
Abstract
Objective
The concept of duration of untreated psychosis or DUP has been a strong candidate for intervention as part of the early intervention paradigm. However, its importance has been questioned. This paper aims to present selected issues concerning attempts to reduce DUP and evaluate the impact of these attempts.
Method
Current research designs are critiqued and alternatives considered.
Results
Evidence suggests that it is difficult to design studies that are both ethical and potent enough to determine the contribution of treatment delay to outcome.
Conclusions
Further research is justified but this should not obstruct commonsense service reforms.
How important is the duration of untreated psychosis in influencing outcome? A young man of 19 years of age, let us call him Steve, is involuntarily hospitalised with the assistance of the police after an aggressive incident. It becomes clear that he has been frankly psychotic for more than a year and prior to that had become progressively more withdrawn and isolated over the previous 2 years. He had dropped out of school during this period, had lost contact with most of his friends and had increased his cannabis usage to 10–15 bongs per day. His family had made several efforts to get help for him but were confused about the nature of his problem and he was highly reluctant to go along with efforts to assist him. Eventually, an outburst, one of many in recent months, led to a physical altercation with his brother. This led to a traumatic process of admission to hospital.
This remains a not uncommon scenario in clinical settings where patients are first treated. Who could doubt that earlier recognition of the problem and rapid initiation of effective treatment would have prevented most of the negative sequelae, moved the young man back toward his developmental trajectory and have led to a better short-term outcome at least? Well, some researchers have raised doubts about this assumption. Let us try to examine why.
First, in support of the commonsense clinical argument, most studies have shown a moderate but robust correlation between DUP and various indices of outcome [1–7]. Others have failed to find this for reasons that are currently unclear [8,9]. While the association does seem robust, cross-sectional evidence regarding longitudinal relationships may be quite misleading, as Kraemer et al. have recently emphasised [10]. In this case, a misleading impression could be gained through selective omission of different subsets of the DUP distribution in different studies. This is something that is almost certain to occur, for example people with longer DUP are more likely to refuse participation in research studies [11]. In some settings, short DUP cases may not make it into the clinical setting because of access problems or because short DUP cases may contain a higher proportion of self-limiting cases [11,12].
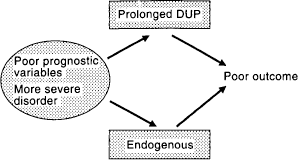
The implication that the association between DUP and outcome reflects a direct causal relationship has also been criticised because alternative explanations exist. First, more fundamental prognostic features reflecting severity of illness, such as poor premorbid functioning, high negative symptoms, strong family history and gender might produce greater delays in treatment and a worse outcome. In this model (Fig. 1), DUP would be an epiphenomenon and the link between DUP and outcome is confounded by a third group of variables. The second possibility (Fig. 2) is that DUP genuinely has a direct effect on outcome, either through the psychosocial damage that occurs in a developing adolescent or young adult during this period or via the notional process of biological toxicity of untreated psychosis [13,14]. The so-called indicators of severity, such as poor premorbid functioning or gender, might actually produce their effects by creating delays in treatment. The third model (Fig. 3), which could be termed the hybrid model, allows for a contribution of both pathways, that is, a more ‘intrinsic’ direct effect of gender, say, on outcome and a second direct effect of DUP. Timing of treatment could be affected by factors in the patient (intrinsic), factors in the environment and factors in the service system, including clinicians. The last model seems to have the most face validity and, indeed, is supported by the correlational data we have. For example, we found that even when more ‘intrinsic’ variables were entered into a regression model first, there was still a significant amount of a outcome variance explained by DUP [15]. Depending on whether DUP was entered first or later into the regression, model 2 or model 3 could be supported.
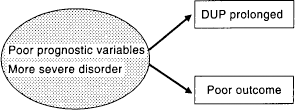
Duration of untreated psychosis as an epiphenomenon

Duration of untreated psychosis as an intervening variable
A hybrid model
Other data suggest that the effect of DUP on outcome may only begin to be exerted after approximately 1 month and can be mitigated by the effect of treatment, although this effect is time-limited [16]. The Suffolk County study no longer found a relationship between DUP and 24-month outcome, again suggesting that, with the passage of time, other variables, such as treatment, compliance and social environment may dilute the effect of DUP [9].
In any event, other designs have been proposed or utilised to examine the issue of causality. Wyatt [13,17] reanalysed the data from the randomised controlled trial of May et al. [18], which effectively compared patients who were exposed to neuroleptics at different points following entry to treatment on a random basis. This study showed a major advantage where the DUP, as defined by time to commencement of antipsychotic medication, was relatively short. Similarly, in the studies of Waddington et al. [19] and Scully et al. [20], the DUP was varied on an essentially non-biased basis and still correlated with outcome, this time long-term outcome. This study depended on the variable time that patients had been ill at the point that antipsychotics became available and the only other possible alternative explanation for the findings could have been a form of cohort effect.
This body of evidence has not been sufficient to convince a number of sceptical researchers (e.g. Verdoux et al. [21]) and hence other designs have been considered.
The quasi-experimental design for DUP: is it sufficient?
