
Abstract
Objective:
Clinicians are tasked with assessing the relationship between violence and mental illness. Yet, there is now a legal expectation in some countries that public services, including health professionals, assess risk of violent extremism – with few available measures. We previously developed a new measure of Sympathies for Radicalisation, using items that measure Sympathies for Violent Protest and Terrorism. In this paper, we present the detailed psychometric properties of a reduced item measure of Sympathies for Violent Protest and Terrorism. We use data from two studies to test replication and then validity against outcomes of self-reported violence and convictions in the entire sample and in those with depressive symptoms.
Methods:
Data from two cross-sectional neighbourhood surveys, consisting of Pakistani and Bangladeshi adults (survey 1, n = 608) and White British and Pakistani adults (survey 2, n = 618), were used to undertake confirmatory factor analysis of Sympathies for Radicalisation and produce a short measure of Sympathies for Violent Protest and Terrorism. Survey 2 data were used to test the Sympathies for Violent Protest and Terrorism’s convergent validity to classify presence/absence of violence and convictions in the whole sample and for subgroups by depressive disorder.
Results:
The seven-item measure’s structure was a consistent measure of extremist attitudes across the two surveys. A threshold score of zero to classify violence was optimal (specificity = 89.7%; area under the curve = 0.75), but sensitivity to a risk of violence was poor (34.5%). The short version Sympathies for Radicalisation was a better classifier of violence in respondents with depression, dysthymia or both (area under the curve = 0.78) than respondents with neither (area under the curve = 0.69; β = 0.62, 95% confidence interval = [−0.67, 1.92]; standard error = 0.66).
Conclusion:
The seven-item measure of Sympathies for Violent Protest and Terrorism is an accessible and valid measure for clinical assessments and helpfully identifies low risk of violence. It enables clinicians to conduct detailed assessments of people endorsing one or more of the items, although further research is needed.
Introduction
In many countries, health professionals and public sector workers are required to report people who express violent extremist attitudes on the grounds that they may be connected with terrorist networks or plotting terrorist acts. However, the evidence to support this interventionist approach is lacking as there are few evidence-based tools to assess risk (Hurlow et al., 2016). Underlying this expectation is a proposed process of ‘radicalisation’ by which an individual becomes increasingly sympathetic towards extremist beliefs and then persuaded to engage in violence. In this model – and consistent with definitions of extremist radicalisation in the United States, Canada and Europe – extremist attitudes count as proxies for radicalisation. Yet, the notion of radicalisation and its assessment in clinical settings is contested given the limited empirical evidence of causal links between extremist beliefs and violence (Knudsen, 2020). Thus, there is a risk of criminalising marginalised people. The challenge of validating measures of violent extremism is a lack of longitudinal data. Such research is ethically difficult as observations might lead to breaches in confidentiality and incrimination. Furthermore, if people involved in radicalised networks participate in research, they are unlikely to reveal their radical beliefs and intentions. Alternatively, covert methods of gathering data are ethically questionable (Younis and Jadhav, 2019).
A preventive approach to extremism and terrorism is consistent with public health interventions to reduce violent crime, suicide, smoking and a range of other medical conditions (Bhui et al., 2012; National Academies of Sciences, Engineering and Medicine, 2017). Existing assessment tools include the Vulnerability Assessment Framework (VAF) and the Identifying Vulnerable People Guidance (IVPG) (Egan et al., 2016; HM Government, 2012). Both tools were validated in known terrorist offenders; hence, their validity in non-offenders is unknown (Scarcella et al., 2016). Furthermore, using the VAF or IVPG requires clinical expertise and judgement and may not be appropriate for use by a broader range of non-specialists, including public and civil servants. Nor can they be self-completed as within a survey or screening questionnaire. These tools do not capture a broad typology of terrorist offences (Lloyd and Dean, 2015), nor are they designed to measure multiple situations and various points in the process between adopting extreme beliefs and acting upon them. The stages that offer preventive opportunities are (1) holding extreme beliefs that sympathise or support violent extremism and (2) a propensity for violence.
