
Abstract
Background
Our study aims to explore the effect of serum long non-coding RNA (lncRNA) H19 level on the long-term prognosis of endoscopic keyhole surgery or craniotomy for glioma.
Methods
A total of 264 glioma patients were selected. Patients were randomly divided into the Craniotomy-high H19 group, the Craniotomy-low H19 group, the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group.
Results
Compared with adjacent tissues (5.19 ± 1.42), H19 level in cancer tissues (7.45 ± 1.60) and serum (6.44 ± 1.57) was significantly increased (P < 0.05). Compared with serum, H19 level in cancer tissues was significantly increased (P < 0.05). Pearson correlation analysis found that the relative expression level of serum H19 in glioma patients was positively correlated with cancer tissues (rPearson = 0.547, P < 0.001), but had no significant correlation with adjacent tissues (rPearson = 0.126, P = 0.207). The expression of H19 in serum was significantly related to WHO grade (rPearson = 0.514, P < 0.001). Compared with the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group, the survival rate of patients in the Craniotomy-high H19 group (χ2 = 17.115 and log-rank P < 0.001; χ2 = 18.406 and log-rank P < 0.001) and the Craniotomy-low H19 group was significantly reduced (χ2 = 15.007 and log-rank P < 0.001; χ2 = 16.121 and log-rank P < 0.001). Cox regression results showed that serum H19 level, craniotomy and WHO grade were risk factors for glioma. When H19 level was lower than 6.28, the 30-month survival rate of patients with the endoscopic keyhole surgery was 100%.
Conclusion
For patients with low H19 level (<5.36), both endoscopic keyhole surgery and craniotomy are available, otherwise, endoscopic keyhole surgery is more recommended.
Introduction
Glioma is the most common primary craniocerebral malignancy caused by glioblastoma of the brain and spinal cord. 1 Its morbidity accounts for about 35.2%–61.0% of intracranial tumours. Glioma is derived from glioblasts and has the characteristics of high morbidity, high recurrence and high mortality. 2 It can occur in any part of the central nervous system. At present, surgical treatment is the preferred method. Surgery can not only provide the final pathological diagnosis but also remove most of the affected parts. 3 Timely surgical treatment can significantly improve the survival rate and quality of life of patients. However, at the current medical technology, glioma tissue cannot be completely removed by craniotomy. The area of residual tumour cells is large, and the postoperative recurrence rate is high.4,5 In addition, the area of normal brain tissue of exposed patients is more likely to cause irreversible damage to normal brain tissue of patients, which is not conducive to postoperative recovery. 6
With the continuous advancement of medical technology, endoscopic keyhole surgery has become widely used. It can accurately distinguish the diseased part and normal brain tissue under the microscope, and can design a reasonable incision and resection range based on the microscopic observation and imaging diagnosis results. 7 Because normal brain tissue is mostly white under the microscope, and tumour tissue is mostly grey-red or yellow-brown under the microscope, it can clearly distinguish the disease boundary during microsurgery and accurately remove the tumour tissue. 8 Microsurgery can remove the largest diseased area while protecting normal brain tissues, and it can also reduce the area of the incision and reduce iatrogenic vascular injury, which is convenient for postoperative haemostasis and recovery. 7 However, endoscopic keyhole surgery has insufficient surgical incisions, resulting in incomplete visual field and affecting the resection of glioma tissue. 9 Since craniotomy and endoscopic keyhole surgery have their own advantages, finding the useful biomarkers for each method, especially the biomarkers which can be detected by non-invasive methods, will be helpful to guide the choice of surgical methods.
Long non-coding RNA (LncRNA) is a functional transcript consisting of more than 200 nucleotides. 10 LncRNA H19 is one of the most highly conserved transcription products involved in mammalian development. 11 Studies have shown that H19 is a potential oncogenic lncRNA for a variety of cancers, including glioma. 12 Mechanistically, the product of the Myc proto-oncogene c-Myc induces the expression of H19, thereby promoting the formation of glioma. 13 In addition, as a miRNA precursor, H19 can further determine the expression of cancer-associated cadherin-13 by producing miR-675, thereby promoting the growth of glioma. 14 Therefore, we speculated that H19 can be used in the selection of surgical methods (craniotomy/endoscopic keyhole surgery) and prognostic evaluation of glioma. In this study, we assessed the expression patterns of H19 in glioma tissue, para-cancer tissue and serum, and analysed its prognostic evaluation ability for craniotomy/endoscopic keyhole surgery treatments, thus guiding the choice of surgical methods for glioma.
