-efficacy in treated clinical populations of depressed youth. Hyun et al. (2005) reported on a cohort of South Korean adolescents living in a homeless shelter who were treated with cognitive behavioural therapy (CBT) over 8 weeks. Those randomly allocated to CBT showed improvement on the Beck Depression Inventory (BDI) and the Self-Efficacy Scale (Hyun et al., 2005). Pössel et al. (2005) conducted a 10-week CBT school-based depression prevention program, finding that those students with low self-efficacy on the General Self-Efficacy Scale had greater improvement on the Center for Epidemiological Studies Depression Scale scores following CBT than those with initially higher self-efficacy scores.
Of the existing self-efficacy measures only the SEQ-DA has been developed for clinical use in depressed adolescent subjects. The SEQ-DA was designed to measure self-efficacy in adolescents with depressive symptoms and trialled in a clinical sample (Tonge et al., 2005). It was modelled on the Self-Efficacy Questionnaire for School Situations (SEQ-SS) (Heyne et al., 1998), a similar measure of capacity to cope with anxiety and school attendance.
In a previously published study in a cohort of 130 depressed adolescents, the SEQ-DA scores at baseline and following 3 months of treatment separately predicted those youth who would be depressed at 6-month follow-up (Gordon et al., 2011). This current study aims to gather further data on the use of the SEQ-DA in this cohort of depressed adolescents, extending the work to now include MDD and depressive disorders at time points not described in the previous study. A preliminary analysis will be undertaken to assess the correlation between SEQ-DA and self-reported depression scores on the Reynolds Adolescent Depression Scale (RADS) and possible sex differences between the SEQ-DA and self-reported depression scores.
Self-report measures that are easily completed and scored can be used as an aid to assist the clinician in decision making. A diagnostic test in primary care that discriminates between youth with a major and minor depression and those depressed youth who are likely to be depressed following treatment and separately at 6-month follow-up may guide the primary care clinician as to who should be referred for more intensive treatment. A diagnostic test result may be positive or negative, and this result can be correct or incorrect as judged by a gold standard. The sensitivity is “the test’s ability to identify true cases” (i.e. a positive result when this is true by the gold standard) and the specificity is “the test’s accuracy in identifying non-cases” (i.e. a correct negative result when this is true by the gold standard) (Blacker and Endicott, 2008: 11). Given that the SEQ-DA has been shown to predict depression at long-term follow-up (Gordon et al., 2011), specific cut-off scores can now be determined by use of a receiver operating characteristic (ROC) analysis. The gold standard used in this study is the presence of a MDD or a depressive disorder as judged by the Schedule for Affective Disorders and Schizophrenia for School Aged Children (K-SAD).
Likelihood ratios are a clinically relevant statistic that provides a ratio of probabilities for a test with only two possibilities (e.g. depressive disorder versus not depressed) (Deeks and Altman, 2004). The likelihood ratio of a positive test result (LR+) is calculated from the formula LR+ = sensitivity/(1 − specificity). Likelihood ratios allow the results of a study to be translated into the clinician’s office for use with a given patient. The knowledge of pre-test probability (of depression) together with a likelihood ratio allows for the calculation of a post-test probability of having a disease (e.g. a depressive disorder).
Materials and methods
Subjects
One hundred and thirty adolescents (65.4% female) aged 12 to 18 years (15.1 years) with a depressive disorder were recruited within two community-based randomised clinical trials (Berriga House [BH] and Time for a Future [TFF]) for the treatment of an adolescent DSM-IV depressive disorder (MDD, Dysthymic Disorder or Depression Not Otherwise Specified). One hundred and nineteen (92%) of the adolescents were born in Australia, three were born in England, two in New Zealand, and one each in Iran, China, Japan, Lebanon, Serbia and the Netherlands.
Design
The study design has been previously described (Gordon et al., 2011). In brief, depressed adolescents were assessed at baseline (T1) and then randomised and treated for 3 months for their depression with one of CBT, supportive counselling, sertraline pharmacotherapy, or a combination of CBT and pharmacotherapy. Assessments of the adolescents were made at baseline (T1), following 3 months of treatment (T2), and at 6-month follow-up (T3) involving clinician assessment and a number of adolescent and parent report measures. One hundred and eleven adolescents were assessed following treatment at T2 and 96 were assessed at T3.
