
Abstract
Background
An accurate estimation of the duration of atrial fibrillation is critical for its safe management. Recent studies suggested that copeptin, carbohydrate antigen-125, galectin-3 and growth differentiation factor-15 are increased in atrial fibrillation. We examined the ability of these markers to identify patients presenting with atrial fibrillation of ≤48 versus >48 h duration.
Methods
Retrospective analysis of a prospective study that included patients with atrial fibrillation of known duration.
Results
A total of 98 patients were analysed, 47 with atrial fibrillation ≤48 h and 51 with >48 h. In patients presenting with atrial fibrillation of ≤48 versus >48 h duration, the mean carbohydrate antigen-125 concentration was 16.9 ± 12.5 versus 30.9 ± 36.3 U/mL (P = 0.01), and growth differentiation factor-15 concentration was 1320 ± 889 versus 2608 ±2163 pg/mL (P < 0.001). Copeptin concentration was not independently associated with atrial fibrillation duration. The galectin-3 concentration did not differ between groups. Area under the ROC curve to identify patients with atrial fibrillation ≤48 h was 0.869 for carbohydrate antigen-125, 0.853 for growth differentiation factor-15.
Conclusion
The plasma concentrations of carbohydrate antigen-125, growth differentiation factor-15 and copeptin, but not galectin-3, are higher in patients presenting with atrial fibrillation of >48 h duration than in those with atrial fibrillation ≤48 h. The ability to discriminate recent atrial fibrillation offered by carbohydrate antigen-125 and growth differentiation factor-15 seems high.
Introduction
Atrial fibrillation (AF) affects approximately 3% of the adult population, is associated with a near-doubling mortality rate and is responsible of 20–30% of all strokes.1–3 Guidelines published in the early 2000s suggested that a cardioversion could be performed safely in AF < 48h without anticoagulation. 4 Later, some studies reported an increase risk of stroke after cardioversion that correlates with AF duration. 5 As a consequence, the latest guidelines still suggest that a cardioversion is possible in AF ≤48 h without prior transoesophageal echocardiography (TEE) or three-week oral anticoagulation, but recommend the initiation of precardioversion anticoagulant.1,6 The precise determination of AF duration therefore appears to be crucial.
We and others have reported that A and B-type natriuretic peptides concentrations were increased in the presence of AF7–10 and could estimate the duration of AF.9,11,12 Some recent studies also suggest that other biomarkers may increase in patients with AF. Thus, copeptin and galectin-3, which are mainly known as important prognostic factors in heart failure and/or coronary artery disease, are increased in AF.13,14 Ding et al. reported the existence of a gradual increase in N-terminal pro-brain natriuretic peptide (NT-proBNP), copeptin and carbohydrate antigen-125 (CA-125) in patients with AF, heart failure and both diseases. 14 Growth differentiation factor-15 (GDF-15) concentration is also increased in AF patients versus age–sex-matched controls, in AF patients with versus without left atrial appendage (LAA) thrombus and is associated with increased mortality in AF.15–17
These biomarkers are involved in inflammation and fibrosis,18,19 and we hypothesized that their concentration may differ according to the duration of AF.
Methods
This is a retrospective analysis of a prospective study. 12 Briefly, we included at two sites, between January 2013 and December 2014, patients <85 years with AF of known duration, without recent acute coronary syndrome (ACS), heart failure (HF) or sepsis and without severe renal failure. A special attention was paid to the determination of the exact duration of AF by two cardiologists; it was based on the onset of symptoms reported by the patients, 12-lead and 24-h ambulatory electrocardiograms recorded in the ambulatory and in-hospital settings, the interrogation of pacemakers, the last cardiac rhythm observed.
At admission, patients underwent blood collection in ethyleneaminetetraacetic acid tubes and the plasma was aliquoted and stored at −80°C. A first aliquot was used to measure mid-regional pro-atrial natriuretic peptide (MR-proANP), and the results of MR-proANP and NT-proBNP have been reported. 12 The second aliquot was used to measure copeptin, GDF-15, galectin-3 and CA-125.