In our previous published research, we developed a measure of extremist beliefs called Sympathies for Radicalisation (SyfoR) (Bhui et al., 2014). This was undertaken through stakeholder engagement with community, faith, academic and charity groups, to identify risky behaviours related to violent extremism (Bhui et al., 2014). The SyfoR has high face and content validity (Scarcella et al., 2016). This paper addresses three gaps in the literature: (1) testing independent samples to verify the factor structure of the SyfoR, which measures Sympathies for Violent Protest and Terrorism (SVPT; that is, construct validity), and (2) testing whether SVPT are associated with violence in a general population more generally, that is violence unrelated to extremism and terrorism (i.e. convergent validity). We asked about violence in general rather than terrorism-related violence, as respondents are unlikely to incriminate themselves by reporting participation in terrorism and even if they had committed such acts, it is highly unlikely they would answer affirmatively. Furthermore, terrorism-related violence is extremely rare in the general population, so asking such questions in a general population survey would deter participation or raise concerns about the intentions of the survey. The ethics committee and our early focus group work in the development of the SyfoR also concluded such questions should not be asked. Finally, (3) given our previous analyses, suggested depressive symptoms were associated with SVPT, and the mandate in government policy that health professional show due regard to assessing extremism, we tested properties of the SyfoR for assessing violence in general in the whole sample and in a subset of people with depressive symptoms.
Method
Design
Data were collected in two surveys in 2011 and 2016 (Bhui et al., 2014, 2019). Both surveys comprised attitudinal and lifestyle questions, along with questions to measure SVPT. First, we used confirmatory factor analysis (CFA) to test the fit of the latent structure of SyfoR to produce a short validated measure. CFA was used to produce adjusted and weighted scores showing the contribution of items to an overall score, standardised to the sample population.
Second, we tested the convergent validity of short item measure of SVPT to calculate sensitivity, specificity and predictive values, using receiver operating characteristics (ROC) with an outcome of self-reported violence or convictions. Finally, given the interest in prevention in patients presenting with mood disorders, and findings that depressive disorders are associated with SVPT (Bhui et al., 2019), we tested the convergent validity of our SVPT measure to classify those reporting violence, among those with and without depressive disorders.
Participants and sampling
Data collected in 2011 (survey 1) included responses from 608 individuals across two localities in England: East London and Bradford. Sampling points were selected from Census data for their high Muslim population density to generate a diverse sample. Participant inclusion criteria were of Pakistani and Bangladeshi heritage and aged 18–45 years.
Data collected in 2016 (survey 2) included responses from 618 individuals, across three localities in England: Blackburn (with Darwen), Bradford and Luton. Sampling points were those identified as high population density of Pakistani inhabitants. Again, inclusion criteria were those aged 18–45 years, but of Pakistani or White British ethnicity.
In both surveys, respondents were approached via door-knocking in selected communities. Responses were collected using hand-held computers in the presence of a researcher that enabled participants to give confidential responses. Respondents gave informed consent after receiving a complete description of the study, which was recorded electronically. Equal sampling quotas were set for age groups 18–30 years and 31–45 years, gender, ethnicity and full-time workers versus other employment status. The recruitment and surveys were conducted by Ipsos MORI, a social survey company, and anonymous data with pre-calculated sample weights were provided in the data files. The weight provided by Ipsos MORI was applied in analyses as a population weight to adjust for quota sampling and non-response.
Variables and measurement
Both surveys contained sociodemographic variables, as well as lifestyle and attitudinal items comprising religious attendance, social contact, social capital, political engagement, stressful life experiences and questions about depression and generalised anxiety (Kroenke et al., 2001; Spitzer et al., 2006).
Attitudes towards extremist behaviours were measured using the SyfoR questionnaire of 16 (survey 1) or 17 items (survey 2) designed using stakeholder engagement with community organisations, and academic and charitable institutions (Bhui et al., 2014). Attitudes towards these behaviours were measured on a 7-point Likert-type scale ranging from −3 = ‘completely condemn’ to 3 = ‘completely sympathise’, and ‘neutral’ responses scored as zero. An expression of ‘sympathy’ was considered an attitudinal risk. Previous analyses of the survey 1 data found an association between higher SyfoR scores and common mental disorders, criminal history and trauma (Bhui et al., 2016, 2019). Similar associations were reported in a separate study of individuals with convictions for terror-related offences (Jensen, 2016), adding to the credibility of SyfoR in measuring a vulnerability to being radicalised (Bhui et al., 2019).
In previous research using data from survey 1, a principal component analysis using 16 SyfoR items identified four distinct factors (Bhui et al., 2014). The first component was a seven-item subset measuring SVPT; a second component – sympathies for defensive violence; the third – attitudes towards UK foreign policy; and the fourth component – sympathies for fighting against British troops. The four distinct components were replicated in the second survey (Bhui et al., 2019), which included an additional 17th item – the act of fighting against British troops in Syria – that loaded on component 4. The seven-item measure of SVPT consisted of the most extreme attitudes related to violence and terrorism and was found to be consistent between the surveys.