Independent measure
SEQ-DA comprises 12 questions about how the adolescent thinks that they could cope with depressive behaviours and feelings. Responses are recorded on a five-point Likert-type scale of ability to cope with depressive symptoms ranging from really sure I couldn’t; probably couldn’t; maybe; probably could; and really sure I could cope. The SEQ-DA inquires about the adolescent’s ability to cope with managing activities, sadness, poor appetite, poor sleep, tiredness, concentration problems, irritability, dealing with negative thoughts, everyday hassles, social anxiety, thoughts of self-harm, and changing life events. The SEQ-DA scores range from 12 (low self-efficacy) to 60 (high self-efficacy). The SEQ-DA was reported to have good internal consistency (Cronbach’s α = 0.73), and test–retest reliability (Pearson’s r = 0.85) (Tonge et al., 2005). The SEQ-DA construct validity of the SEQ-DA has been reported, with the SEQ-DA negatively correlated with the RADS, a self-report measure of adolescent depression (Pearson’s r = – 0.67) (Tonge et al., 2005). A copy of the SEQ-DA is found in the appendix of Tonge et al. (2005).
Outcome measures
The measures utilised in this study were drawn from a larger battery of assessments (Gordon et al., 2011). The clinician assessed the young person with the Schedule for Affective Disorders and Schizophrenia for School Aged Children Lifetime (K-SADS-L) in order to determine depressive diagnosis according to DSM-IV criteria (Ambrosini, 2000) at T1, T2 and T3. The young person also completed SEQ-DA and the RADS. The RADS is a reliable and valid adolescent self-report questionnaire used to gauge depressive symptoms along a dimensional scale with higher scores indicating a higher level of depression (Reynolds, 1987).
Analyses
Regression and logistic regression analyses have been previously reported with the finding that the SEQ-DA scores at T1 in the single model and SEQ-DA scores at T2 in single and multivariate models predicted any depression at T3 (Gordon et al., 2011). Correlations between the RADS scores and SEQ-DA were undertaken in this current study. Separate correlation and predictor analyses for males and females were undertaken to explore whether there was a gender difference in predicting depression in this clinical cohort. Analyses were then conducted to establish appropriate clinical cut-off scores for the SEQ-DA. ROC analyses have been employed to locate the optimal cut-off score that provides the best combination of sensitivity and specificity in rating scales used for depressed adolescents (Clarke et al., 1992; Rey and Morris-Yates, 1992). As the SEQ-DA scores are inversely correlated with depression, in order to predict depression for the ROC analysis the SEQ-DA scores were transformed. The SEQ-DA scores were transformed by subtracting the SEQ-DA scores from 60 (the maximum SEQ-DA score possible) and then re-interpreted back for reporting.
Data was analysed using the Statistical Package for the Social Sciences Version 11 (SPSS Inc., Chicago). The BH and TFF projects had received ethical approval from the Southern Health Human Research Ethics Committee.
Results
Of the 130 depressed adolescents assessed at T1, 72 adolescents suffered with MDD, 30 had a dysthymic disorder and 28 suffered with depressive disorder NOS. Of the 111 adolescents assessed at T2, 57 were not depressed, 7 suffered with MDD, 18 suffered with MDD in partial remission, 25 had dysthymic disorder and 4 suffered with depressive disorder NOS. At T3, 96 adolescents were followed up with 70 not being depressed, 5 still suffering with MDD, 14 with MDD in partial remission, 2 with dysthymic disorders, and 4 with depressive disorder NOS.
The SEQ-DA scores at T1 (n = 129) ranged from 14 to 49 (mean 34.40, SD 6.68), the SEQ-DA scores at T2 (n = 106) ranged from 18 to 57 (mean 41.70, SD 7.54) and the SEQ-DA score at T3 (n = 89) ranged from 21 to 59 (mean 44.22, SD 8.06). At each of the three assessment points (T1, T2 and T3), 95% of the SEQ-DA scores fell within two SDs of their respective means. The SEQ-DA 5% trimmed mean at T1 was 34.57, at T2 was 42.01, and at T3 was 44.62, suggesting little effect of outliers at any of the three assessment points. There was no difference in mean SEQ-DA or RADS scores at T1 on independent t-tests between those who stayed and those who later dropped out at T2 or T3. Equally, there was no difference in mean SEQ-DA or RADS scores at T2 on independent t-tests between those who stayed and those who dropped out at T3.
An independent t-test showed that the SEQ-DA scores were significantly higher in boys than girls (t = 2.297, df = 127, p = 0.023, two-tailed) at T1, however there was no significant gender difference on SEQ-DA at T2. The RADS at T1 were significantly higher in girls on independent t-test (t = −4.689, df = 118, p < 0.001, two-tailed), however there was no significant gender difference on RADS score at T2.
