
Abstract
Objective
To evaluate measures of schizotypy as familial risk factors for schizophrenia with the aim of making recommendations for assessing schizotypy as part of screening procedures for identifying people at risk of schizophrenia.
Method
Published studies using self-report and interview-based measures of schizotypy to assess relatives of patients with schizophrenia are reviewed. A parent study is reported evaluating the diagnostic accuracy of parental schizotypy as assessed by three questionnaire-based measures: the Chapman Perceptual Aberration and Physical Anhedonia Scales, and the Eysenck Psychoticism Scale. Group scores for these self-report ratings of 23 parent-pairs of patients with schizophrenia, 20 parent-pairs of patients with chronic nonpsychotic psychiatric disorder, and 19 parent-pairs of healthy comparison subjects are compared.
Results
Consistent with published evidence that self-report measures of psychosis-proneness and schizotypy do not consistently reflect familial risk factors that are specific for schizophrenia, scores on questionnaire measures of schizotypy did not distinguish the parents of patients with schizophrenia from the parents in the other two groups.
Conclusions
Interview-based assessments of schizotypy better assess familial risk factors than self-report measures of schizotypy. Questionnaire measures of schizotypy should be supplemented by interview-based assessments when screening for individuals at risk of schizophrenia.
Bleuler concluded that the familial liability to schizophrenia expressed itself more commonly as the chronic neurotic and character disorders that he considered formes fruste of schizophrenia [1]. Bleuler named these conditions latent schizophrenia in which he considered could be seen in nuce all the symptoms that are present in manifest schizophrenia [1, pp. 335–336].
The disease appears in an even more pernicious light when we take into account that a vast multitude of psychopaths, who are not considered as mentally ill and who keep their families and society as a whole on edge all the time, as well the neuropaths who keep the doctors busy without their being able to effect any cures, are latent schizophrenics. I have reason for the assumption that these latent unrecognised schizophrenics are by far more numerous than the overtly diseased.
These observations were convincingly confirmed in the Danish-American Adoption Studies. Kety reported rates of chronic schizophrenia of 3% and rates of schizotypal spectrum disorders of 21% in the biological relatives of adoptees who developed schizophrenia, while the corresponding rates for the biological relatives of adoptees screened as mentally healthy (and their adoptive families) were 0% and 6% [21. The DSM criteria for Schizotypal Personality Disorder were developed from the operational definition of the diagnosis of ‘borderline schizophrenia’ used in the Danish-American Adoption Studies [3]. Re-analysis of the original ‘spectrum’ diagnoses using DSM criteria strengthened the evidence that there was a genetic relationship between schizotypal disorders and schizophrenia, and that schizotypal disorders are the most frequently expressed phenotype of schizophrenia [4]. This type of familial aggregation has been consistently replicated using interview-based assessments of schizotypal disorders [5–7].
In terms of interview-based instrumentation, there are two schedules designed specifically for assessing schizotypal disorders that have been used in family studies: Schedule for Schizotypal Personality (SSP) [8] and Structured Interview for Schizotypy (SIS) [9]. General personality disorder interviews have also been used to assess schizotypal disorders in family studies: the Personality Disorder Examination (PDE) [10] and Structured Interview for DSM-III-R Personality Disorders (SIDP) [11]; however, studies using these instruments have produced less consistent results compared with studies that used schedules specifically designed to detect schizotypal disorder.
The aforementioned categorical approach to the assessment of schizotypal disorders has been complemented by dimensional measures developed mainly by psychologists. This approach is based on the view that degrees of schizotypy are widely distributed in the general population. To enable the study of large normative samples, the 19 schizotypy scales available are all in the form of self-report questionnaires [12]. The most commonly used are the Chapman scales (Perceptual Aberration Scale [13]; Physical Anhedonia Scale and Social Anhedonia Scale [14]; Magical Ideational Scale [15]; and Psychoticism [16]).
Use of self-report questionnaire ratings in family studies has not produced clear-cut evidence that these measures tap phenotypic aspects of the predisposition to schizophrenia. Claridge and coworkers [17] administered the Psychoticism scale and the Schizotypy-A Scale (STA) [18] to 56 relatives of patients with schizophrenia and 43 relatives of ‘neurotic’ patients. Although psychoticism scores were higher in the relatives of patients with schizophrenia than in the relatives of ‘neurotic’ patients, against prediction, scores on the STA scale were significantly lower in the relatives of patients with schizophrenia versus relatives of ‘neurotic’ patients. Using a different self-report measure called the Munich Personality Test, Maier et al. found no differences in the scores on the three schizotypy scales (reflecting schizoidia, unsociability and eccentric preoccupations) between three groups of relatives of patients with schizophrenia, unipolar depression and healthy controls [19]. Katsanis and coworkers compared the scores of relatives of patients with schizophrenia with scores of healthy controls on the Social Anhedonia, Physical Anhedonia, and Perceptual Aberration Scales [20]. Compared to the healthy subjects, relatives of patients with schizophrenia scored significantly higher on physical and social anhedonia, but against prediction, scored lower on perceptual aberration. Both Claridge et al. and Katsanis et al. suggested that low self-report schizotypy scores in relatives of patients with schizophrenia may be related to defensive response set.