To measure violence propensity, we used the following items: (1) one or more convictions for violent offences with or without harm to life or health, or (2) occasional or more frequent fighting and/or property damage, measured on the Gunn Criminal Profile questionnaire (Gunn and Robertson, 1976). The comparison group reporting no violence included people with no convictions for violence and no history of fights or property damage.
We used International Classification of Diseases, 10th Revision (ICD-10) diagnoses of depression and dysthymia and tested whether the classification properties of our seven-item measure of SVPT in the entire sample also held for people with these depressive disorder diagnoses. Testing the role of depressive disorder on the classification of violence using our seven-item measure of SVPT was in accordance with the findings of a previous study showing associations of SVPT with ICD-10 diagnoses of dysthymia, and/or moderate to severe depression (binary measure vs those with neither).
Diagnostic criteria were generated using algorithms reported in analyses of survey 2, using the Clinical Interview Schedule–Revised (CIS-R, Das-Munshi et al., 2014) and additional items for dysthymia. An indication of depression required at least one symptom of persistent sadness/low mood, loss of interest/pleasure or fatigue/low energy, as well as problems with sleep, concentration, confidence, appetite, suicidality, agitation or guilt/self-blame. An indication of dysthymia required two or more depressive symptoms that occurred most of the day, most days, for 2 years or more (World Health Organization, 1992).
Statistical methods
Analysis proceeded in three stages: first, multiple imputation of missing values; second, CFA to test construct validity of the short item measure of SVPT; and third, a test of the convergent validity of the short item measure of SVPT in classifying violence propensity in the overall sample, with and without depressive disorder.
Imputation and missing data
