
Abstract
Background
Monocyte distribution width has been recently proposed as a sepsis biomarker in the emergency department. The aim of this study was to assess the role of monocyte distribution width as a diagnostic biomarker of sepsis in the intensive care unit.
Methods
In this prospective observational study, we included all consecutive patients admitted to the intensive care unit of the University Hospital “P. Giaccone” of Palermo. Patients were classified into three groups according to Sepsis-3 criteria: (1) patients without sepsis; (2) patients developing sepsis during their hospital stay; (3) patients admitted with sepsis. Monocyte distribution width was measured at admission (groups 1, 2, 3) and daily until the developing of sepsis (group 2) or the end of hospitalization (group 1).
Results
Monocyte distribution width was significantly higher in group 3 than group 1 and group 2 (30.9 [25.6–36.0] vs. 20.3 [18.3–23.6] and 21.4 [19.4–25.2]). Among patients belonging to group 2, monocyte distribution width values, measured at the day when sepsis was clinically diagnosed, were significantly higher than those found at admission: 29.4 (26.7–36.0) vs. 21.4 (19.4–25.2), P = 0.001.
Conclusion
Monocyte distribution width could represent a reliable biomarker of sepsis in the intensive care unit.
Introduction
Sepsis is a leading cause of hospital mortality worldwide, especially in the intensive care unit (ICU). In the last decades, the potential role of several molecules as biomarkers of sepsis has been assessed.1,2 Among these, monocytes have gained attention. At a very early stage of sepsis, monocytes undergo morphological and functional changes resulting in a very heterogeneous population. Monocyte morphological variability can be detected by the monocyte distribution width (MDW), a measure of the dispersion around the mean of the monocyte volume population. Recently, MDW, CE IVD marked and FDA approved, has been proposed as an early indicator of sepsis in the emergency department (ED).3–5 Since MDW has the advantage of being easily measured as part of the complete blood count (CBC), it could represent a practical tool for supporting the diagnosis of sepsis in ICU.
The aim of this study was to assess the role of MDW as a biomarker of sepsis in ICU.
Material and methods
Study design
This observational prospective, monocentric cohort study was performed at the University Hospital “P. Giaccone” of Palermo, Italy.
Eligible patients were all consecutive adult patients (≥18 years of age) admitted to the ICU from September 2019 to March 2020.
Exclusion criteria were (i) age < 18 years; (ii) incomplete data collection; (iii) failure to determine the MDW parameter; (iv) underlying conditions potentially associated with deregulation of the immune system, including AIDS, organ or bone marrow transplantation and haematologic diseases.
All patients were classified into three groups based on the Sepsis-3 consensus criteria 6 : group 1 included patients admitted to the ICU without a diagnosis of sepsis that did not develop sepsis during their hospital stay; group 2 included patients that developed sepsis during ICU hospitalization; group 3 included patients admitted in ICU with a clinical diagnosis of sepsis. According to Sepsis-3 consensus criteria, sepsis was defined as life-threatening organ dysfunction caused by a deregulated host response to infection. 6 Organ dysfunction was identified as an acute change in total SOFA (Sequential Organ Failure Assessment) score ≥2 points consequent to the infection.
The study was performed in accordance with the principles set out in the Declaration of Helsinki. Informed consent was not required because residual biological material was used for all biochemical analyses, confidentiality was guaranteed and no interventions were performed beyond ordinary good and standard clinical practices.
Biochemical parameters
For each patient, MDW was measured at admission (group 1, group 2 and group 3). Moreover, MDW was measured daily from the hospital admission to the development of sepsis (group 2) or to the end of hospital stay due to discharge or death (group 1). Procalcitonin (PCT) and C-reactive protein (CRP) were routinely measured each day of hospital stay.
MDW was measured on blood samples collected in the EDTA-K3 tube by a UniCel DxH 900 hematology analyzer (Beckman Coulter, Inc.) within 2 h of collection, as recommended by the manufacturer, after the laboratory analysis ordered by clinicians were performed.
CRP and PCT were measured on a fully automated platform (Cobas 8000, Roche Diagnostics).
Statistical analysis
Statistical analyses were performed by SPSS statistical software v.17.0 (SPSS Inc., Chicago, IL, USA). Normality distribution was assessed preliminarily by q–q plot, Kolmogorov–Smirnov and Shapiro–Wilk tests. Quantitative variables were expressed by the median and interquartile range (IQR), while categorical variables were expressed by absolute and relative frequencies. Differences between groups for continuous and categorical variables were estimated respectively by non-parametric Kruskal-Wallis test (if >2 groups) or Mann–Whitney U-test, with Bonferroni’s correction and Fisher’s Exact test. Differences between MDW values at different time points were estimated by the non-parametric Wilcoxon signed-rank test.