Materials and methods
The number of glioma patients required in this study
The formula for the current study is as follows: n = (μα2/δ) 2 (1–P)P, where α is set to 0.05, μα is set to 1.96, δ is set to 0.10, and the P(Sensitivity) is set to 90%. After substituting μα = 1.96, δ = 0.10, and P(Sensitivity) = 90% into the formula, the number of cases is 133, that is, at least 133 glioma patients are required to obtain reliable statistical results.
Basic information of glioma patients
The ethical approval, the implementation of experimental protocols and subsequent research of this study have been approved by the Clinical Medical Research Ethics Committee of The First Affiliated Hospital of Soochow University (Approval number: 2016012). A total of 279 patients who were suspected of having glioma were chosen in our hospital from February 2016 to June 2017. Among them, 264 cases were confirmed as glioma by pathology. They were divided into craniotomy group and endoscopic keyhole surgery group according to the random number table method, with 132 cases in each group. In the craniotomy group, there were 84 males and 48 females, aged 35 to 50 years, with an average of 43.37 ± 5.31 years. The course of disease was from 0.2 to 13 months, with an average of 5.74 ± 3.21 months. The tumours were located in 36 cases in the frontal lobe, 27 in the thalamus, 17 in the temporal lobe, 19 in the parietal lobe, 15 in the occipital lobe and 18 in the cerebellum. In the craniotomy group, there were 83 males and 49 females, aged 34 to 50 years, with an average of 42.91 ± 5.74 years. The course of disease was 0.3 to 14 months, with an average of 5.38 ± 3.59 months. The tumours were located in 32 cases in the frontal lobe, 28 in the thalamus, 16 in the temporal lobe, 20 in the parietal lobe, 15 in the occipital lobe and 21 in the cerebellum. There was no significant difference in general information between the two groups of patients (P > 0.05).
Inclusion and exclusion criteria for glioma patients
Inclusion criteria: (1) According to the patient's medical history and imaging data, it shows that it meets the diagnostic criteria for gliomas. (2) The course of admission is about five months, and surgery is needed. (3) The patient can perform treatment-related surgery, and the surgery is well tolerated. (4) The patients and their families gave informed consent and volunteered to participate in the research.
Exclusion criteria: (1) People with heart failure and severe arrhythmia. (2) People with severe liver and kidney disease and mental disorders. (3) Patients who are allergic to surgical drugs. (4) The patients have poor tolerance for surgery and cannot follow-up on time. (5) Patients with incomplete information.
Methods of craniotomy and endoscopic keyhole surgery
The craniotomy group was treated with traditional craniotomy, and the endoscopic keyhole surgery group was treated with microsurgery. The craniotomy method is that the patient is given general anaesthesia before surgery, and the craniotomy is performed conventionally. According to the visual observation, the tumour site and the limit of the infiltrated tissue are determined and an appropriate approach is chosen to perform the operation and remove the diseased site. Endoscopic keyhole surgery was performed with 10 mg of dexamethasone and intravenous infusion of 20% mannitol 250 mL 30 min before surgery to reduce oedema and control the infection. After conventional craniotomy, the operation is performed under a microscope, and the surgical incision is designed in accordance with the imaging diagnosis of the patient. The size of the surgical incision can be smoothly implemented without exposing the patient's normal brain tissue and protecting the nervous system. The sulci or fissure approach is chosen, which is closest to the affected area during the operation. During the approach, attention is paid to protecting important functional areas of the brain, and the arachnoid on the surface of the approach sulcus is released and separated. The patient's brain tumour is observed in the microscope, and an entry is made along the oedema zone or glial hyperplasia zone around the tumour, and the tumour is separated. The diseased tumour is removed while protecting the corresponding brain tissue.