We were able to score 122 of 137 respondents with missing data on depressive disorder using consensus ratings by two, and if necessary three, clinicians who had access to all the information collected. Using this procedure, 89% of the missing diagnostic data were scored. Multiple imputation of further missing data is outlined in the statistical annex.
CFA
CFA was undertaken using data from both surveys to derive a valid structure for a measure of SVPT. SVPT scores were calculated as the sum of weighted item scores. The item weights were calculated as the item’s contribution to the overall latent variable, measured as the proportion of each factor loading to the sum of all factor loadings in CFA. These standardised proportional weights are presented in Table 1. Sensitivity analyses were run using complete cases only and imputed data for each model. More detail on the methods used in multiple imputation and CFA is provided in the supplementary file.
Proportional weights for scoring the SVPT; derived from CFA in merged survey 1 and 2 data.
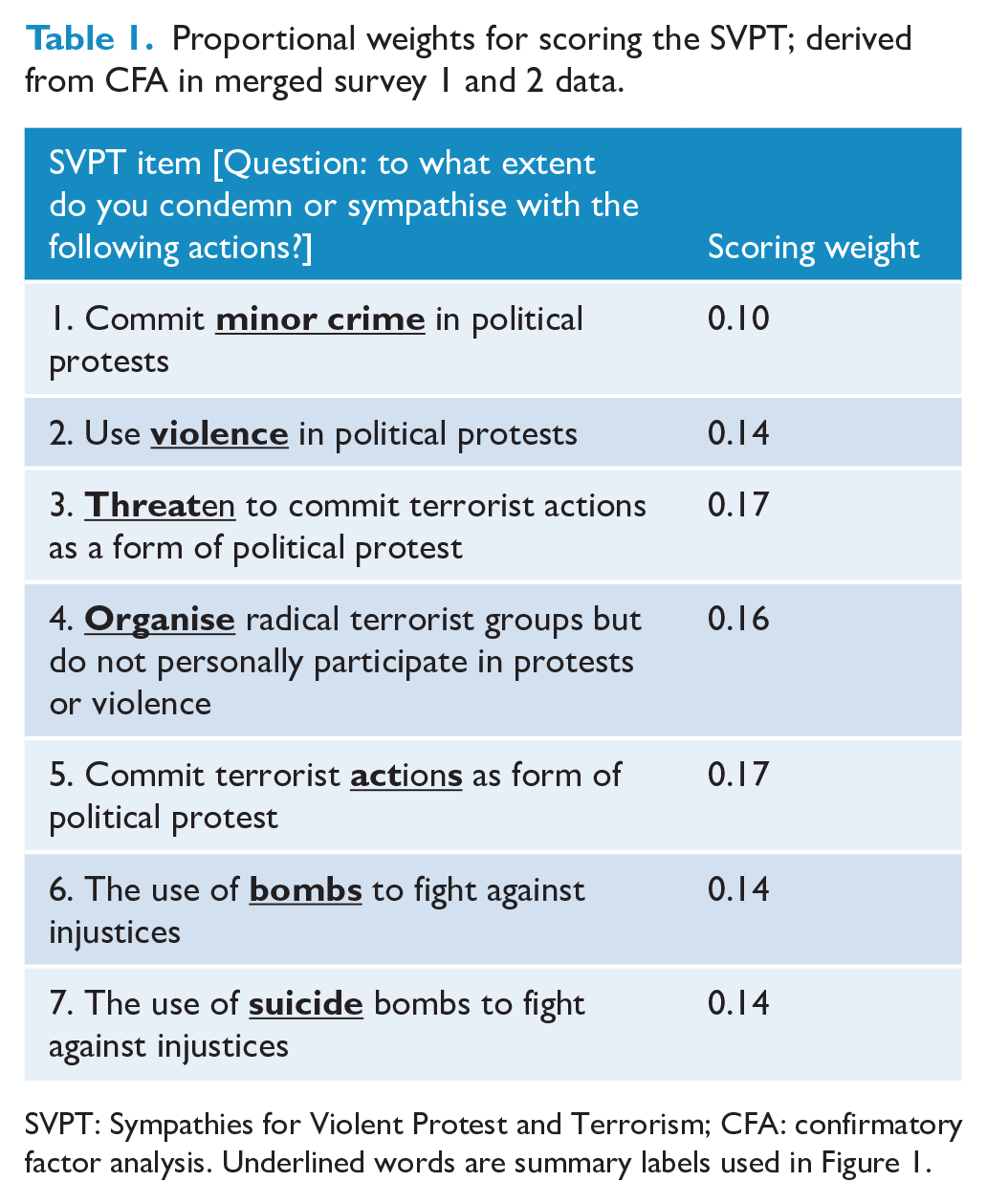
SVPT: Sympathies for Violent Protest and Terrorism; CFA: confirmatory factor analysis. Underlined words are summary labels used in Figure 1.
Testing classification against violence
The validated seven-item measure of SVPT and the new scoring method were used in subsequent analyses to classify violence propensity. Associations between SVPT and violence were tested using logistic regressions, both unadjusted and adjusted for ethnicity, gender, age and marital status. The classification of violence was then tested to produce sensitivity, specificity and prediction at thresholds in the SVPT scores. Likelihood ratios (LRs) are provided as the nonparametric alternative to predictive values, with a binary outcome. ROC regression analyses were used to test the covariate role of depressive disorders on the classification of violence propensity using an optimal threshold for SVPT, when adjusted for age, gender, ethnicity and marital status. All analyses were conducted in Stata version 13.1 for Windows and weighted using the population weight as provided by Ipsos MORI who conducted the surveys.
Results
Factor structure of the measure of SVPT