The management of the patient was at the discretion of his/her physician and was not influenced by the participation in the study. The study was approved by the ethics committee (Comité de Protection des Personnes Ile de France III, rec number 2013, A00687-38), and all patients granted their informed consent to participate in the study.
Biochemical analysis
Plasmatic concentrations of galectin-3 were measured using the enzyme-linked fluorescent assay technique on a Vidas analyzer (Biomerieux, Lyon, France). The measured range is from 3.3 to 100 ng/mL, and the inter-assay coefficient of variation at 38.7 ng/mL is <5% in our laboratory.
Plasmatic concentrations of GDF-15 and CA-125 were measured using a sandwich immunoassay on a Cobas E801 analyzer (Roche Diagnostics, Meylan, France). For GDF-15, the measured range is from 400 to 20,000 pg/mL and the inter-assay coefficients of variation at 1400 and 7300 pg/mL are <2% in our laboratory. For CA-125, the measured range is from 0.6 to 5000 U/mL and the inter-assay coefficients of variation at 14.8, 35.9 and 101 U/mL are <3.5% in our laboratory.
Plasmatic concentrations of copeptin were measured using the immunoluminometric assay on a Kryptor analyzer (B.R.A.H.M.S, ThermoFisher Scientific, Hennigsdorf, Germany). The measuring range is from 4.8 to 500 pmol/L and the inter-assay coefficients of variation at 5.2 and 97.1 pmol/L are <5% in our laboratory.
Statistical analysis
Variables are expressed as means ± standard deviations, medians (interquartile ranges) or counts and percentages as appropriate. Continuous variables were compared using Student’s t-test. Qualitative data were compared using the chi-square or Fisher’s exact test. Correlations between biomarkers and the CHA2DS2-VASc score were examined using Spearman’s test.
The ability of the measured biomarkers to discriminate AF ≤ 48 h versus >48 h was examined first using single variable regression models, then multiple variable logistic regression. Based on our previous results that showed that heart rate, the presence of dyspnoea and MR-proANP were the best parameters to differentiate the two groups, we included heart rate and dyspnoea in the analysis. As renal function may affect the concentration of several biomarkers, we added creatine concentration in a second model. Receiver operator characteristic (ROC) curves were constructed to examine and compare the performances of the measured markers. The statistical analyses were performed using the R (R Foundation for Statistical Computing, version 3.1.1, Vienna, Austria) software. A P value < 0.05 was considered statistically significant.
Results
From the 106 patients included in the study, the stored plasma was damaged in eight (7.5%); results are therefore presented for 98 patients. AF was ≤48 h in 47 patients and >48 h in 51. Table 1 summarized the main characteristics of the patients. Compared with AF > 48 h, patients with AF ≤ 48 h were younger, had a higher heart rate, fewer had history of AF, had more palpitation and less dyspnoea at admission.
Main baseline characteristics.