Serum and tissue samples collection
A total of 2 mL of peripheral blood was collected from patients with glioma on an empty stomach for 8–10 h before the surgery, and serum was isolated. The cancer and adjacent tissues were collected during the operation. All specimens were stored in liquid nitrogen.
LncRNA H19 detection
This study was conducted in full compliance with the Minimum Information for Publication of Quantitative Real-Time PCR Experiments (MIQE) guidelines 2009 (Supplementary Table 1).
15
Total RNA was extracted according to the RNA extraction kit (QIAGEN, Germany, Lot number: 40281102), and then reverse-transcribed into cDNA by genome-free-reverse transcription kit (Takara, Japan, Lot number: 47001921). Quantitative real-time polymerase chain reaction (qRT-PCR) was performed according to SYBR GREEN instructions (QIAGEN, Germany, Lot number: 40280319). Primer sequences are as follows: H19 forward: 5′-
Observation indicators and postoperative follow-up
The average operation time and average postoperative recovery time of the two groups were recorded and compared. The clinical curative effect of the two groups, the number of adverse reactions during the perioperative period and the death after 30 months of follow-up were also observed and compared. Clinical effects include effective (clinical symptoms disappeared and glioma was completely removed), improved (clinical symptoms improved significantly, compared with previous imaging data, glioma resection was more than 50%) and ineffective (no significant improvement in clinical symptoms, less than 50% of glioma resections compared to previous imaging data). Effectiveness = (valid + improved)/invalid × 100%.
Statistical analysis
Statistical analysis was performed using SPSS 20.0. Comparisons of normal distribution data (mean ± standard deviation [SD]) were performed using t-test. Pearson test was used to calculate the correlation between H19 and clinical features of glioma patients. Receiver operator characteristic curve (ROC) was used to calculate the cut-off value of H19 for predicting the death of patients within 30 months. The Kaplan–Meier method was used to calculate the survival analysis of serum H19 in craniotomy and endoscopic keyhole surgery groups, and the Cox proportional regression model was used to analyse the potential factors affecting the prognosis of glioma patients. The inspection level α in this study was 0.05.
Results
H19 expression levels in serum, cancer and adjacent tissues, and the correlation between patients' tissues and serum H19 levels
In order to analyse the expression level of H19 in glioma patients, we measured the relative expression of H19 in cancer tissues, adjacent tissues and serum of 264 glioma patients. Compared with adjacent tissues (5.19 ± 1.42), the relative expression of H19 in cancer tissues (7.45 ± 1.60) and serum (6.44 ± 1.57) was significantly increased (P < 0.05, Figure 1(a)). Compared with serum, the relative expression of H19 in cancer tissues was significantly increased. Pearson correlation analysis found that the relative expression level of serum H19 in glioma patients was positively correlated with cancer tissues (rPearson = 0.547, P < 0.001, Figure 1(b)) but had no significant correlation with adjacent tissues (rPearson = 0.126, P = 0.207, Figure 1(c)).