Using CFA, the seven-item measure of SVPT produced an acceptable model fit and high internal consistency. The structure of the short measure of SVPT is shown in Figure 1, and the proportional weights for scoring the final seven-item measure are presented in Table 1, with a scoring manual in the supplementary materials.
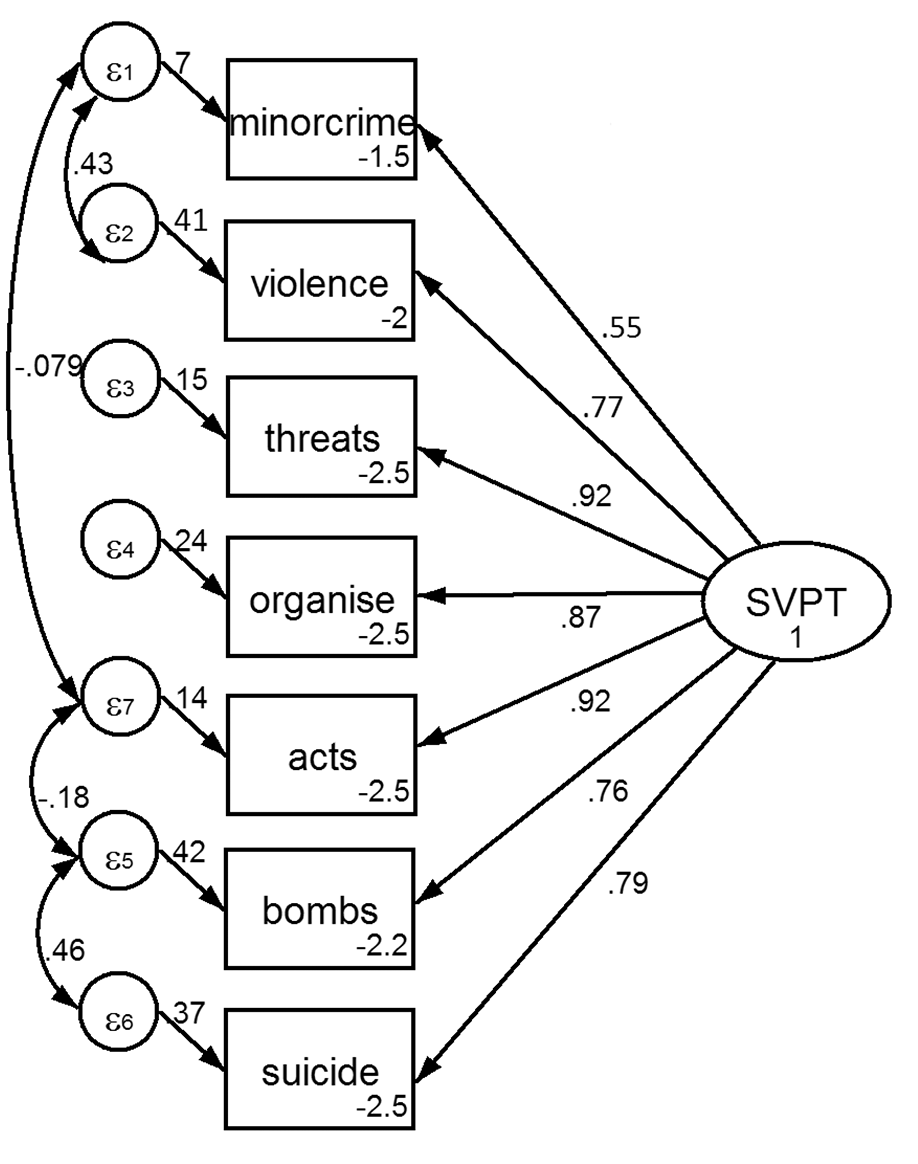
Validated seven-item SVPT structure from confirmatory factor analysis, using merged 2016 and 2011 imputed data.
Testing associations between SVPT and violence propensity
Significant univariate risk factors of violence propensity were a higher SVPT score (odds ratio [OR] = 1.44, 95% confidence interval [CI] = [1.1, 1.83]; p = 0.004), being male (OR = 2.65, 95% CI = [1.02, 6.89]; p = 0.045), being aged 18–30 years (compared to 31–45 years; OR = 4.25, 95% CI = [1.27, 16.09]; p = 0.02) and being single (OR = 3.1, 95% CI = [1.09, 8.89]; p = 0.03). In the multivariable model including sociodemographic variables, the weighted SVPT score was associated with higher risk of violence propensity, when adjusted for age, gender, ethnicity and marital status (OR = 1.33, 95% CI = [1.05, 1.68]; p = 0.02; n = 523). There were similar findings for complete cases in sensitivity analyses. Adjusted and unadjusted associations are shown in supplementary Table e2.
Classifying violence propensity using SVPT
The unadjusted sensitivity, specificity and predictive validities of the seven-item measure of SVPT in classifying people reporting and not reporting violence are presented in Table 2. The threshold SVPT score of more than or equal to −2.5 had the best trade-off in sensitivity and specificity and the maximum correctly classified people (specificity = 68.4%, sensitivity = 62.1%; correctly classifying 68%). However, a score of zero or more had a specificity of 89.7%, indicating a better classification of true negatives. Thus, zero is arguably a more valid and practical threshold score to improve the correct rejection of people unlikely to be at risk of violence.
Sensitivity, specificity and likelihood ratio (LR) of violence at SVPT thresholds, using unadjusted and survey 2 imputed data.