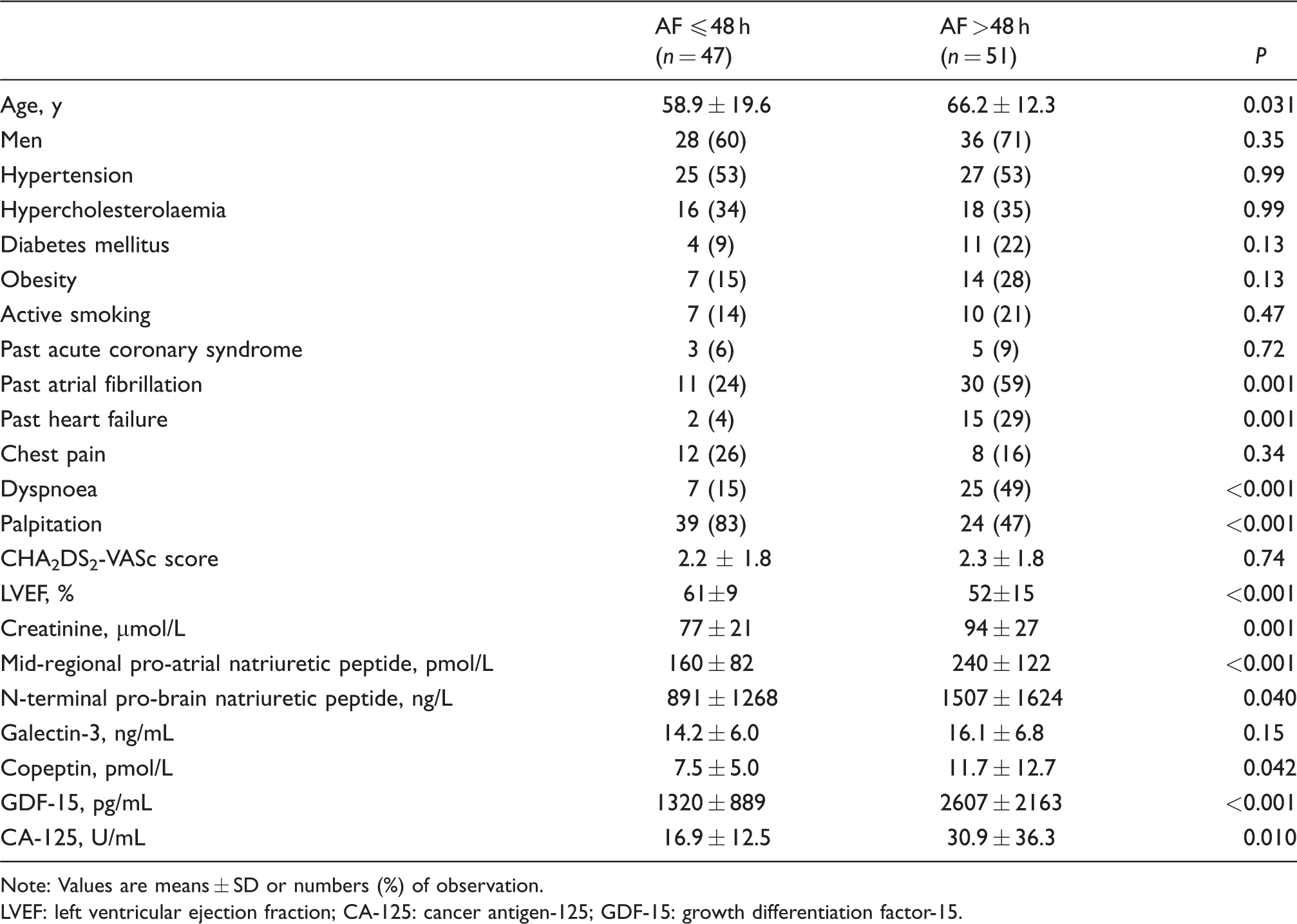
Note: Values are means ± SD or numbers (%) of observation.
LVEF: left ventricular ejection fraction; CA-125: cancer antigen-125; GDF-15: growth differentiation factor-15.
The plasma concentrations of GDF-15, MR-proANP, NT-proBNP, galectin-3, CA-125, but not copeptin correlated with the CHA2DS2-VASc score, with Spearman's rank correlation coefficients of 0.52 (P < 0.001), 0.49 (P < 0.001), 0.39 (P < 0.001), 0.36 (P = 0.002), 0.34 (P = 0.002) and 0.008 (P = ns), respectively.
Copeptin concentration ranged from 1.6 to 62.9 pmol/L and was below the 12 pmol/L cut-off value in 74 (76%) patients; copeptin concentration was higher in patients with AF > 48 h versus patients with AF ≤ 48 h (P = 0.042) (Table 1). In multivariable analysis, copeptin was not significantly associated with AF ≤ 48 h.
Galectin-3 ranged from 4.6 to 81.7 ng/mL and did not differ between patients with AF ≤ 48h versus AF > 48 h (P = 0.15).
Compared with AF > 48 h, patients with AF ≤ 48 h had lower GDF-15 concentration (2608 ± 2163 versus 1320 ± 889 pg/mL, respectively, P < 0.001) and CA-125 concentration (30.9 ± 36.3 versus 16.9 ± 12.5 U/mL, respectively, P = 0.01).
