
Abstract
Background
Exposing blood serum samples to ambient white light-emitting diode (WLED) light may accelerate bilirubin photoisomer production. We previously demonstrated the quantitative effect of bilirubin configurational isomers (BCI) on direct bilirubin (DB) value using the vanadate oxidation method. However, the effects of bilirubin structural photoisomers (BSI) remain unclear.
Methods
In Study 1, the relationship between WLED irradiation time and BSI production was examined. Serum samples from five neonates were irradiated with WLED light for 0, 10, 30, 60 and 180 min. Bilirubin isomer concentration and BSI production rates were calculated. In Study 2, we performed quantitative investigation of BSI effect on DB values: Differences in DB, BCI and BSI values before and after irradiation were calculated as ⊿DB, ⊿BCI and ⊿BSI, respectively. Assuming the coefficient of BCI affecting DB values was ‘a’, relational expression was ⊿DB = a*⊿BSI + 0.19*⊿BCI. Serum samples from 15 neonates were irradiated with green LED light for 10 and 30 s. The respective bilirubin isomer levels were measured, and the coefficient was derived.
Results
In Study 1, the median BSI production rate was 0.022 mg/dL per min in specimens with an unconjugated bilirubin concentration of 10.88 mg/dL. In Study 2, assuming that ⊿DB-0.19*⊿BCI was Y and ⊿BSI was X, the relational expression was Y = 0.34X-0.03 (R2 = 0.87; p < .01) and a = 0.34.
Conclusions
Under ambient WLED light, serum sample generated 1.3 mg/dL BSIs in 1 h. Approximately 34% (0.44 mg/dL) of BSI concentrations was measured as DB when using the vanadate oxidation method according to the above equation.
Introduction
The vanadate oxidation method is used to measure total bilirubin (TB) and direct bilirubin (DB) concentrations. In this method, TB measurement involves the use of a citric acid buffer solution containing a surfactant, and DB measurement involves the use of a tartaric acid buffer solution as the primary reagent. The secondary reagent for the TB and DB measurements is sodium metavanadate. The first absorbance is measured after mixing with the primary reagent, and the second absorbance is measured after mixing with the secondary reagent. The measurement wavelengths are 450 nm (primary wavelength) and 546 nm (secondary wavelength). The TB and DB values are calculated based on the absorbance change in the two absorbance measurements. 1
Direct and indirect bilirubin classifications are used when measuring DB with the diazo method; therefore, the term ‘direct bilirubin’ has also been used in bilirubin measurement in subsequent clinical testing. The DB concentrations measured with the diazo method do not necessarily coincide with the glucuronosyl bilirubin concentrations. This inconsistency is likewise recognized in the bilirubin oxidase and vanadate oxidation methods.2–5 The effect of δ bilirubin and bilirubin photoisomers (BPIs) is a reason that the DB values obtained with the vanadate oxidation method deviate from the glucuronosyl bilirubin concentrations.6,7
BPIs are generated by irradiating the light-sensitive complex of 4Z,15Z-bilirubin Ⅸα ([ZZ]-BR), which is an unconjugated bilirubin, and albumin. BPIs include bilirubin configurational photoisomers (BCIs) generated by cis–trans configurational isomerization reactions and bilirubin structural photoisomers (BSIs) generated by structural isomerization reactions (BPIs = BCIs + BSIs).8,9
BCIs include 4Z,15E-bilirubin Ⅸα ([ZE]-BR), 4E,15Z-bilirubin Ⅸα ([EZ]-BR), and 4E,15E-bilirubin Ⅸα ([EE]-BR), although only an extremely trace amount of [EE]-BR exists in human blood. [ZE]-BR and [EZ]-BR are generated in vivo under normal light environments, and exist in blood at approximately 10–20% of [ZZ]-BR (BCIs = [ZE]-BR + [EZ]-BR). 10
We previously reported that the DB concentrations were affected by the reaction of BCIs and BSIs with vanadate when using the vanadate oxidation method. 11 In addition, previous research indicated that approximately 19% of the BCIs concentration in specimens is quantitatively measured as DB. As a greater amount of BCIs exist in neonates in whom unconjugated bilirubin is physiologically more plentiful than in adults, the conjugated bilirubin concentrations greatly deviate from the DB values. 5 However, the effect of BSIs on DB values when using this measurement method has not been quantitatively evaluated.