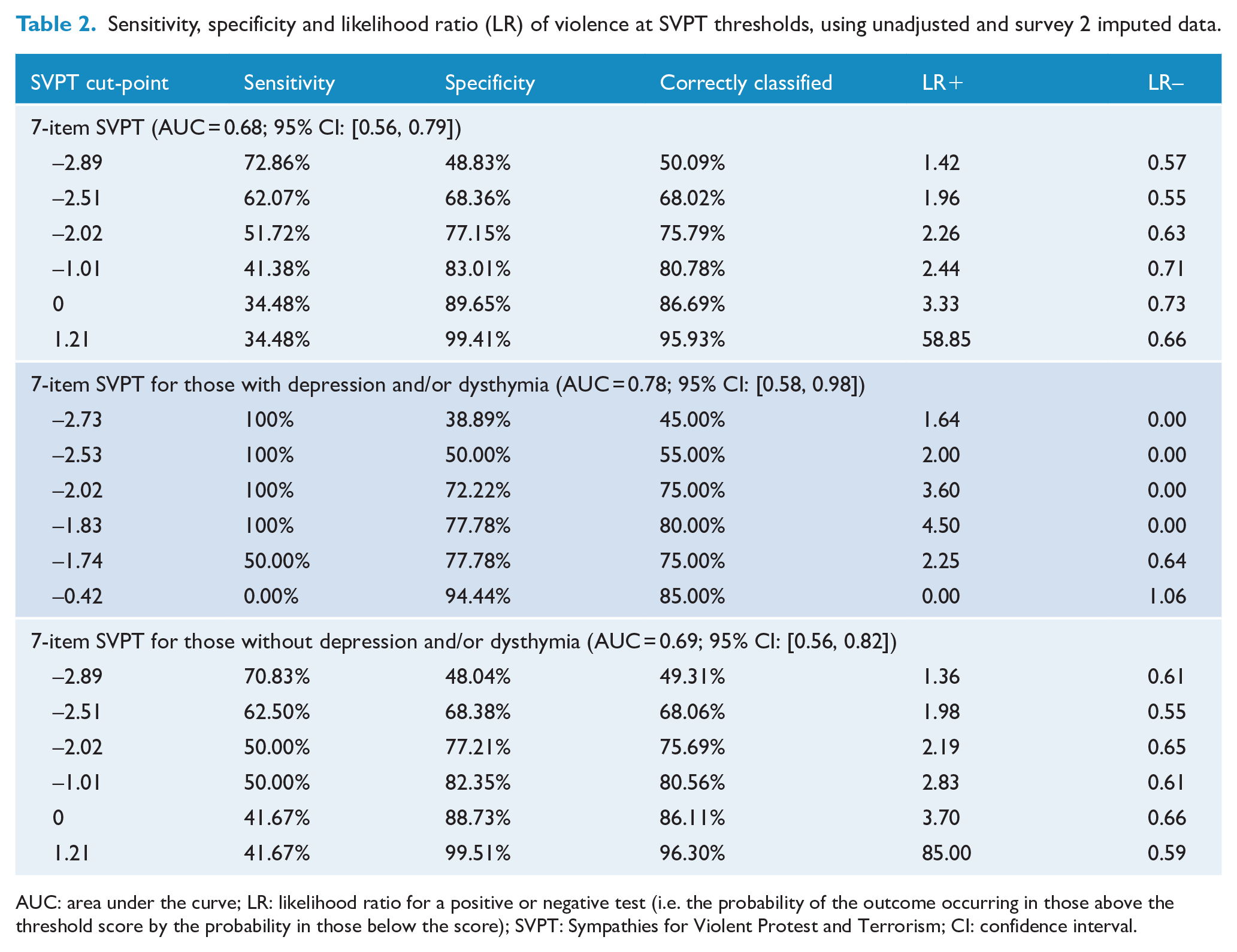
AUC: area under the curve; LR: likelihood ratio for a positive or negative test (i.e. the probability of the outcome occurring in those above the threshold score by the probability in those below the score); SVPT: Sympathies for Violent Protest and Terrorism; CI: confidence interval.
The overall convergent validity of the short measure of SVPT in classifying violence was fair (area under the curve (AUC) = 0.75, 95% CI = [0.56, 0.79]) when adjusted for age, gender, ethnicity and marital status. The short measure of SVPT was a better classifier of violence propensity in those with depression, dysthymia or both (AUC = 0.78, 95% CI = [0.58, 0.98]), compared to those without (AUC = 0.69, 95% CI = [0.56, 0.82]; β = 0.62, 95% CI = [−0.67, 1.92]; SE = 0.66). In the presence of dysthymia or depression, a high classification of true negatives of non-violence was achieved with a lower threshold score of −0.42 (specificity = 94.4%). A sensitivity–specificity plot classifying violence by presence of depression and dysthymia or their absence is displayed in Figure 2, adjusted for marital status, age, gender and ethnicity. Sensitivity analyses using complete cases only were consistent with results from imputed data.