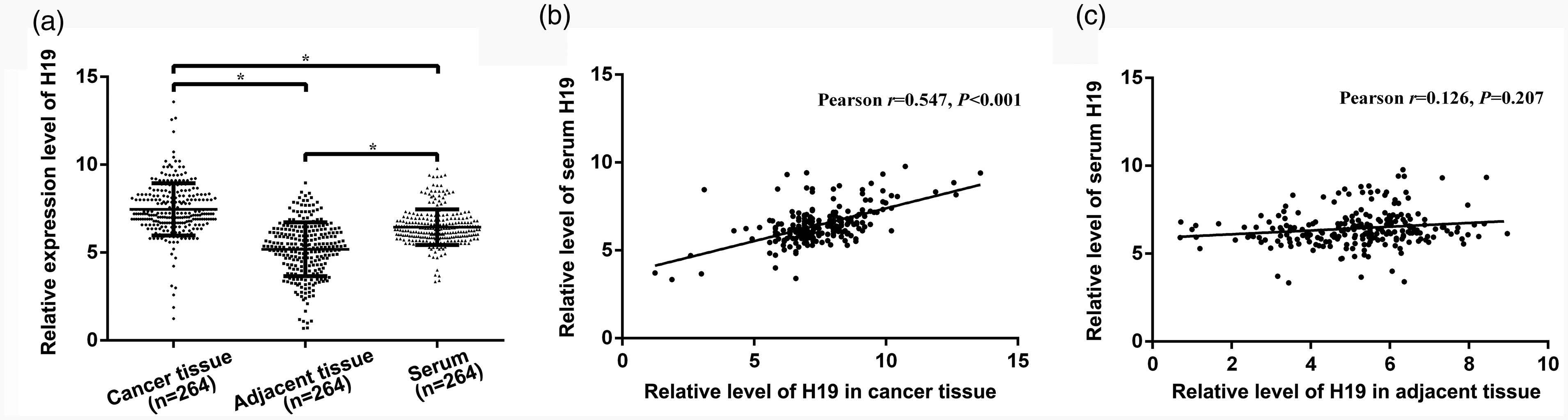
The relative expression level of H19 in serum, cancer and adjacent tissues. (a) H19 expression levels in 264 glioma patients' tissue and serum. (b) The relative expression level of serum H19 in glioma patients was positively correlated with cancer tissues. (c) The relative expression level of serum H19 in glioma patients had no significant correlation with adjacent tissues. *P < 0.05.
Relationship between serum H19 and clinical characteristics of glioma
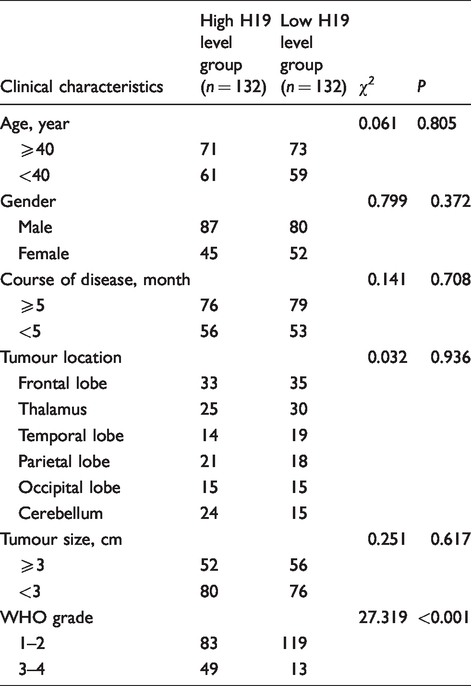
Because the relative expression of H19 in cancer tissue and serum has a significant correlation, in addition, in order to meet the needs of non-invasive detection, we selected the relative expression of H19 in serum for subsequent analysis. In order to further explore the relationship between the relative expression of serum H19 and the clinicopathological characteristics of glioma patients, we collected the patient's age, gender, course of disease, tumour location, tumour size and WHO grade. Our analysis found that the relative expression of H19 in patients' serum was significantly related to WHO grade (rPearson = 0.514, P < 0.001), and the relative expression of H19 in patients with grade 3–4 (7.13 ± 1.55) was significantly higher than that in patients with grade 1–2 (6.23 ± 1.52, P < 0.05, Table 1). However, the relative expression of serum H19 has no significant correlation with other basic information (P > 0.05, Table 1).
Relationship between serum H19 and clinical characteristics of glioma patients.
Comparison of the intraoperative parameters, complications and recurrence in the different groups
According to the surgical method and the relative expression of serum H19, 264 patients were divided into the Craniotomy-high H19 group (n = 66), the Craniotomy-low H19 group (n = 66), the Endoscopic keyhole surgery-high H19 group (n = 66) and the Endoscopic keyhole surgery-low H19 group (n = 66). Compared with the Craniotomy-high H19 group and the Craniotomy-low H19 group, the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group had significantly lower average operation time, average recovery time, adverse reaction rate, recurrence and death (P < 0.001, Table 2). There was no significant difference in postoperative efficacy between the four groups (P = 0.531).
Intraoperative parameters, complications and recurrence in the different groups.