BSIs include 4E,15Z-cyclobilirubin Ⅸα ([EZ]-CBR) and its configurational isomer 4E,15E-cyclobilirubin Ⅸα ([EE]-CBR), (BSIs = [EZ]-CBR + [EE]-CBR), with the former being generated by structural isomerization reactions, in which reversible reactions via [EZ]-BR are not prone to occur.12,13 BSIs are rapidly excreted, even if generated in a physiological state in vivo in humans; therefore, they exist only in trace amounts in blood. However, in test tube serum irradiated with light, BSIs have no excretory pathway. Hence, they are generated and accumulate in the serum. 10
The wavelength at which bilirubin photoisomerization reactions tend to occur is 400–520 nm. 7 Indoor ambient light in settings, such as clinical laboratories, is increasingly changed from white fluorescent lighting to white light-emitting diode (WLED) lighting. WLED is currently in widespread use, which combine blue LED with yellow fluorescent bodies (i.e. the complementary color), may generate more wavelengths to which bilirubin is sensitive, compared to fluorescent lighting, and, therefore, may be more prone to generate photochemical reactions in bilirubin. However, the generation of BPIs accompanying exposure to ambient WLED light and their effect on clinical bilirubin testing measurements have not been heretofore fully investigated. We hereby conducted a detailed examination of the generation of BSIs under a WLED environment, as well as their quantitative effects on DB values when using the vanadate oxidation method.
In humans, jaundice is physiological only during the neonatal period. An average TB of 12 mg/dL is typically observed at 6–7 days of age in Japanese term infants. Therefore, neonatal serum samples were collected, and the DB was evaluated using a TB concentration of 10 mg/dL as the threshold.
Methods
Leftover serum samples of neonates who were born at Kagawa University Hospital (Kagawa, Japan) and underwent blood draws for routine care were used as the specimens. The specimens were centrifugally separated in a dark location, shielded from light with aluminum foil, and stored frozen. At the time of the experiment, these specimens were used after having been thawed in a dark location. The institutional ethics committee of the Kagawa University Heisei approved the study (approval number: 30–188). The remaining specimens of blood collected for clinical testing were used, and a notice was posted on the Web regarding the use of the specimens.
Study 1 Relationship between white LED irradiation time and BSI production
The specimens of five neonates (five specimens for each neonate) were dispensed at 100 μL at a time. By using a WLED light source (Z-Light, Yamada Shomei, Tokyo, Japan) having the equivalent wavelength characteristics of lighting used in the central laboratory of Kagawa University Hospital, the specimens were irradiated for 0, 10, 30, 60 and 180 min, respectively, in a dark location where light, other than the light source, could not enter. The irradiance was 1.2 μW/nm/cm2 (MINOLTA Air-Shields 451-Fluoro-Lite Meter; Konica Minolta, Tokyo, Japan), which was the same irradiance of the location where the separated serum samples were placed in the central laboratory until they were measured. The BPIs of the respective specimens were measured with high-performance liquid chromatography (HPLC). The sum of the [ZZ]-BR concentration and BPI concentration (= [ZZ]-BR + ([ZE]-CBR + [EE]-CBR) + ([ZE]-BR + [EZ]-BR) was considered the unconjugated bilirubin Ⅸα (UCB) concentration, and the sum of the [EZ]-CBR and [EE]-CBR concentrations was defined as the BSI concentration. For the BSI concentration, the change from the start of irradiation was calculated and defined as the ⊿BSI, while the BSI generation rate was calculated from the ⊿BSI and the irradiation time.