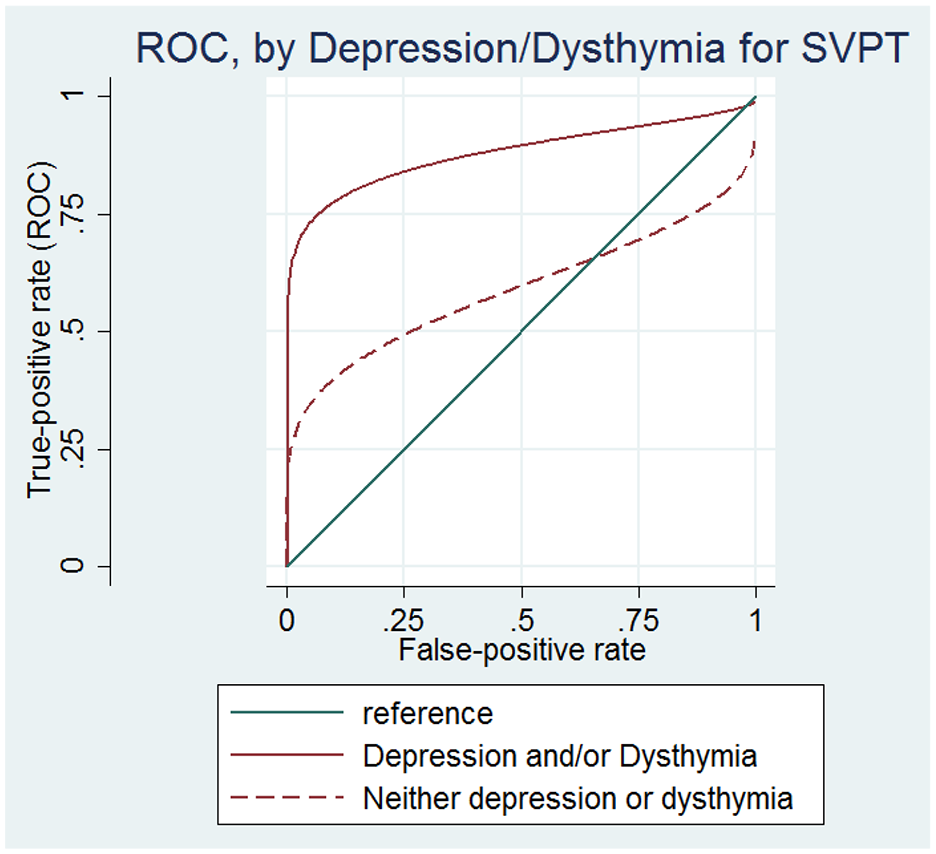
Classifying violence using SVPT by depressive disorder, adjusted by demographics on imputed 2016 data.
Discussion
Guidance for countering violent extremism often identifies risk as changes in appearance and behaviours, strongly expressed ideological opinion, or condoning harm, hate and violence towards others or groups (Home Office, 2015). However, these factors lack specificity, and attempts to translate these behavioural indicators into practice have received criticism for stereotyping and scapegoating marginalised individuals (Weine et al., 2017). Attempting to predict whether an individual who holds extreme attitudes will then perform criminal acts is challenging. Arguably, a more appropriate and evidence-based approach is required (Bhui et al., 2012). The short measure of SVPT provides a practical option as an early-stage assessment to screen out those with low risk and recommend more detailed judgements for those scoring high.
The seven-item measure of SVPT can support clinical assessment of individuals thought to be at risk of violent extremism, especially those presenting with depressive symptoms. This is an important finding as previous research shows relationships between violent offending and terrorism with depressive symptoms. A threshold score of zero had a specificity of 89%, that is, a low probability of false positives – being important for screening purposes for the rare phenomenon of violent extremism. A higher score is associated with a greater propensity to violence and can be used qualitatively to guide more detailed clinical assessment. Our measure of SVPT is a marginally better classifier of violence propensity in those with depression, dysthymia or both, compared to those with neither, suggesting a useful role in assessing people with mood disorders who hold extremist beliefs or have a history of violence. We are further testing the measure in forensic populations.
The findings support the more general body of research that risk prediction of violence using structured measures is poor (Coid et al., 2013). Individual assessments incorporating our measure of SVPT should use additional assessment tools. Additional evidence of cognitive and affective risk factors are important for assessment of vulnerability to engaging in violent extremism, including a heightened sense of injustice; intolerance of alternative beliefs; attempted abolition of perceived threats; paranoia, rage or suspiciousness; self-righteousness (Altemeyer and Altemeyer, 1996; Berlet, 2004; Boyd, 2010; De Regt et al., 2011; Hetherington and Suhay, 2011; Jost et al., 2003; Rogers et al., 2007; Rokeach, 1954; Seipel et al., 2012; Strozier and Boyd, 2010); distress, trauma and social disconnectedness (Bhui et al., 2014, 2016; Centre for the Prevention of Radicalization Leading to Violence (CPRLV), 2018); as well as mental disorders including depression, dysthymia, post-traumatic stress disorder (PTSD) and anxiety (Bhui et al., 2014, 2016, 2019; Borum, 2014; Corner and Gill, 2015; Jensen, 2016; Victoroff, 2005), and should also consider a person’s political and societal context (Knudsen, 2020).