Grove et al. reported that 61 relatives of patients with schizophrenia scored significantly higher for physical anhedonia but the same for perceptual aberration when compared with 18 healthy screened controls [21]. Clementz et al. reported that relatives of patients with schizophrenia obtained higher scores for physical anhedonia but, against prediction, did not score more highly on perceptual aberration compared with normal controls or their relatives [22]. Franke and coworkers compared 57 patients with schizophrenia to 32 of their healthy siblings and 32 healthy screened controls [23]. The healthy siblings scored more highly on physical anhedonia, but not more highly on perceptual aberration when compared with the healthy control group.
There is only one report of a direct comparison of the performance of interview-assessed and self-report questionnaire-based measurement of schizotypy. Kendler et al. compared the diagnostic accuracy of self-report and interview-assessed schizotypy measures in first-degree relatives of four groups of psychiatric patients diagnosed according to DSM-III-R [24], namely: (i) schizophrenia (n = 265–295 relatives); (ii) other nonaffective psychosis (n = 208–259 relatives); (iii) affective psychosis (n = 183–200 relatives); and (iv) nonpsychotic affective disorder (n= 158–176 relatives) and first-degree relatives of a representative unscreened sample of the general population (n = 416–564 relatives). Six of the seven interview-based schizotypy factor scores discriminated relatives of patients with schizophrenia from relatives of the general population sample [25]. Of the three self-report measures (psychoticism, magical ideation and social anhedonia), only social anhedonia scores distinguished relatives of the general population sample with schizophrenia from relatives of controls. In a direct estimate of relative predictive power of interview-based and self-report measures, interview-based measures had significantly greater predictive power than the self-report measures in 16 of the 18 comparisons made [24]. This study could be criticised on the grounds that the self-report scales were abbreviated (with the assistance of the scale designers). However, this potentially mitigating factor in demonstrating predictive power of self-report scales seemed more than offset by the power of the study in terms of sample size. Moreover, the pattern of findings was consistent with published family studies.
In summary, family studies of schizotypy suggest that interview-based measures are successful at assessing underlying familial vulnerability to schizophrenia. In fact, Faraone and coworkers estimated that interview-based measures of schizotypy have greater diagnostic accuracy in terms of assessing the phenotype of schizophrenia than the diagnostic category of schizophrenia itself [26]. However, the evidence for self-report measures of schizotypy successfully tapping the phenotype in relatives of patients with schizophrenia is still not clear. Therefore, we now report a study of self-report schizotypy in parent-pairs of three groups of index subjects; namely, patients with schizophrenia, patients with chronic nonpsychotic psychiatric disorder and healthy controls.
Method
Subjects
Parent-pairs were identified through index-offspring. Patient-offspring were recruited from the Eastern Sydney Area Health Service (Sydney, Australia) from individuals who were past or present inpatients in the psychiatric wards of two Sydney public general teaching hospitals, The Prince of Wales and Prince Henry Hospitals. Diagnosis was made on the basis of a Present State Examination (PSE) [27] interview and review of available case notes. Twenty-three index patients who satisfied the diagnostic criteria of the ICD-9 [28] for schizophrenia provided 23 parent-pairs that were grouped. Only 19 of these 23 index-patients satisfied DSM-III-R [29] criteria for schizophrenia, the reminder attracting the diagnosis of DSM-III-R schizoaffective disorder. Twenty index patients who met ICD-9 and DSM-III-R criteria for nonpsychotic, nonorganic psychiatric disorder provided 20 parent-pairs that constituted a second parent group. All nonpsychotic index patients met DSM-III-R criteria for an axis I diagnosis (mood disorder: n = 8; anxiety disorder: n = 9; eating disorder: n = 3) and all but two cases satisfied criteria for an axis II diagnosis of personality disorder. The two clinical index-patient groups were well matched for age of onset of illness (schizophrenia group: 18.3 ± 4.5 years; nonpsychotic group: 17.2 ± 5.4 years) and duration of disabling symptoms (schizophrenia group: 5.2 ± 3.8 years; nonpsychotic group: 4.1 ± 3.8 years). The 19 healthy index-offspring providing parent-pairs were recruited by public advertising, from a church group and by personal association. The healthy index-subjects had never received psychiatric treatment, did not satisfy the diagnostic criteria of ICD-9 for any disorder, and were rated zero on all items in the Behaviour, Affect and Speech Section of the PSE.