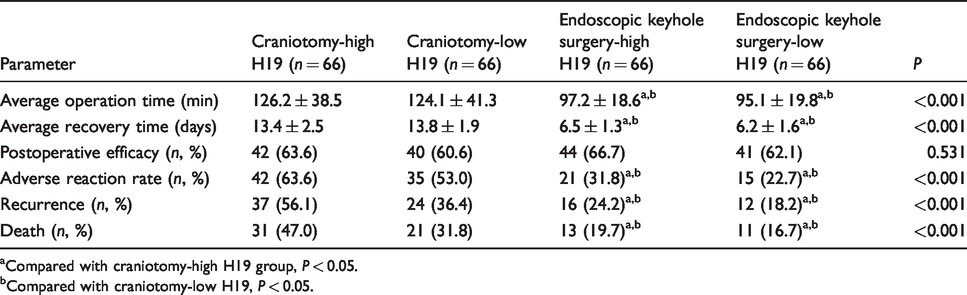
aCompared with craniotomy-high H19 group, P < 0.05.
bCompared with craniotomy-low H19, P < 0.05.
Effect of serum H19 level on the prognosis of patients treated with two surgical methods
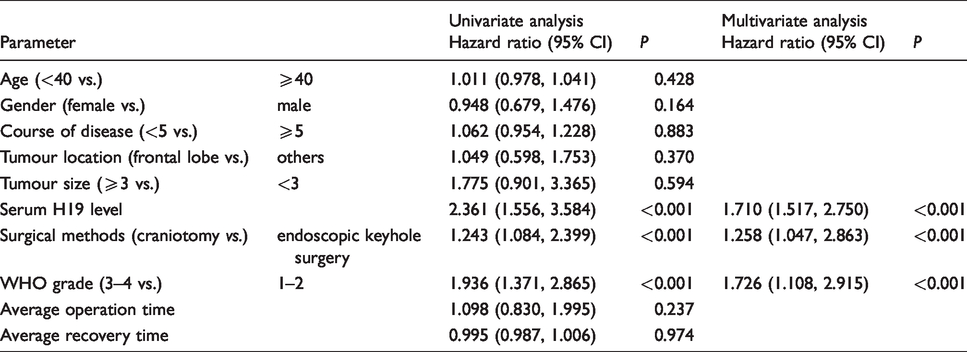
According to the median of H19 expression levels in each group, we further divided patients into the Craniotomy-high H19 group (n = 66), the Craniotomy-low H19 group (n = 66), the Endoscopic keyhole surgery-high H19 group (n = 66) and the Endoscopic keyhole surgery-low H19 group (n = 66). In order to analyse the relationship between the relative expression of serum H19 and the surgical method on the prognosis of glioma patients, a 30-month follow-up was performed, and the patient's survival was recorded. Compared with the Craniotomy group, the survival rate of patients in the Endoscopic keyhole surgery group was significantly improved (χ2 = 14.791 and log-rank P < 0.001, Figure 2(a)). Compared with the Craniotomy-high H19 group and the Craniotomy-low H19 group, the survival rate of patients in the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group was significantly improved (χ2 = 20.528 and log-rank P < 0.001, Figure 2(b)). And compared with the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group, the survival rate of patients in the Craniotomy-high H19 group (χ2 = 17.115 and log-rank P < 0.001; χ2 = 18.406 and log-rank P < 0.001, Figure 2(b)) and the Craniotomy-low H19 group was significantly reduced (χ2 = 15.007 and log-rank P < 0.001; χ2 = 16.121 and log-rank P < 0.001, Figure 2(b)). The Cox regression results are shown in Table 3. The relative expression levels of serum H19, craniotomy and WHO grade were risk factors affecting the prognosis of glioma patients.