By multiple variable analysis, GDF-15 and CA-125 were correlated with AF duration ≤48 h independently of heart rate and dyspnoea (Table 2).
Associated factors with AF ≤ 48 h by multivariable analysis.
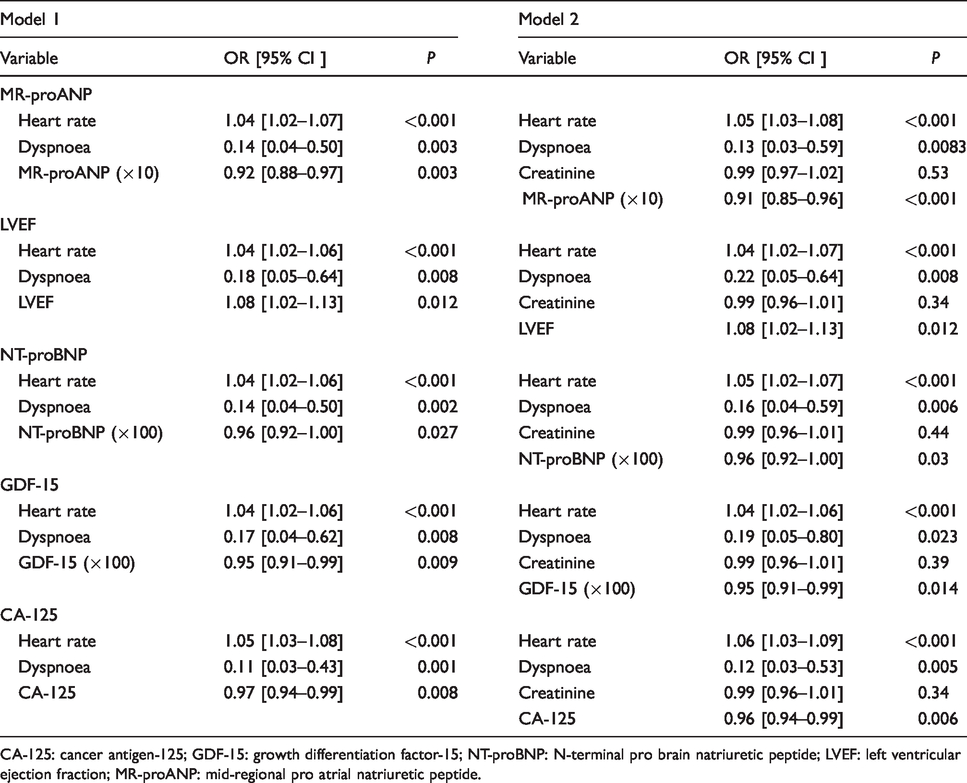
CA-125: cancer antigen-125; GDF-15: growth differentiation factor-15; NT-proBNP: N-terminal pro brain natriuretic peptide; LVEF: left ventricular ejection fraction; MR-proANP: mid-regional pro atrial natriuretic peptide.
Area under the ROC curve to identify patients with AF ≤ 48 h was 0.853 for GDF-15, 0.869 for CA-125, 0.868 for MR-proANP and 0.851 for NT-proBNP (P = NS for all comparisons) (Figure 1).