Across the three index groups, there were no significant differences in age, sex ratio and education level. Both clinical index groups were of significantly lower socioeconomic status, estimated IQ and were less frequently married compared to the healthy index group. Across the three parent-pair groups, there were no significant differences in age (all parent groups had a mean age of about 55 years), estimated IQ, education level, socioeconomic status or marital status.
Procedure
Index subjects and their parent-pairs underwent an extensive clinical, psychometric and electrophysiological assessment lasting about 4 h in total, as described elsewhere [30,31]. Psychometric testing did not occur until patients were much improved and able to cooperate. Informed consent was obtained from all subjects.
The self-report questionnaire measures of interest to this report are as follows: (i) the Eysenck Personality Questionnaire (EPQ) [16]; (ii) the Perceptual Aberration Scale (PAS) [13]; and (iii) the Physical Anhedonia Scale [14].
Data Analysis
Parametric analyses were employed after skewed data were normalised by square root transformation. Of the EPQ scales, Extroversion or E-score, neuroticism or N-score and psychoticism or P-score were included in the analysis.
Results
Psychosis-Proneness and Schizotypal Measures in the Index Groups
Descriptive statistics are listed in Table 1.
Psychometric results for index groups
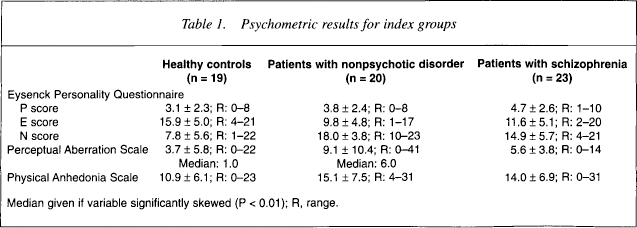
Median given if variable significantly skewed (P < 0.01); R, range.
Anova across the three groups indicated that there were differences in PAS scores (F2,56 = 5.03, p = 0.01), and Physical Anhedonia scores (F2,56 = 1.83, p = 0.17) at the level of a trend. Compared with the healthy controls, patients with schizophrenia (p < 0.015) and patients with nonpsychotic disorders (p < 0.009) obtained higher scores for PAS, but the PAS scores for the two clinical groups did not differ significantly. Compared to healthy controls, nonpsychotic patients obtained significantly higher scores for Physical Anhedonia (p < 0.001). Against prediction, there was a trend for the patients with schizophrenia to obtain lower Physical Anhedonia scores (p < 0.08).
Psychosis-Proneness and Schizotypal Measures in the Parent Groups
Descriptive statistics are listed in Table 2.
Psychometric results for parent groups
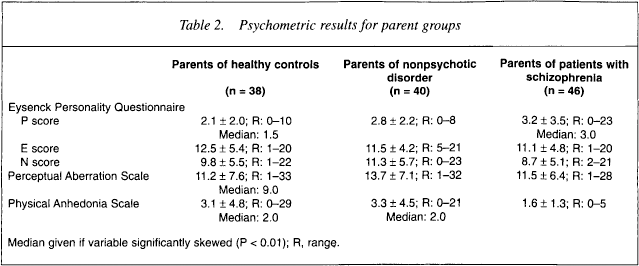
Median given if variable significantly skewed (P < 0.01); R, range.
Anova across the three parent groups indicated that there were statistically nonsignificant trends for a difference in PAS scores (F2,116= 1.67, p = 0.20) and Physical Anhedonia scores (F2,115 = 1.46, p = 0.24). Against prediction, the parents of patients with schizophrenia scored significantly lower on the PAS than parents of healthy controls (p = 0.04). Perceptual Aberration scores for parents of patients with nonpsychotic disorder did not differ from those of the parents of healthy controls. There was a strong trend for parents of patients with nonpsychotic disorders to obtain higher PAS scores compared to the parents of patients with schizophrenia (p = 07). Compared with the parents of healthy controls, parents of patients with schizophrenia did not obtain higher Physical Anhedonia scores. Compared to parents of both healthy controls (p = 0.05) and patients with schizophrenia (p = 0.08), parents of patients with nonpsychotic disorder obtained higher Physical Anhedonia scores.
Correlations between Eysenck Personality Questionnaire Scales and Schizotypy Measures
The E-score and the N-score were significantly negatively correlated in the index groups combined (r = −0.37, p < 0.01) but not in the parent groups combined. Extroversion was significantly negatively correlated with Physical Anhedonia (r = −0.31, p < 0.001), but only in the total parent group. Ratings of Physical Anhedonia were not correlated with the P-score or PAS ratings in the parent groups combined. There was a weak negative correlation between Physical Anhedonia and P-score in the patient groups combined (r = 0.27, p < 0.05).