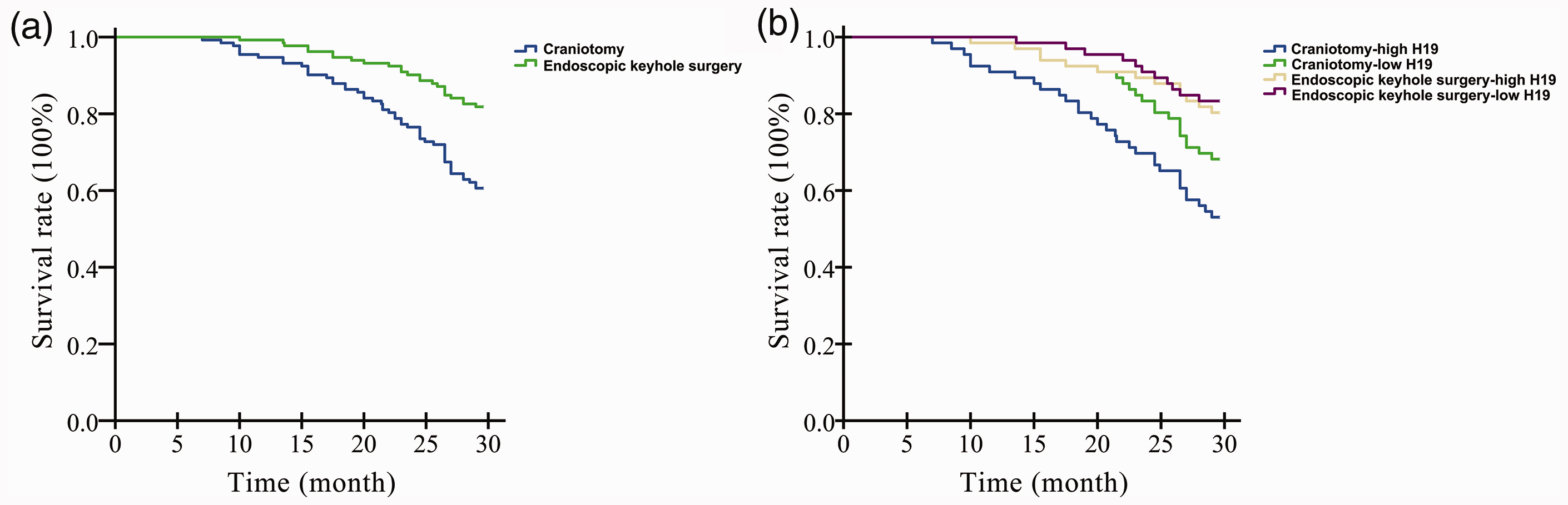
The relative expression level of H19 in serum affects the long-term prognosis of glioma patients. (a) Compared with the craniotomy group, the survival rate of patients in the endoscopic keyhole surgery group was significantly improved. (b) Compared with the Craniotomy-high H19 group and the Craniotomy-low H19 group, the survival rate of patients in the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group was significantly improved.
Proportional hazards model analyses for glioma.
In order to further determine the value of the relative expression of serum H19 in the choice of surgical method, we performed ROC curve analysis. The results showed that when the relative expression level of serum H19 in glioma patients was lower than 5.36, the survival rate at 30 months after craniotomy was 100% (Figure 3(a)). When the relative expression of serum H19 in glioma patients was lower than 6.28, the 30-month survival rate of patients with the endoscopic keyhole surgery was 100% (Figure 3(b)). When the relative expression of H19 in glioma patients was higher than 6.28, the endoscopic keyhole surgery was better.