Results
Ninety-six patients were enrolled in this study: group 1 consisted of 50 patients (52%); group 2 consisted of 16 patients (17%): nine patients developed sepsis in the first two days, whereas the remaining seven patients within the next 10 days; group 3 consisted of 30 patients (31%).
Demographics and biochemical data of the three groups investigated are shown in Table 1. No differences in age, gender or WBC were found between groups. Group 3 displayed significantly higher MDW, PCT and CRP levels than group 1 and group 2 (Bonferroni’s correction, P < 0.001 for all comparisons). Conversely, no significant difference was found between group 1 and group 2 (Bonferroni’s correction, MDW: P = 0.432; PCT: P = 0.225; CRP: P = 0.162) (Table 1). MDW values of group 1 and group 2 are within the reference interval provided by the manufacturer (13.98–21.28). Interestingly, among patients belonging to group 2 (n = 16), MDW values, measured at the day when sepsis was clinically diagnosed, were significantly higher than those found at admission: 29.4 (26.7–36.0) vs. 21.4 (19.4–25.2), P = 0.001. Similarly, MDW values measured at the day of clinical diagnosis of sepsis in patients belonging to group 2 were also significantly higher than baseline MDW levels of patients belonging to group 1: 29.4 (26.7–36.0) vs. (20.3 (18.3–23.6), P < 0.001. However, among patients of group 2, no increasing linear trend of MDW was found in the days before sepsis was diagnosed. Moreover, no significant differences were observed between the baseline and the values of MDW measured in the days before the development of sepsis.
Demographics and biochemical data.
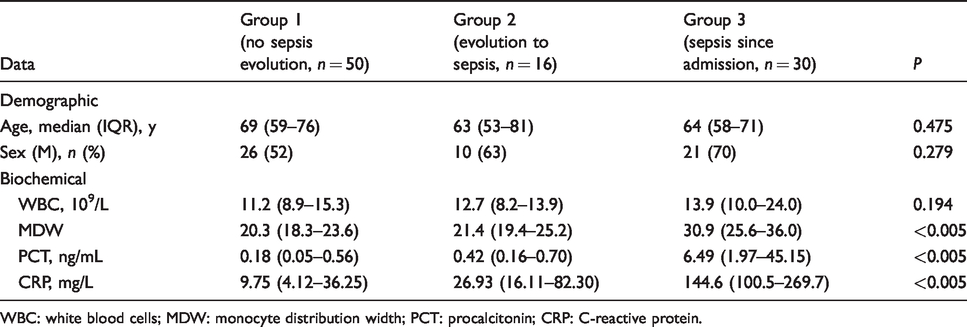
WBC: white blood cells; MDW: monocyte distribution width; PCT: procalcitonin; CRP: C-reactive protein.
Discussion
In this study, we assessed the usefulness of MDW as a diagnostic biomarker of sepsis in ICU. The main findings of our study can be summarized as follows: (i) at admission, patients with sepsis had significantly higher levels of MDW than both patients without sepsis and patients who developed sepsis during their hospital stay; (ii) patients developing sepsis during their hospital stay showed an increase in MDW levels when they developed sepsis in comparison with MDW levels at admission. Overall, our findings support the use of MDW as a biomarker of sepsis in ICU.
To the best of our knowledge, this is the first study evaluating the role of MDW in an ICU setting.
MDW can be measured automatically, routinely, within a few minutes, requiring neither additional sampling nor additional cost to that of CBC, thus making it a very promising biomarker of sepsis.
Some limitations of this pilot study need to be acknowledged. First of all, the small sample size. Moreover, the sample was very heterogeneous because patients developed sepsis in different days. However, this study was performed in a real-practice clinical setting.
Conclusion
MDW could represent a diagnostic biomarker of sepsis in patients hospitalized in ICU. These results are particularly interesting because MDW could be easily available in routine blood counts. Thus, although MDW did not increase in the days before sepsis was diagnosed, it could represent an easy to perform and reliable tool for supporting the diagnosis of sepsis in ICU. However, larger studies are recommended before introducing MDW in ICU clinical practice.
Footnotes
Acknowledgements
We would like to thank Danila Crobu, PhD (Beckman Coulter) for product scientific support and laboratory technicians of the Department of Laboratory Medicine, University Hospital “P. Giaccone”, for their technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Ethics Committee of the University Hospital of Palermo approved this study (REC number: 07/2019)
Guarantor
MC.
Contributorship
LA and MC researched literature and conceived the study. LA, BLS, RVG, GB, CMG, AC were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. MV performed statistical analysis. LA and AMC wrote the first draft of the article. MC made critical revision of the article. All authors reviewed and edited the article and approved the final version of the article.