It was previously reported that over the course of the study, the RADS depression score decreased (T1 = 82.18, T2 = 66.33 and T3 = 59.44) (Gordon et al., 2011).
A preliminary assessment was undertaken to assess the degree of correlation between the SEQ-DA scores at T1 and T2 and the level of depression at T3 as measured by the RADS score. The RADS and SEQ-DA scores at the three time points are all significantly and negatively correlated; the findings are summarised in Table 1.
Correlation matrix of RADS and SEQ-DA
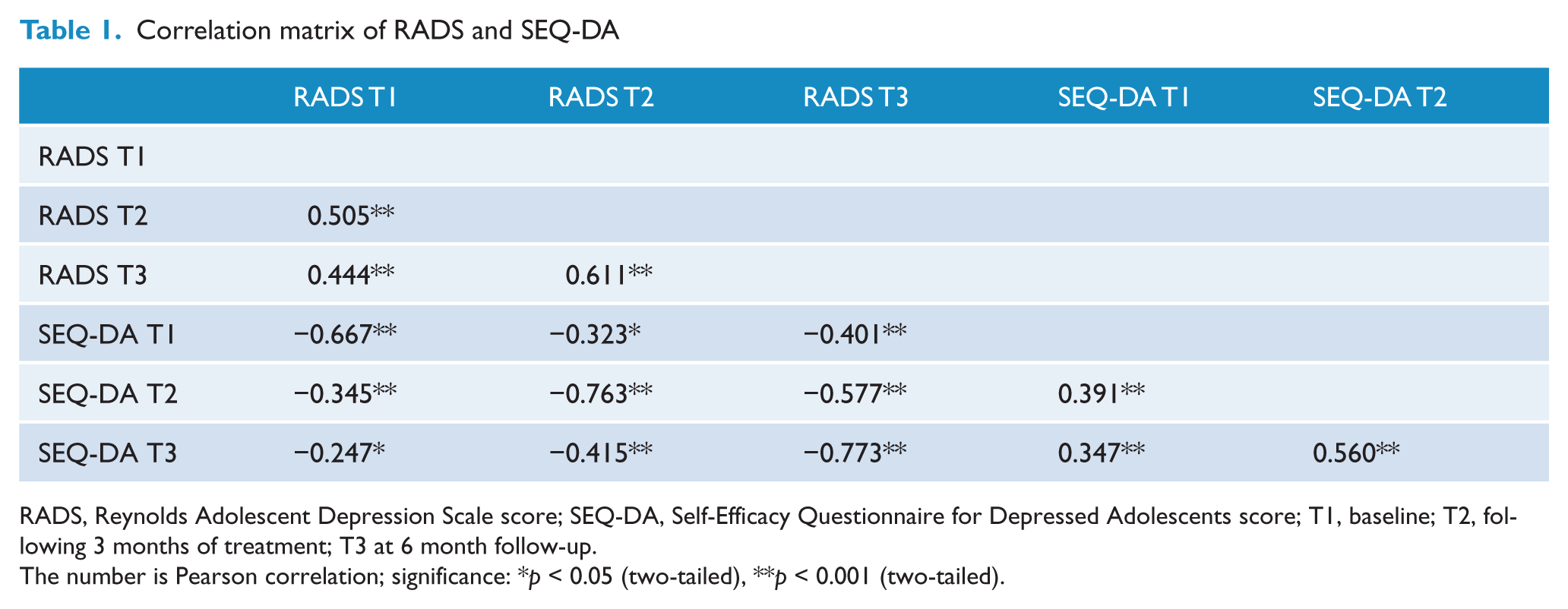
RADS, Reynolds Adolescent Depression Scale score; SEQ-DA, Self-Efficacy Questionnaire for Depressed Adolescents score; T1, baseline; T2, following 3 months of treatment; T3 at 6 month follow-up.
The number is Pearson correlation; significance: *p < 0.05 (two-tailed), **p < 0.001 (two-tailed).
In view of the gender difference on the SEQ-DA and RADS scores identified at T1, a secondary analysis was undertaken to explore the gender differences on the degree of correlation between the SEQ-DA scores and the RADS scores at T3. The male SEQ-DA scores at T1 and T2 were correlated with the RADS scores at T3 (r = −0.603, p < 0.001, two-tailed and r = −0.598, p = 0.001, both two-tailed, respectively). The female SEQ-DA scores at T1 and T2 were also correlated with the RADS scores at T3 (r = −0.256, p = 0.045, and r = −0.571, p < 0.001, both two-tailed). It is clear that the SEQ-DA score at T1 and T2 remained significantly and inversely correlated with RADS score at T3 for both males and females.