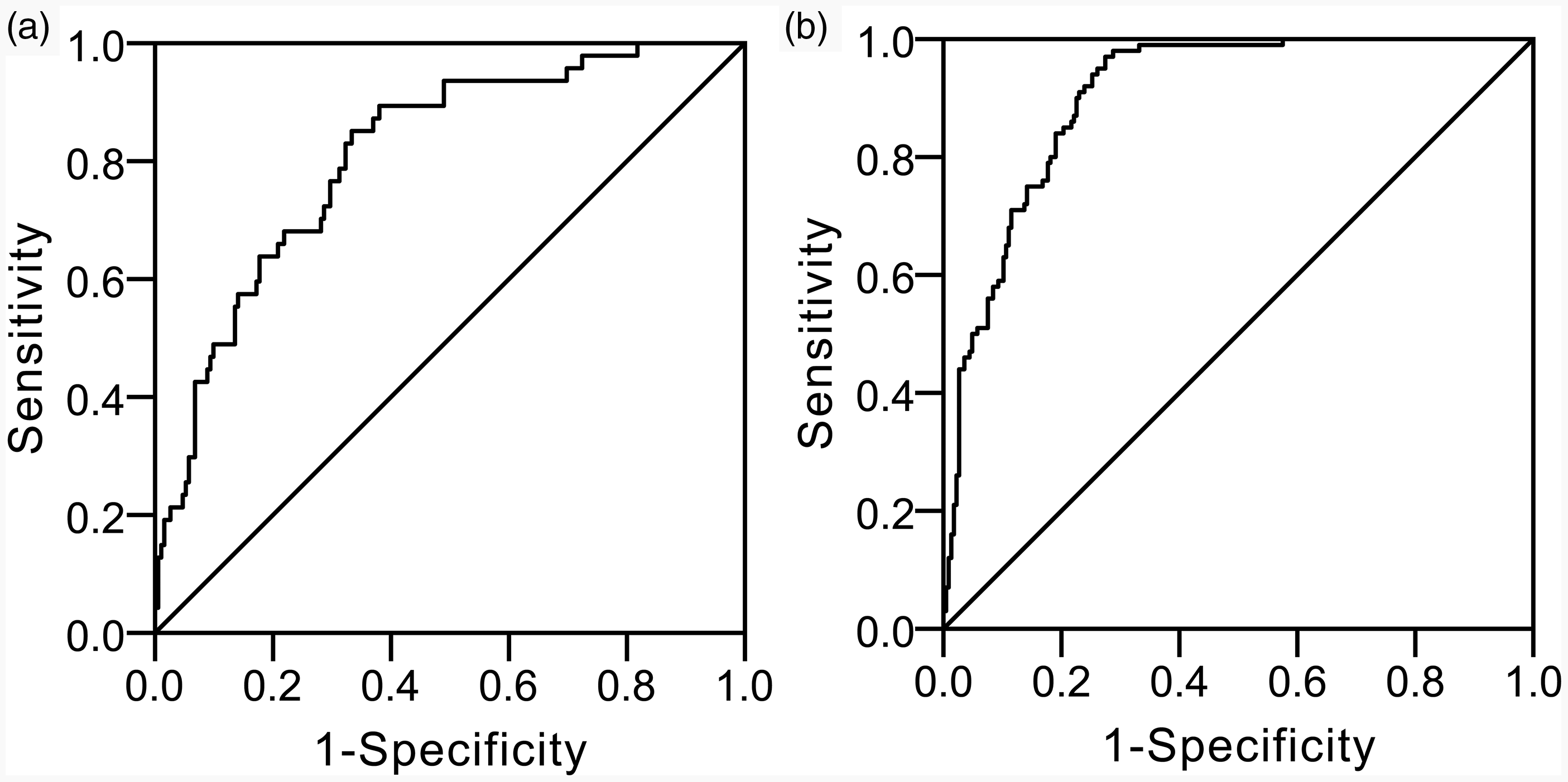
Receiver operating characteristic (ROC) curve analysis. (a) Craniotomy group. (b) Endoscopic keyhole surgery group.
Discussion
Glioma is a disease with a high incidence of brain tumours. Its incidence is about 40.49%, and the age of onset is mainly in the 30–40 years. 16 Glioma is a primary craniocerebral tumour, which is the most common pathological change after the brain and spinal glia become cancerous. It is often caused by the interaction of congenital high-risk factors and alleviating carcinogenic factors, and its incidence is increasing year by year. 17 Glioma can occur in any part of the central nervous system, and the boundaries of the disease are not clear. 2 Clinically, it is mainly treated by surgery, radiotherapy, chemotherapy, targeted therapy and other methods, but the effect is not obvious and it is easy to relapse. 6 With the continuous development of the medical field, the level of microsurgery has been continuously improved, the application in brain tumours has been increasing, and good results have been achieved in surgical resection of brain tumours.