Study 2 Quantitative investigation of the effect of BSIs on DB values
The irradiation of bilirubin with light generates BSIs and BCIs. In this study, minimizing the effect of BCIs to quantitatively examine the effect of BSI was necessary. For this purpose, the amount of change in BSIs in the specimens before and after irradiation was examined by using a light source with green wavelengths, at which few BCIs but many BSIs are generated. A green LED (Bili-therapy Spot type, Special machine for research; Atom Medical, Tokyo, Japan), which has a [ZE]-BR/[ZZ]-BR ratio of 0.15 during optical equilibrium, was the light source. A preparatory experiment was conducted using a green LED light (irradiance, 70.0 μW/nm/cm2; MINOLTA Air-Shields 451-Fluoro-Lite Meter; Konica Minolta). Once [ZZ]-BR and BCI reached an optical equilibrium state after 10 s irradiation, the irradiation time that generated the smallest amount of BCI change, compared to this specimen, and the amount of BSI sufficient to enable a quantitative examination was 30 s.
The specimens of 15 neonates were separated into two samples, 200 μL each. These samples were, respectively, irradiated for 10 and 30 s, and the TB, DB and BPI concentrations were measured. The differences in DB, BCI and BSI concentrations before and after irradiation were defined as ⊿DB, ⊿BCI and ⊿BSI, respectively. Assuming the coefficients of the BCIs and BSIs affecting the DB values were a and b, the relational expression of ⊿DB = a*⊿BSI + b*⊿BCI was established. In our previous report, b was 0.19. 5 In this study, the coefficient a was derived from the measurement results.
Measurement methods
The HPLC measurement method described by Itoh et al. 14 was used with the Shimadzu LC-20AD HPLC system (Shimadzu Co., Kyoto, Japan). The column used was the Nova-Pack C18 radial compression cartridge (5 mm × 10 cm; Nihon Waters KK, Osaka Japan). Acetonitrile, 0.01 M phosphate buffer (pH 5.5), and dimethylformamide mixed at a ratio of 5:30:65 (v/v/v) was defined as Solution A. When mixed at a ratio of 20:15:65 (v/v/v), it was defined as Solution B. By using the gradient elution method, Solution B varied from 0% to 34% for 17 min and, then, it was 100% for 8 min. The flow rate was assumed to be 1 mL/min. The SPD-20AV detector (Shimadzu Co.) was used, and the detection wavelength was 455 nm. The specimens were mixed with dimethyl sulfoxide and acetonitrile at volumetric ratios equivalent to those of the specimen in a vortex mixer and, then, centrifuged. Thereafter, 25 μL of the supernatant was injected into the HPLC analyzer for analysis. The area of each peak was calculated by absorbance at 455 nm, and the quantitative calculation was performed using the relative ratio of molar absorption coefficient of [ZZ]-BR.
For DB measurements, the Total Bilirubin E-HA Test and Direct Bilirubin E-HA Test (Wako Co., Tokyo, Japan) were used as the measurement reagents. Measurements were obtained with the TBA-C16000 analyzer (Canon Medical Systems Co., Otawara City, Japan) at the central laboratory.
Statistical procedures
For the relationship between the WLED irradiation time and BSI production, a linear regression analysis of the light exposure time and BSI was conducted, and the slope was treated as the generation rate. In the experiment of the effect of BSI on DB values, we conducted linear regression analysis of ⊿BSI and ⊿DB - 0.19*⊿BCI. A p-value of <.05 was statistically significant. Statistical analysis was conducted using Prism version 6.0 for Windows (GraphPad Software, San Diego, CA, USA).