The strengths of the SyfoR are that it was developed through community engagement, supported by cognitive debriefs in pilot studies before the surveys were undertaken, resulting in higher content validity and normative acceptability (Bhui et al., 2014; Scarcella et al., 2016). Psychometrically, the short version of the SyfoR holds a consistent factor structure across ethnically and geographically diverse populations, improving its potential generalisability. A systematic review of risk assessments of radicalisation reported that only the IVPG tool out of 30 assessed tools had published positive and negative predictive values in classifying terrorism offences, together with sensitivity and specificity to risk (Scarcella et al., 2016). The IVPG is a risk criterion used in professional settings and was validated using a sample of 157 offenders with terror-related convictions (Egan et al., 2016). Thus, its use is restricted to those with a history of convictions for violent extremism offending and deemed unsuitable in a community and non-criminal setting (Egan et al., 2016). Whereas the short measure of SVPT is suitable for community populations, it has similar predictive value to the IVPG. The short measure of SVPT had a ‘fair’ accuracy for classifying violence (AUC = 0.75), similar to fair accuracy of the IVPG in classifying violent outcomes in ‘Islamists, Irish Republicans, and right-wing extremists collectively’ (AUC = 0.73). The short measure of SVPT is the first risk measure of violent extremism for preventive use in non-offenders; however, we did not validate it against actual terrorist incident, given their rarity; rather we used self-reported violence to show that the attitudinal measure does associate with criminality and violent behaviours more generally.
More empirical work is needed to ensure policy and practice is evidence based. Measures of extremism risk should be applied with careful judgement around ethics, given the invariably poor psychometric properties of most available risk assessments of violence in the presence of mental disorder (Coid et al., 2013), and in predicting violence longer term (Ramesh et al., 2018).
Future research
Future work should seek to validate the SVPT’s sensitivity to changes in risk, test–retest consistency and prevalence of SVPT in specific populations with mental illness, criminality or both (Scarcella et al., 2016). For example, it is possible that those with historical violent offences are more likely to adopt extremism beliefs, and both lead to depressive symptoms; or that depressive symptoms make the adoption of violence and extremism more likely, although at face value many people with mental illnesses are not violent nor participating in terrorism; thus, the additional risk factors that make some people with depressive symptoms hold more SVPT need investigation. This might be done by research to establish the sequence of developing depressive symptoms, violent offending and SVPT. Further validation of the measure comparing terrorist and other violent offenders may also be useful, although challenging in terms of the sample sizes needed and the relatively few people convicted of terrorist violence. Assessing people showing violent behaviours or criminality for SVPT also has practical value for clinicians to be alert to susceptibility to radicalising influences. The short SyfoR is available for further empirical research and we offer a scoring mechanism, yet research needs careful balance of the ethical dilemmas we have discussed above. It is important not to add inadvertently to stigma and fears of people with depressive symptoms or mental illnesses.
Supplemental Material
Supplementary_file – Supplemental material for Assessing risks of violent extremism in depressive disorders: Developing and validating a new measure of Sympathies for Violent Protest and Terrorism
Supplemental material, Supplementary_file for Assessing risks of violent extremism in depressive disorders: Developing and validating a new measure of Sympathies for Violent Protest and Terrorism by Kamaldeep Bhui, Michaela Otis, Kristoffer Halvorsrud, Mark Freestone and Edgar Jones in Australian & New Zealand Journal of Psychiatry
Footnotes
Author contributions
K.B. made substantial contributions to the conception, design, acquisition, analysis, interpretation and drafting; M.O. made substantial contributions to the design, analysis, interpretation and drafting; K.H. contributed to the design, interpretation and revision; M.F. contributed to the design, analysis, interpretation and revision; E.J. made substantial contribution to the conception, interpretation and revision. All authors approved the final version and agree to be personally responsible for their contributions.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: All authors report no conflicts of interest or financial relationships with commercial interests, except K.B. who is undertaking a separate project for CPNI examining the role of culture in mental health assessments, as a general learning set for practitioners.
Ethical Approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human participants were approved by Queen Mary University of London Research Ethics Committee: QMERC2015/06.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of Data and Materials
The authors had full access to the anonymised dataset compiled by Ipsos MORI. The dataset generated and/or analysed during the current study are not publicly available as it contains ethically sensitive information, and we are developing further analytic methods, but we are happy to collaborate with groups on reasonable requests. Regrettably due to the sensitivity and care needed in managing and interpreting the analyses, we feel this is a responsible position and supported by our ethics review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.