Binary regression analyses
Univariate binary regression analyses were undertaken to explore the relationship between the SEQ-DA scores, and a current or future DSM-IV MDD or any DSM-IV depressive disorder diagnoses are described in Table 2. There was a consistent predictor effect of the SEQ-DA in discriminating those adolescents with MDD as well as predicting future depressive disorders.
Binary regression analysis of the Self-Efficacy Questionnaire for Depressed Adolescents (SEQ-DA) in predicting major depressive disorder (MDD) and any depressive disorder diagnosis at various time points
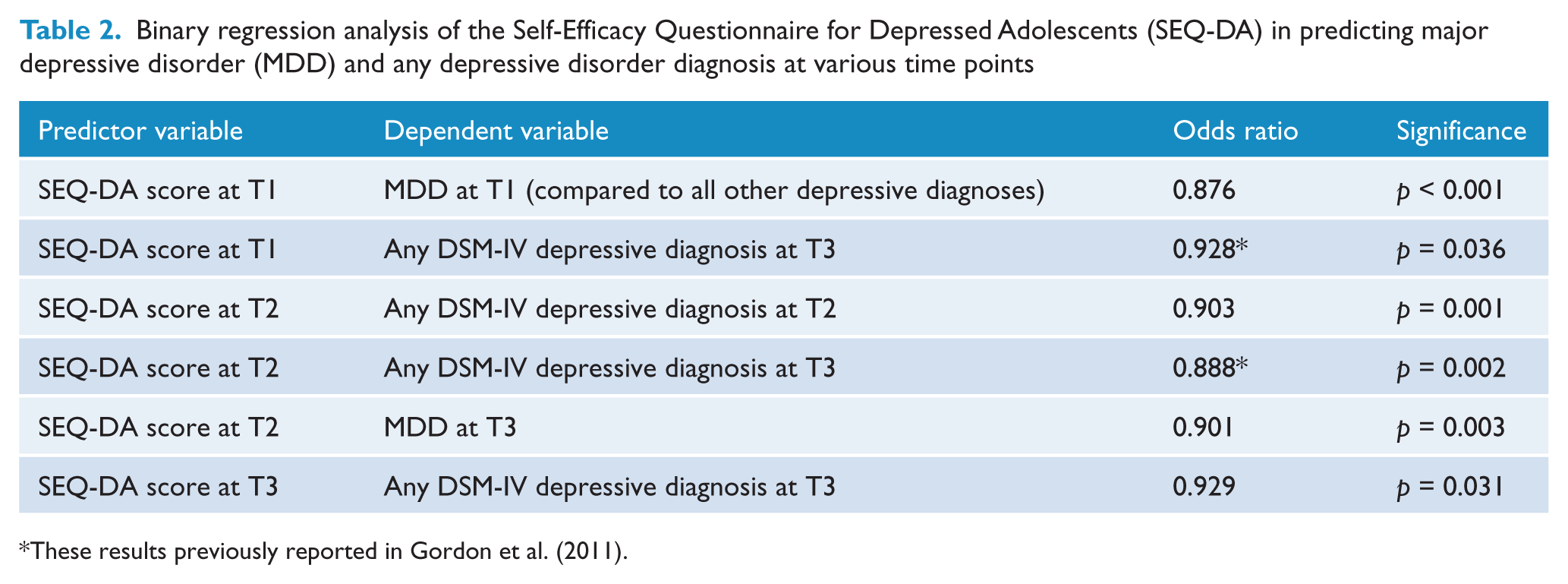
These results previously reported in Gordon et al. (2011).
ROC analyses
The cut-off scores were calculated for the SEQ-DA scores at the three time points in predicting both a depressive disorder and MDD, with sensitivity and specificity given (Table 3). SEQ-DA scores at T1 that are under 36 were predictive of MDD at T1 and predictive of any depressive disorder at T3; SEQ-DA scores at T2 that are under 43 were predictive of depressive disorders at T2 and T3.