Results
Study 1 Relationship of white LED irradiation time and BSI production
The pre-light irradiation UCB concentration of the five specimens [presented as the median (range)] was 10.88 (9.82–13.32) mg/dL and the BSI concentration was 0.09 (0.05–0.94) mg/dL. After 10, 30, 60 and 180 min of irradiation, the ⊿BSI was 0.28 (0.18–0.33), 0.85 (0.66–0.88), 1.56 (1.29–1.91) and 3.95 (3.33–4.76) mg/dL, respectively. The slope of the linear regression formula was 0.022 (0.018–0.026), and R2 was 0.99 (0.99–1.00) (Figure 1). There was no significant correlation between the TB value of each sample and the rate of BSI generation. Based on this finding, the BSI generation rate under the same conditions was 0.022 mg/dL per min and 1.32 mg/dL per hour. Study 1: The relationship between white LED irradiation time and BSI production in the serum samples of five neonatal patients (labeled A–E). BCI: bilirubin configurational isomer; BSI: bilirubin structural isomer; DB: direct bilirubin; LED: light-emitting diode.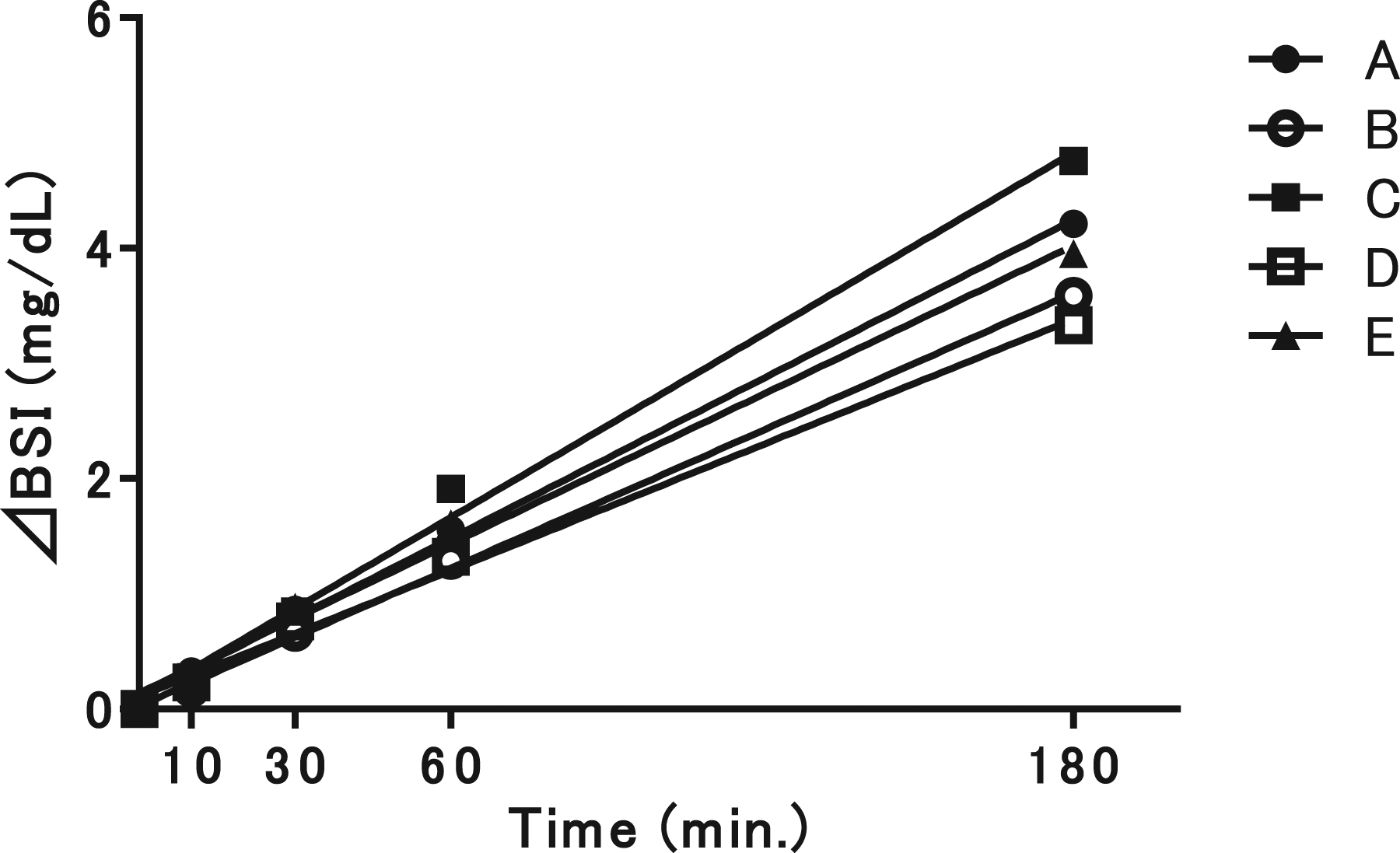
Study 2 Quantitative investigation of the effect of BSIs on DB values

Changes in total bilirubin, direct bilirubin and bilirubin photoisomer concentrations between the 10-s and 30-s irradiation groups.