Correlation between Parental and Offspring Eysenck Personality Questionnaire and Schizotypy Scores
The across-generation correlation of psychometric measures was calculated between the mid-parent score (average for a parent-pair) and the offspring score for each family triplet. This correlation provides an upper estimate of heritability for the psychometric measure. Extroversion (r = 0.31, p < 0.01) and Physical Anhedonia (r = 0.49, p < 0.001) showed significant across-generation correlations; that is, significant heritability. Psychoticism, PAS and neuroticism were not correlated across-generation.
Predicting Index Group Membership with Parental Eysenck Personality Questionnaire and Schizotypal Measures
Using mid-parent scores of psychometric measures in regression analysis, parental P-score ratings significantly predicted offspring clinical group membership, but did not significantly predict membership of the schizophrenic group. There was a statistically nonsignificant trend for parental E-score to predict the offspring membership of a clinical and schizophrenic group. Parental N-score had no predictive value. Mid-parental Physical Anhedonia scores did not significantly predict membership of the schizophrenic index group, but there was a weak trend for these ratings to predict clinical group membership (p = 0.17). Mid-parent PAS scores did not predict offspring membership of a clinical group, although there was a trend for parental PAS score to predict index offspring membership of the schizophrenia group (p = 0.07). An attempt to obtain a discriminant function that significantly predicted index group membership from mid-parent P-scores, and PAS and Physical Anhedonia ratings by using simple stepwise discriminant function analysis was unsuccessful.
Discussion
The present study found that P-score was significantly elevated in the index group of patients with schizophrenia, supporting the validity of this measure in demonstrating clinical group differences. Consistent with previous reports [16], E-score was significantly reduced and N-score was significantly increased in both clinical index groups. The score for psychoticism was significantly elevated in the parents of patients with schizophrenia and in parents of patients with nonpsychotic disorder, supporting this measure as a nonspecific familial risk factor for psychiatric disorder and not necessarily as a measure of schizotypy. There was a trend for E-score to be lower in the parents of patients with schizophrenia; the importance of this finding highlighted by the significant heritability of E-score detected in this and other studies.
Perceptual Aberration Scale was significantly elevated in both patient index groups compared to healthy controls, supporting the validity of PAS as a correlate of psychopathology. Physical Anhedonia was significantly elevated in the index nonpsychotic patient group but not the group of patients with schizophrenia, which indicates that it, too, is a nonspecific correlate of psychopathology. The prediction that the parents of patients with schizophrenia would have higher schizotypy scale ratings, which was based on the assumption that they were familial vulnerability factors, was not fulfilled. Physical Anhedonia was not significantly increased in the parents of patients with schizophrenia, and PAS was actually reduced in these parents. The possibility that defensive responding reduced self-report schizotypy ratings cannot be excluded. Detection in this study of a significant estimate of heritability for Physical Anhedonia suggests consistency of results at least for this scale.
Considering the results together, the P-score, PAS or Physical Anhedonia scores do not appear to be specific familial risk factors for schizophrenia. Both P-score and Physical Anhedonia may be nonspecific familial vulnerability risk factors, perhaps for adolescent-onset psychopathology [32], but the PAS score seems more likely to be a correlate of psychopathology itself. Although these results argue against the conclusion that these self-report questionnaires specifically measure the phenotype for schizophrenia, these results do not refute the value of these questionnaire measures as part of screening procedures for risk factors for schizophrenia. In fact, there is increasing evidence that extreme self-reported schizotypy scores in apparently healthy college students are associated with a range of neurocognitive and other deficits associated with schizophrenia [23,33–35] and, on long-term follow-up, a substantial risk of developing serious psychotic illness [36,37]. These associations are most apparent when several different indicators of schizotypy are used. This is consistent with the results of the present study, which shows a relative absence of correlation between schizotypal measures, and other reports, all indicating that the risk for schizophrenia is multifactorial, as is schizotypy itself [12,35]. Therefore, to achieve acceptable predictive power in estimating the future risk of an individual for the development of schizophrenia, assessment of a range of risk factors, both schizotypal and others, will have to be made.
To conclude, the self-report questionnaire measures of schizotypy evaluated in this study and by literature review, appear to have only modest diagnostic accuracy in detecting the phenotype for schizophrenia. Interview-assessed schizotypy appears to have superior diagnostic accuracy. However, both interview-based assessments of schizotypy [38] and self-report questionnaires of schizotypy [36,37] appear to significantly measure future risk of developing schizophrenia.