Receiver operating characteristic (ROC) analysis of the Self-Efficacy Questionnaire for Depressed Adolescents (SEQ-DA) in predicting major depressive disorder (MDD) and any depressive disorder diagnosis at T1 and T2
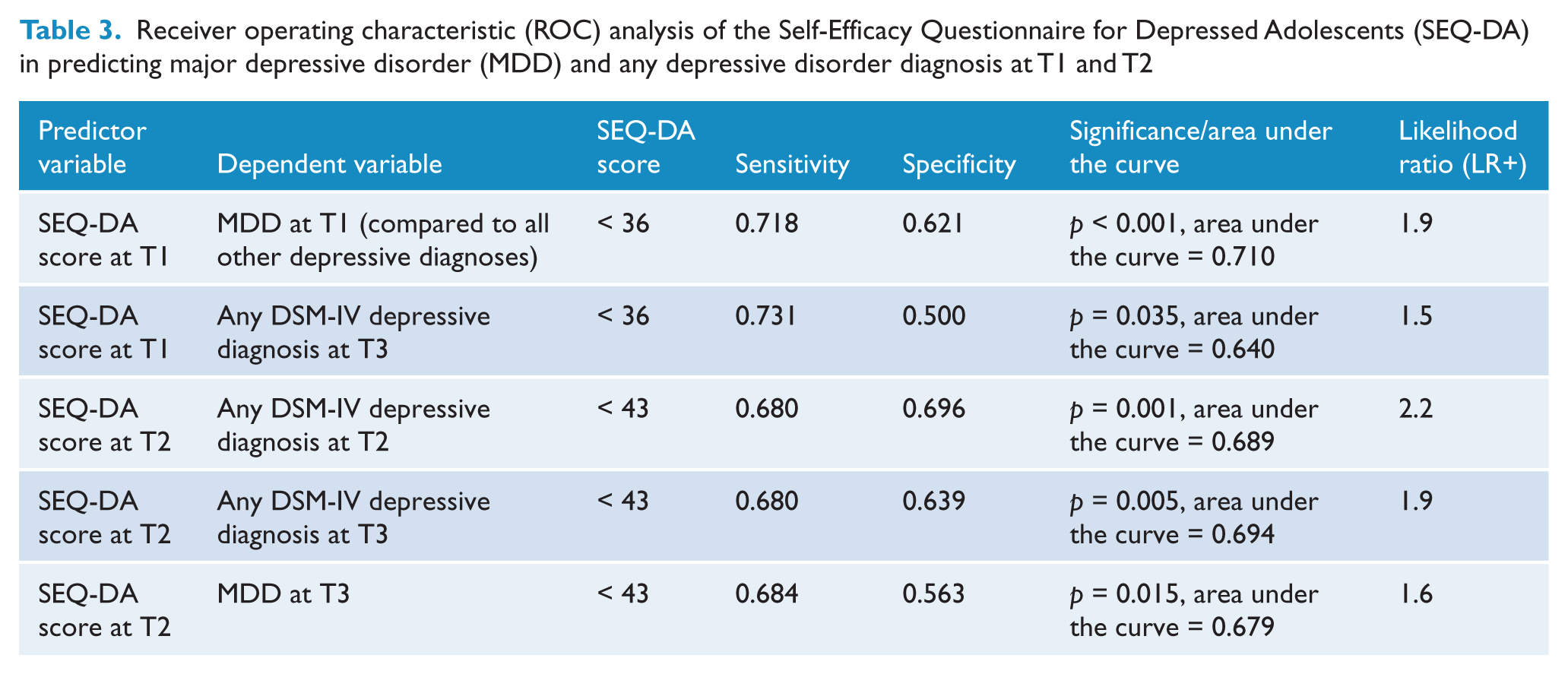
Likelihood ratios
The likelihood ratios of depression (LR+) are also given in Table 3. The post-test probability is a function of the prevalence of the condition and the LR+ and can be calculated by means of a nomogram (Deeks and Altman, 2004; Lawrie et al., 2000). For instance, if the given base rate of MDD for any referral into a child psychiatry clinic is 40% (Biederman et al., 1995) then for any patient presenting at this service who scored less than 36 on their screening SEQ-DA prior to being seen, their chances of having a MDD (i.e. the post test probability) is 56%. Alternatively if the base rate of MDD for any referral into a child psychiatric clinic is 25% (Kolvin et al., 1991) then for any patient presenting at this service who scored less than 36 on their screening SEQ-DA prior to being seen, their chances of having a MDD is 39%.
Discussion
This is the first paper to use an adolescent self-efficacy questionnaire to measure the capacity to cope with depressive symptoms in a clinical population, providing meaningful cut-off scores for the prediction of future depressive disorders. This paper extends the previous findings where the SEQ-DA was found to be a robust predictor of adolescent depression at T1 and T2, in both the binary and linear regression analyses (Gordon et al., 2011). Together these findings provide clinicians working with depressed young people with a brief measure that may help detect those who may experience further difficulties with depression following acute treatment. The findings also strongly suggest that the adolescent’s self-assessed self-efficacy makes a meaningful contribution to the development of their depressive symptoms.