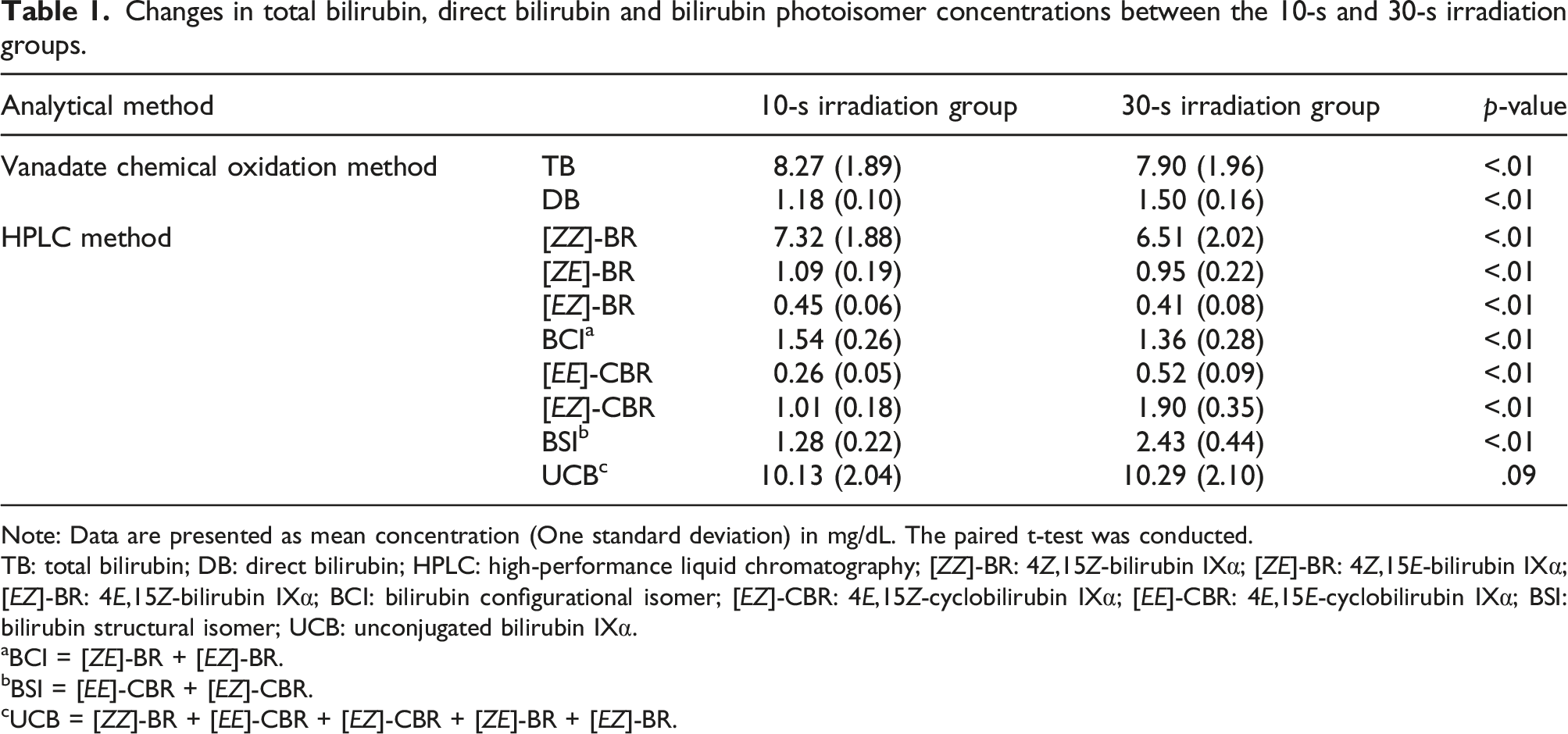
Note: Data are presented as mean concentration (One standard deviation) in mg/dL. The paired t-test was conducted.