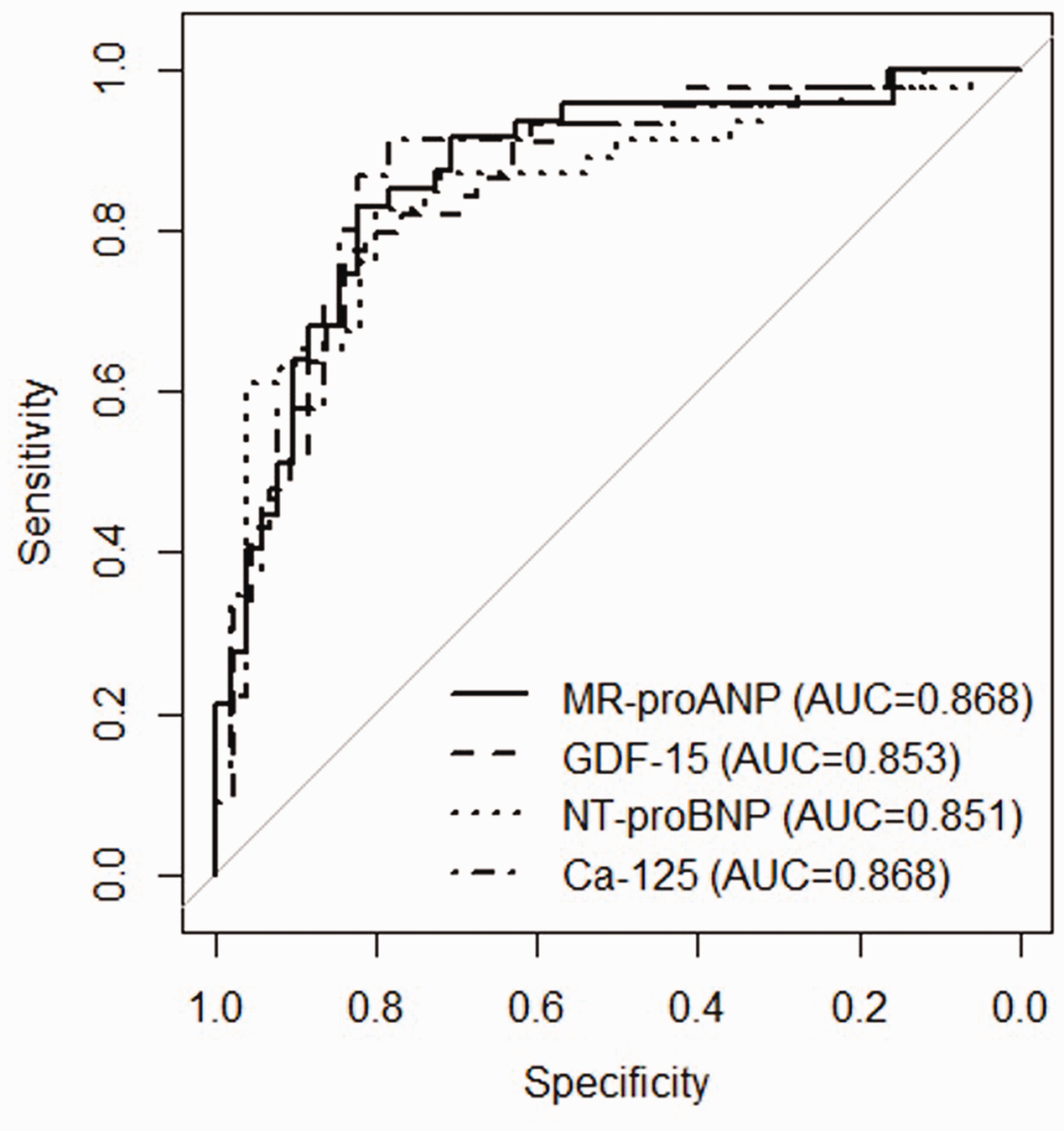
ROC curve for (a) CA-125, (b) GDF-15, (c) NT-proBNP and (d) MR-proANP for the prediction of AF of recent onset.
Discussion
Our study showed that the plasma concentrations of copeptin, GDF-15, CA-125 but not galectin-3 are higher in patients presenting with AF of >48 h duration than in patients presenting with AF that had lasted ≤48 h. The plasma concentrations of GDF-15 and CA-125 were correlated with the CHA2DS2-VASc score. The association between GDF-15, CA-125 and AF duration was independent of heart rate, dyspnoea and renal function. The accuracy of these markers to identify AF of ≤48 h duration was similar to the one observed with MR-proANP or NT-proBNP.