A measure to track the course of depression is important as relapse and recurrence following empirically supported treatments such as CBT (Birmaher et al., 2000; Vostanis et al., 1998) and antidepressant medication (Emslie et al., 1998) is common. The finding of the SEQ-DA being a measure to predict the course of adolescent depression is consistent with research from adult studies where the self-efficacy scale for managing depression (Gopinath et al., 2007) and the Depression Coping Self-Efficacy Scale (Perraud et al., 2006) were found to predict relapse and rehospitalisation, respectively.
The SEQ-DA is also inversely related to continuous variables which describe depression. There is a significant negative correlation between the RADS score and the SEQ-DA score, which is consistent with an inverse relationship between self-efficacy and depression. This is in keeping with findings from community samples on self-efficacy in adults inversely correlating depression with self-efficacy (Gondoli and Silverberg, 1997; Gross et al., 1994; Howell et al., 2006; Jones and Prinz, 2005; Pakenham et al., 2007). The SEQ-DA independently identified both male and female adolescents at T1 who were at high risk of persistent depression at T3. However, the finding of the SEQ-DA as a predictor is perhaps not a surprise; Bandura has suggested that enhanced self-efficacy is related to the capacity to think clearly about future ability to cope (Bandura, 1989). The SEQ-DA in essence asks the adolescent to think about whether they could manage various potential symptoms of depression now and into the future.
The SEQ-DA has a sensitivity of 72% and specificity of 62% of predicting MDD at T1. By comparison, the BDI has a comparable sensitivity of 76.9% and a specificity of 64.8% of screening for MDD (Whitaker et al., 1990), however this finding was in a non-referred group of adolescents. Further, the BDI is a direct measure of depressive symptoms, not an indirect measure of depression through the adolescent’s self-assessed coping. By comparison with a non-inventory measure of depression, the Dexamethasone Suppression Test (DST) was found to have a sensitivity of 87% and a specificity of 53% in diagnosing MDD in a small cohort of inpatient children (Petty et al., 1985). The calculated likelihood ratio of the DST (LR+ = 1.85) is comparable to the SEQ-DA.
The preliminary findings of this study suggested that there may be a gender bias inherent in the SEQ-DA with higher scores (increased self-efficacy) reported in males at initial assessment. This discrepancy appears to disappear following 3 months of treatment. It is unclear whether this is a property of the scale or if adolescent girls appear to mark themselves down more than boys.
Limitations
This study has several limitations and assumptions that require consideration when interpreting the findings. This paper has pooled the results of two studies but both studies had comparable design and identical outcome measures. It was assumed that the treatments given between T1 and T2 of CBT and/or sertraline and supportive counselling were equivalent. Selection bias, the length of depression prior to entry into the study and non-depressive comorbidity were not controlled for.
It is assumed that the SEQ-DA does not have any ceiling or floor effects. However as the adolescent patients improved over time the extreme scores moved towards the highest possible score (i.e. 60) on the SEQ-DA. It was reasoned for this clinical sample that given that the SEQ-DA scores at all three data points fell within two SDs of their respective means and that there was little difference between the 5% trimmed mean and the actual means that this was not significant. It may be that in a community sample a ceiling effect may be evident.
Current research is under way to characterise the predictive qualities of the SEQ-DA with this same cohort of depressed adolescents over a longer follow-up period of 3 to 9 years. Further research is also under way to assess the SEQ-DA in a non-clinical school-based cohort.
Conclusion
The findings support the use of the SEQ-DA as a simple screening device for clinicians working with depressed young people, to stratify adolescents into those at greater risk of future depression and to modify their treatment and follow-up accordingly. Further investigation of normative scores for adolescents in the community, both with and without depression, are needed to characterise the SEQ-DA cut-off scores in a non-clinical group.
Footnotes
Acknowledgements
Dr John Taffe provided invaluable statistical advice. The sertraline used in Time for a Future was provided by Pfizer Pharmaceuticals.
Funding
Funding for Time for a Future was through the Department of Human Services Victoria Mental Health Branch, Australian Rotary Health Research Fund, Department of Human Services Barwon Region Innovative Practice Grant, and the Commonwealth Department of Health and Aged Care. Berriga House was funded through an NHMRC project grant (grant 990154).
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.