TB: total bilirubin; DB: direct bilirubin; HPLC: high-performance liquid chromatography; [ZZ]-BR: 4Z,15Z-bilirubin Ⅸα; [ZE]-BR: 4Z,15E-bilirubin Ⅸα; [EZ]-BR: 4E,15Z-bilirubin Ⅸα; BCI: bilirubin configurational isomer; [EZ]-CBR: 4E,15Z-cyclobilirubin Ⅸα; [EE]-CBR: 4E,15E-cyclobilirubin Ⅸα; BSI: bilirubin structural isomer; UCB: unconjugated bilirubin Ⅸα.
aBCI = [ZE]-BR + [EZ]-BR.
bBSI = [EE]-CBR + [EZ]-CBR.
cUCB = [ZZ]-BR + [EE]-CBR + [EZ]-CBR + [ZE]-BR + [EZ]-BR.
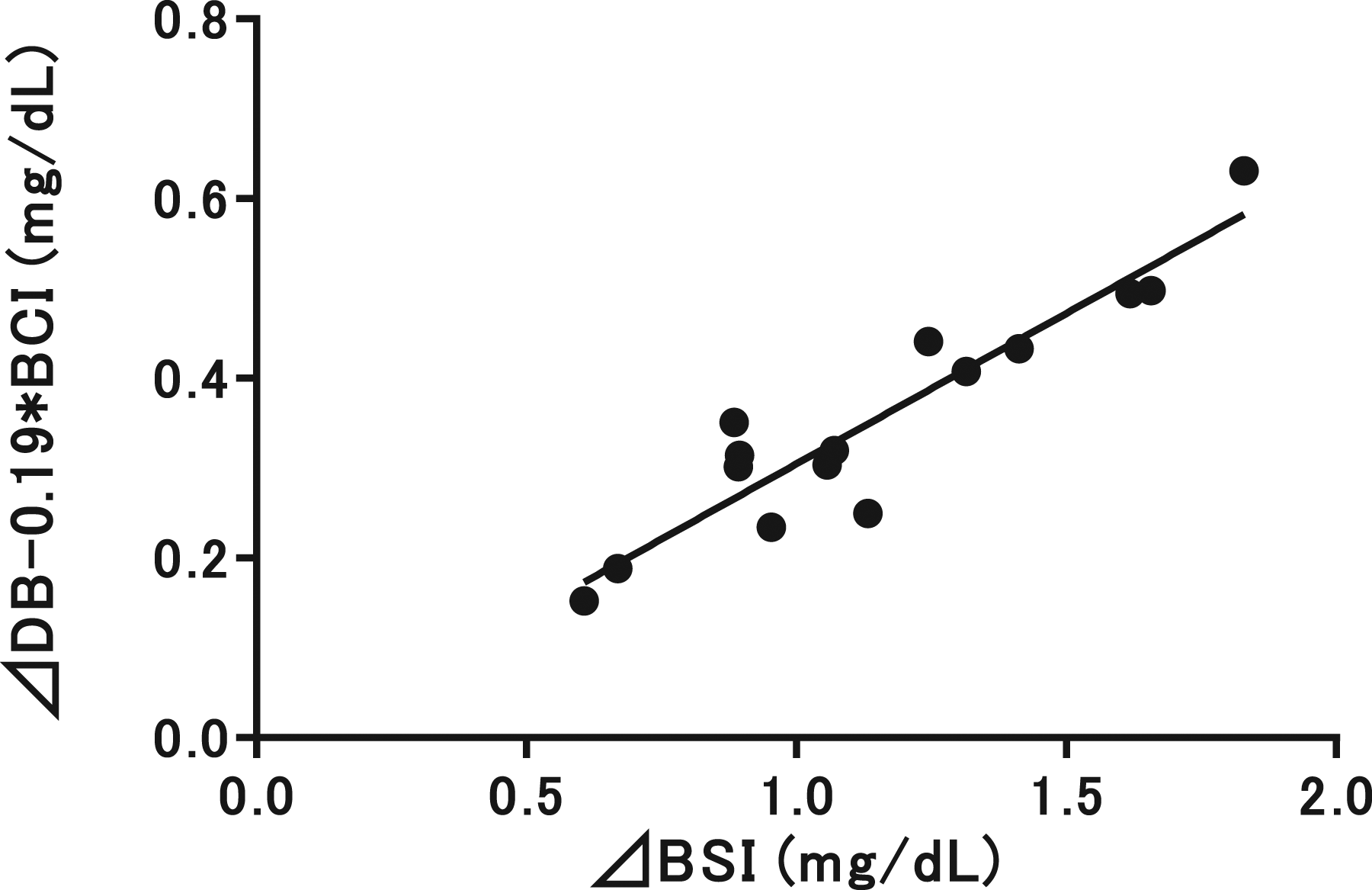
Study 2: The relationship between the amount of DB value increase due to BSIs (i.e. ⊿DB - 0.19*⊿BCI) and the amount of increase in BSIs (i.e. ⊿BSI). The x-axis shows the increase amount in bilirubin structural isomers (i.e. ⊿BSI), and the y-axis shows the increase in the amount of direct bilirubin due to bilirubin structural isomers (i.e. ⊿DB - 0.19*⊿BCI). Note: Y = 0.34X - 0.031 (R2 = 0.87, p < .01). BCI: bilirubin configurational isomer; BSI: bilirubin structural isomer; DB: direct bilirubin; LED: light-emitting diode.
If intercept 0.03 was ignored because it was close to zero, then, the a-value was 0.34 in the relational expression: ⊿DB = a*⊿BSI + 0.19*⊿BCI.
Discussion
The changeover from white fluorescent lights, which have primarily been used until recently as the light source for indoor illumination, to white LEDs has been progressing in recent years. When the spectra of the light sources are compared, white fluorescent lights used in indoor lighting create the white color by synthesizing the emissions of three wavelengths of fluorescent light in blue (450 nm), green (550 nm) and red (610 nm), which are the three primary colors of light. However, owing to the characteristics of fluorescent light, the green and red wavelengths are strong, whereas the blue wavelength is relatively weak. However, as the most widely used WLEDs