In this study, 264 glioma patients were included and randomly divided into the craniotomy and endoscopic keyhole surgery groups. In addition, we analysed the correlation between the relative expression of serum H19 and the clinicopathological characteristics and prognosis of glioma patients, and initially formulated the cut-off value of serum H19 for the selection of surgical methods. We found that compared with adjacent tissues, the relative expression of H19 in cancer tissues and serum was significantly increased. Pearson correlation analysis found that the relative expression level of serum H19 in glioma patients was positively correlated with cancer tissues, but had no significant correlation with adjacent tissues. We analysed that the relative expression of serum H19 was related to cancer tissues because H19 was released into the blood in cancer tissues. Therefore, serum H19 level can indirectly reflect the level of H19 in cancer tissues and is expected to be used for the evaluation of patients' disease status, non-invasive screening and choice of surgical methods. The results of the correlation analysis further validated our hypothesis; we found that the relative expression of H19 in patients' serum was significantly related to WHO grade, and the relative expression of H19 in patients with grade 3–4 was significantly higher than that in patients with grade 1–2. Currently, the most commonly used classification system for gliomas is the classification system developed by the WHO.18 According to this grading system, gliomas are classified from grade 1 (with the lowest malignancy and the best prognosis) to grade 4 (with the highest malignancy and the worst prognosis). Our results suggest that the relative expression of serum H19 is positively correlated with the severity of the patient's condition and has value for assessing the prognosis of the patient.
It is worth noting that we compared intraoperative parameters, complications and recurrence of patients with craniotomy or Endoscopic keyhole surgery. The results show that compared with the Craniotomy-high H19 group and the Craniotomy-low H19 group, the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group had significantly lower average operation time, average recovery time, adverse reaction rate, recurrence and death. The above results suggest that endoscopic keyhole surgery is more secure. In order to analyse the relationship between the serum H19 and the prognosis of glioma patients, we analysed the patients of the Craniotomy-high H19 group, the Craniotomy-low H19 group, the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group. Compared with the Craniotomy-high H19 group and the Craniotomy-low H19 group, the survival rate of patients in the Endoscopic keyhole surgery-high H19 group and the Endoscopic keyhole surgery-low H19 group was significantly improved. The above results suggest that patients with endoscopic keyhole surgery have a better overall prognosis. Moreover, we also found that when the relative expression level of serum H19 in glioma patients was lower than 5.36, the survival rate at 30 months after craniotomy was 100%. When the relative expression of serum H19 in glioma patients was lower than 6.28, the 30-month survival rate of patients with the endoscopic keyhole surgery was 100%. When the relative expression of H19 in glioma patients was higher than 6.28, the endoscopic keyhole surgery was better. The above results provide a reference value for glioma patients with different serum H19 expression levels when choosing a surgical method.
In conclusion, this is the first study demonstrating the value of serum H19 to predict long-term outcomes of glioma patients who underwent craniotomy or endoscopic keyhole surgery, which may provide us a non-invasive approach to guide the selection of surgical methods for glioma treatment.
Supplemental Material
sj-pdf-1-acb-10.1177_0004563220941888 - Supplemental material for Prognostic evaluation of serum long non-coding RNA H19 for endoscopic keyhole surgery or craniotomy in glioma
Supplemental material, sj-pdf-1-acb-10.1177_0004563220941888 for Prognostic evaluation of serum long non-coding RNA H19 for endoscopic keyhole surgery or craniotomy in glioma by Likui Shen, Min Xu, Zhimin Wang and Zhengquan Yu in Annals of Clinical Biochemistry
Footnotes
Acknowledgements
We would like to thank the Clinical Laboratory of First Affiliated Hospital of Soochow University for the technical guidance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Clinical Medical Research Project of Wuhan health bureau (Approval number: WX12B08).
Ethical approval
This study was approved by the Clinical Medical Research Ethics Committee of The First Affiliated Hospital of Soochow University (Approval number: 2016012).
Guarantor
ZY.
Contributorship
ZW and ZY designed this study. LS and MX performed the experiments. LS, MX and ZW analysed the data. LS and ZY wrote the paper. All authors reviewed and edited the article and approved the final version of the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.