An alternative, quasi-experimental design termed ‘adequate’ has been proposed and implemented by McGlashan and colleagues [22]. This involves a two-step process, first, aiming to reduce the duration of DUP and second, estimating whether the outcome is correspondingly improved. This is similar to what has been attempted in the Early Psychosis Prevention and Intervention Centre (EPPIC) program in Australia on a large scale continuous naturalistic basis and also in a small experimental study. However, here it was found that a floor effect was present to some extent and there were also secondary effects of these interventions, which altered the composition of the clinical sample through effects on treated incidence [23]. The Scandinavian design involves an experimental sector where greatly enhanced detection systems have been systematically introduced, and two control sectors, in which similar treatment was offered but detection was not improved [22,24]. The early results appear promising in having substantially reduced DUP in the experimental sector, however, a number of unforeseen methodological problems have surfaced, which make interpretation complex. The enhanced detection intervention is powerful, so that in addition to reducing DUP for those cases who would have been detected under usual conditions, two new previously untapped sources of treated incidence have been accessed. Certainly, the treated incidence in the experimental sector has been substantially increased compared with the previous pilot study [25]. First, brief, self-limited psychoses, psychotic-like phenomena and non-clinically significant psychoses [26], which are more prevalent than previously realised, especially in young people [21], will be identified. Second, a long DUP subgroup similar to the untreated group that was described in Padmavathi et al. [27] should also be detected. In the Melbourne system, some of the first group have been channelled to the Personal Assistance and Crisis Evaluation (PACE) clinic for potential prodromal patients [28]. The latter group, however, has been clearly identified in a pilot study based on the Scandinavian design, which actually showed a longer DUP occurring with more vigorous detection efforts [23]. It is likely that the Scandinavian study will clarify the issue because of the scope for DUP reduction in the local system and the power of the early detection intervention, provided the focus is confined to a subgroup of the sample. However, other methodological problems that have arisen include the tendency for long DUP cases to refuse participation in the study [7,11] (see Fig. 4 and Fig. 5).
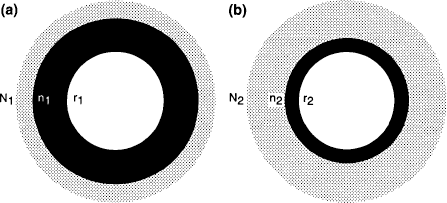
Quasi-experimental design, (a) Enhanced detection, (sector A). (b) Detection as usual (sector B). N, total annual incidence; r, research cohort; n, treated annual incidence
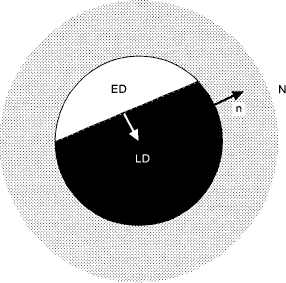
Dual effect of enhanced detection on duration of untreated psychosis and treated incidence. n, Treated incidence; N, total incidence; ED, early detected; LD, late detected
Conclusions
The intense interest in early psychosis in recent years has certainly helped us to appreciate the complexity that lies behind the simple logic of early detection. How should we respond to this complexity and the series of questions that arise from it?
On a clinical level, I believe it is critical for professionals and service systems to make every effort to provide easy access and promote engagement for clearly diagnosable and treatable first-onset psychosis. It is so counter-intuitive that this would not be helpful that the onus of proof should be on the sceptics to refute this. Another aspect of this task is the need to improve mental health literacy and trust in mental health interventions within the general population and among referrers, including those involved in primary care.
On a research level, we need to ask ourselves what needs to be proven and what level of proof will suffice. I believe that the unresolved question in relation to DUP and delayed treatment is whether such delays affect the medium- to long-term course of illness. We already know that response to acute or very short-term treatment (e.g. < 3/12) is much better with antipsychotic medication and supportive psychosocial interventions. This fact has made it questionable as to whether a further randomised controlled trial of early versus delayed neuroleptic treatment would be ethical.
How could this issue be examined in an ethical way? The quasi-experimental design of McGlashan and colleagues is one method [22], however, as noted, there are sampling problems with this that could weaken the inferences that will be drawn from the study. There are two additional options. First, the subset of patients who, although frankly psychotic, are not at immediate risk of rapid further deterioration, self-harm or aggression, could be invited to help resolve this research question through participation in a randomised controlled trial. Some patients would be competent to consider this request and could be informed about the possible short-term risks. This competence could be carefully assessed [29]. These short-term risks could be minimised by only delaying the antipsychotic drug component of acute treatment and offering intensive psychosocial support and frequent monitoring, with a 24-h emergency response. Indeed, in the real clinical world at present, such patients often request or demand a period of delay for drug therapy as they consider whether to trust the recommendations of clinicians and build engagement. Notwithstanding the evidence base, many competent people with early psychosis reject or wish to think about whether to take antipsychotics. I believe that such an approach would be ethical provided such potential subjects are fully aware of the finite risks involved. Second, in populations where a small minority of people with psychotic illness ever receive treatment, there is a strong case for increasing the availability of modern treatments and, especially, novel antipsychotic medications. This cannot be done in a universal manner across the population at the same point in time, but could be done in a carefully staggered manner, opening up services and access to care sequentially. This would mean that people would be commenced on drug treatment at different time intervals from the onset of their symptoms, but the factor determining the timing would be independent of their clinical picture and the potential intrinsic ‘severity’ factors referred to previously. This would be ethically more acceptable than carrying out a randomised controlled trial of antipsychotic medications versus placebo in such a population.
As with all good clinical research, we have learned many new things about this emerging frontier of preventive psychiatry. Undoubtedly, we shall learn more as more carefully designed studies are planned and implemented. A balance between enthusiasm, momentum for implementation of knowledge and expert opinion, and sound research evidence will be vital if rapid progress is to continue. The stakes are high. Losing the balance, either in the direction of zealotry or scepticism will create delay and may result in the failure and atrophy of this paradigm, an outcome with very serious consequences for patients and families.