produce white light by combining blue LEDs with fluorescent bodies that are yellow, which is the complementary color, they are characterized by a greater volume of light energy in the 450-nm blue wavelength region than that found in white fluorescent lights. The λmax of bilirubin is 450 nm, and BPIs are efficiently generated at wavelengths of 400–520 nm. A proposed hypothesis is that the generation rate of BPIs in specimens increased by irradiation with ambient WLED light containing a blue LED and a complementary color compared to irradiation with white fluorescent lights. In this study, we ascertained that BSIs were produced at a rate of 0.022 mg/dL per min on the irradiation of serum with a TB concentration of approximately 10 mg/dL, and that 1.32 mg/dL of accumulation in the serum specimen occurred in 1 h.
To investigate the effect of BSIs on DB measurement values, we examined the DB measurements after having converted the two parameters of BSI and BCI, which differ in the molecular extinction coefficient, into a single parameter, assuming that approximately 19% of the BCI concentration was measured as the DB value. We derived the difference in the DB increase owing to BCIs based on the increase in the DB value (i.e. ⊿DB - 0.19*⊿BCI). Considering this amount as the amount of DB increase owing to BSI (i.e. a*⊿BSI), we conducted a linear regression analysis with the BSI increase amount (i.e. ⊿BSI) and examined whether the coefficient a could be calculated as a = (⊿DB - 0.19*⊿BCI)/⊿BSI). As a result, ⊿BSI and (⊿DB - 0.19*⊿BCI) exhibited a significant positive correlation; the intercept was close to 0 in the approximate linear formula, while the slope was 0.34. Therefore, calculating coefficient a was possible. We thereby calculated that a = 0.34, and we believe that BSI (1 mg) is reflected by the increase in DB (0.34 mg/dL).