Galectin-3 is a β-galactoside-binding lectin involved in adhesion, inflammation, immunity and fibrosis. It has been well studied as a marker of present and incident heart failure. 20 In the ARIC study, elevated concentration of galectin-3 was associated with an increased risk of incident AF, but this association was mitigated when HF and coronary artery disease (CAD) were entered as variables in the statistical model; this suggests that galectin-3 has a role in the promotion of AF via HF/CAD or involved similar pathways. 13 Very recently, Tang et al. reported a gradual increase in galectin-3 in permanent versus persistent and versus paroxysmal AF as well as an association with the presence of a LAA thrombus. 21 The optimal cut-off value was 18.95 ng/mL. In our study, we report a non-significant difference between AF ≤48 h versus >48 h, and a lower concentration in galectin-3 than the one they observed; this may be explained by a lesser LA and LAA remodelling and is consistent with the lower LA volume observed in our population (data not shown).
Copeptin is the C-terminal fragment of pro-vasopressin and has been studied in numerous cardiovascular diseases including acute myocardial infarction and HF.22,23 The possible role of copeptin as a marker of AF has not been extensively studied and results are somewhat discordant. In one study of patients with transient ischaemic attack, no association existed between the concentration of copeptin and AF but only 18 patients had onset of AF. 24 In another study, copeptin concentration was increased in patients with AF and inversely correlated with left ventricular ejection fraction (LVEF). 14 Our results are consistent with this latter study as we observed an association between AF duration and the concentration of copeptin in single variable analysis, but not in multiple regression that included dyspnoea.
CA-125 and GDF-15 are non-specific biomarkers. To our knowledge, both have seldom been studied in AF and no study investigated their association with AF duration. Thus, GDF-15 concentration was higher in patients with paroxysmal AF versus in patients in sinus rhythm and was associated with the presence of a LA/LAA thrombus according to two studies.15,16 CA-125 concentration was also higher in patients with AF than in those in sinus rhythm according to a recent meta-analysis; however, there was a high heterogeneity among the studies included in the analysis, suggesting some uncertainty in the conclusion. 25 In our study, we show that both GDF-15 and CA-125 can discriminate patients with AF≤ 48 h from those with more prolonged FA. The exact mechanism of the increased of CA-125 and GDF-15 cannot be derived from our study. GDF-15 is a stress-responsive member of the transforming growth factor-β superfamily that may increase following myocardial stretch, volume overload, oxidative stress or inflammation. 18 CA-125 is synthetized by the coelomic cells from the pericardium, pleura and other tissues, following mechanical stress and inflammation. 19 In our study, we excluded patients with recent onset of HF and/or ACS, two conditions associated with increased CA-125 and GDF-15.26–28 In addition, we observed a correlation between the two markers and the CHA2DS2-VASc score. Overall, we may hypothesize that inflammation and/or cardiac wall stretch may contribute to the observe increase in GFD-15 and CA-125, but this hypothesis warrants confirmation.
We and others have previously examined the ability of natriuretic peptides to estimate the duration of AF.10,12 In the present study, we observe a high predictive value of GDF-15 and CA-125 to detect recent AF with AUC > 0.85, but this was not superior to the one of NT-proBNP or MR-proANP. Further studies of the predictive value of these biomarkers, alone or in combination, to identify patients with recent-onset of AF and no LA/LAA thrombus are warranted.
Limitations of our study
The main limitations of our study include its small sample size and its retrospective design.
Conclusion
The plasma concentrations of CA-125, GDF-15 and copeptin are higher in patients presenting with AF of > 48 h duration than in those with AF ≤ 48h. The ability to discriminate recent AF offered by CA-125 and GDF-15 seems high. A prospective external validation in a larger sample is needed to confirm these results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of ‘Paris Ile de France 3’ approved this study (Rec number: 2013-A00687-38).
Guarantor
CM.
Contributorship
CA-B and DL: researched literature and wrote the first draft. CC-G: blood analysis and data analysis. DL, SM, VR, TB and F-XG: patient recruitment, data analysis. MB: statistical analysis. FB: data analysis and revised the article. CM conceived the study, gained ethical approval, data analysis and revised the article. All authors reviewed and edited the article and approved the final version of the article.