Based on these results, we ascertained that the apparent DB measurement would increase by approximately 0.45 mg/dL when a neonatal serum sample containing a TB concentration of 10 mg/dL is exposed to ambient WLED light for 1 h. Only trace amounts of conjugated bilirubin exist in the serum of healthy neonates, and this amount does not change substantially on irradiation with light. In addition, on account that the DB measurement system has no substance other than bilirubin, which absorbs light at the 450-nm wavelength and exhibits large changes in the concentration because of irradiation with light, we believe that the increase in DB values was caused by changes in the amount of BPIs in the specimens.
In Study 2, we believe that the TB values significantly decreased, despite the lack of significant change in the UCB concentration between specimens irradiated for 10 s and those irradiated for 30 s because the relative molar absorption coefficient for [EZ]-CBR and [EE]-CBR was 0.47 and 0.39 for [ZZ]-BR at 450 nm. 14 Thus, we believe that this finding occurred because of the fact that [ZZ]-BR decreased and BSI increased at 450 nm, which was the bilirubin measurement wavelength used for the TB measurement. Therefore, the absorbance at 450 nm decreased at the time of measurement and the measured TB concentration was lower than the actual concentration.
The management guidelines of the American Academy of Pediatrics stipulate that abnormal accumulation of conjugated bilirubin occurs when the DB concentration is ≥ 1 mg/dL and the TB concentration is < 5 mg/dL as well as in cases where the DB is ≥ 20% of the TB and the TB concentration is > 5 mg/dL. Therefore, in cases where the TB is 10 mg/dL, the threshold value is DB = 2.0 mg/dL. 15 However, evidence is lacking. Under the conditions, in which the specimens were placed without light shielding in a bright light environment in the present study, the DB values deviated from the conjugated bilirubin concentration because of the accumulation of BSIs and, therefore, they could cause erroneous clinical judgments. When measuring the DB values by the vanadate oxidation method, it is strongly recommended that the blood sample should be shielded from light after collection until testing.
This study had some limitations. First, we examined the effect of ambient WLED light in specimens with a TB concentration of 10 mg/dL; however, the degree to which BSI accumulation will occur in specimens with different TB concentrations remains unclear. Second, the results may differ greatly, depending on the type of LED light source, and the reproducibility of the current results is limited only to light sources with the same wavelength characteristics of the light source used. Third, the effect of BSIs was calculated under the assumption that no effect was caused by bilirubin-derived substances, other than the BPIs measured, and the effects of bilirubin-derived substances, such as polymerized cyclobilirubin as well as tripyrroles, dipyrroles and monopyrroes of [ZZ]-bilirubin oxidation products were not considered.
In clinical testing, the exposure of certain substances, such as vitamin B2 to light, affects test results, and light shielding measures after a blood draw have been adopted for these substances. 16 The necessity of light shielding measures has heretofore not been strongly recommended for bilirubin fraction measurements. However, based on the results of the present study, we believe that it is advisable to shield a sample from light after the blood draw until testing, at least with neonatal specimens, when measuring DB by using the vanadate oxidation method.
Conclusions
Under ambient white LED light, specimens with UCB concentrations of approximately 10 mg/dL generated and accumulated approximately 1.3 mg/dL of BSI in 1 h. In addition, approximately 34% of the BSI concentration affected the measurements of DB when using the vanadate oxidation method.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by KAKENHI (19K08349) and Health Labor Sciences Research Grant (21FC1001).
Ethical approval
The study was approved by the institutional ethics committee (Kagawa University Heisei 30-188).
Guarantor
Takashi Kusaka.
Contributorship
MA, KK, HO, SI, and TK researched literature and conceived the study, and was involved in protocol development. MA, YN, and SN collected samples. MA, KK, MO, and HK measured bilirubin fractions. MA and KK wrote the first draft of the manuscript. KK, KM, HO, SI, and TK obtained ethical approval. All authors reviewed and edited the manuscript and approved the final manuscript.