
Abstract
A rare case of cyanoacrylate urine bladder urolithiasis in a 60-year-old male is presented. The application of surgical glue (Glubran) as treatment of seroma one month after laparoscopic inguinal hernioplasty led to the instillation of the n-butyl cyanoacrylate into the bladder resulting in the formation of a concretion. Infrared spectroscopy of the urine stone removed by cystoscopic laser lithotripsy four months after the surgery allowed the identification of the nature of the stone and revealed cyanoacrylate as the major component and co-monomer methacryloxy sulfolane as the minor component. Polypropylene from the mesh was not detected.
Introduction
Urolithiasis is a multifactorial disease resulting from complex interactions between environmental and genetic factors. 1 Risk factors leading to the development of urolithiasis are well known. They include increased content of lithogenic substances (calcium and phosphate ions, oxalates, sodium ions and uric acid), reduced amounts of inhibitory agents (citrates, magnesium ions, Tamm-Horsfall mucoprotein, pyrophosphate), lower intake of fluids, change of urine pH (renal tubular acidosis, bacterial infections), diet (high intake of animal protein, salts, alcohol, sugars and phosphates) and inherited metabolic disorders (metabolic disorders of oxalates, purines, cystine). Conditions such as inflammatory bowel disease, pancreatitis, short gut syndrome and hyperparathyroidism also increase the risk of stone formation due to the associated metabolic abnormalities.1–4
Urocystolithiasis is the presence of calculi or stone-like deposits (concretions) in the urinary bladder. Urocystolithiasis accounts for less than 5% of urinary stones. Elderly men are more prone to urocystolithiasis secondary to intravesical obstruction caused by benign prostatic hyperplasia, neurogenic bladder or urethral stricture. Bladder stones are often seen in patients with augmentation cystoplasty and neobladder construction following radical cystectomy due to chronic exposure to intestinal mucosa. 5
Cyanoacrylate is the generic name of the group of fast-acting adhesives such as ethyl-2-cyanoacrylate, n-butylcyanoacrylate, 2-octylcyanoacrylate sold under various trade names like Histoacryl®, Indermil®, Dermabond®, or Glubran®. Cyanoacrylate is an acrylic resin that polymerizes exothermically in the presence of water, especially with OH– ions, joining the bonded surfaces in 5–6 s and reaching the final stage in 60 s. It binds body tissue excellently and shows bacteriostatic effects. The film of glue is eliminated by hydrolytic breakdown, a process whose duration varies according to tissue type and quantity of glue applied. 6
Case report
We present a rare case of a 60-year-old male with urocystolithiasis of cyanoacrylate origin.
Medical history revealed laparoscopic surgery of bilateral inguinal hernioplasty one month before urinary bladder stone diagnosis. Laboratory tests of relevant serum and urine parameters performed before the surgery showed normal results. One week after hernioplasty, excessive oozing occurred continuously on both sites of the surgical wound and secretion above the mesh occurred, with no mesh erosion. Oozing persisted for one month and aspiration of 150 ml ooze on the left side failed to control it. Surgical glue (1 ml of Glubran) was applied, and its use was documented in medical notes. Next day, symptoms of acute cystitis occurred and patient was admitted at the urology department for presence of dysuria, frequent micturition (10 times per night), haematuria and stranguria. Laboratory investigation of urine chemistry showed signs of inflammation. Cotrimoxazole (2 × 960 mg/day) was prescribed, and follow-up visit after five days was ordered. At the follow-up visit, haematuria was not present any more, but pollakiuria, stranguria and nocturia persisted. Subsequent ultrasonography confirmed bladder cystolithiasis (concretion about 10 × 17 mm). The patient was then indicated to cystoscopy and lithotripsy. Cystoscopy was performed three months later (four months after the hernioplasty). Endoscopic examination demonstrated the presence of irregular solitary concrement 20 mm in diameter, and cystoscopic laser lithotripsy was applied. The stone was crushed by cystoscope and directly collected from the bladder through the cover of the cystoscope. After washing, there was no evidence of residual stone. Removed fragments were collected in the transport tube and on the same day sent to the laboratory for further analysis.
Urine stone analysis
Physical properties of the fragments were of brown smooth surface and a foamy solid white interior. The size of the fragments varied from 5 × 2 × 1, 4 × 2 × 2 mm to fine particles.
Total weight of the all fragments was approximately 0.20 g. All fragments were flexible, plastic and resisted to further crushing (see Figure 1). The fragments were then analysed using infrared (FT-IR) spectroscopy (Nicolet IS10, Thermo Fisher Scientific, USA). The obtained IR spectrum was compared with reference spectra between 4000 and 400 cm−1 from the laboratory spectra reference library.
Fragments of cyanoacrylate urinary stone.
Spectral analysis of the concretion showed the presence of the poly n-butylcyanoacrylate (∼80%). The IR spectrum of the analysed concretion presented peaks matching the reference peaks of functional groups occurring in cyanoacrylate (alkane groups –3000–2840 cm−1, cyanide groups –2250 cm−1, ketone groups – 1750 cm−1, polyalkyl groups –940–500 cm−1). Specific peak in region 1600–1700 cm−1 could refer to the C = C group showing the presence of methacrylate (methacryloxy sulfolane) which is present as an additional co-monomer in Glubran – about 20% (Figure 2).
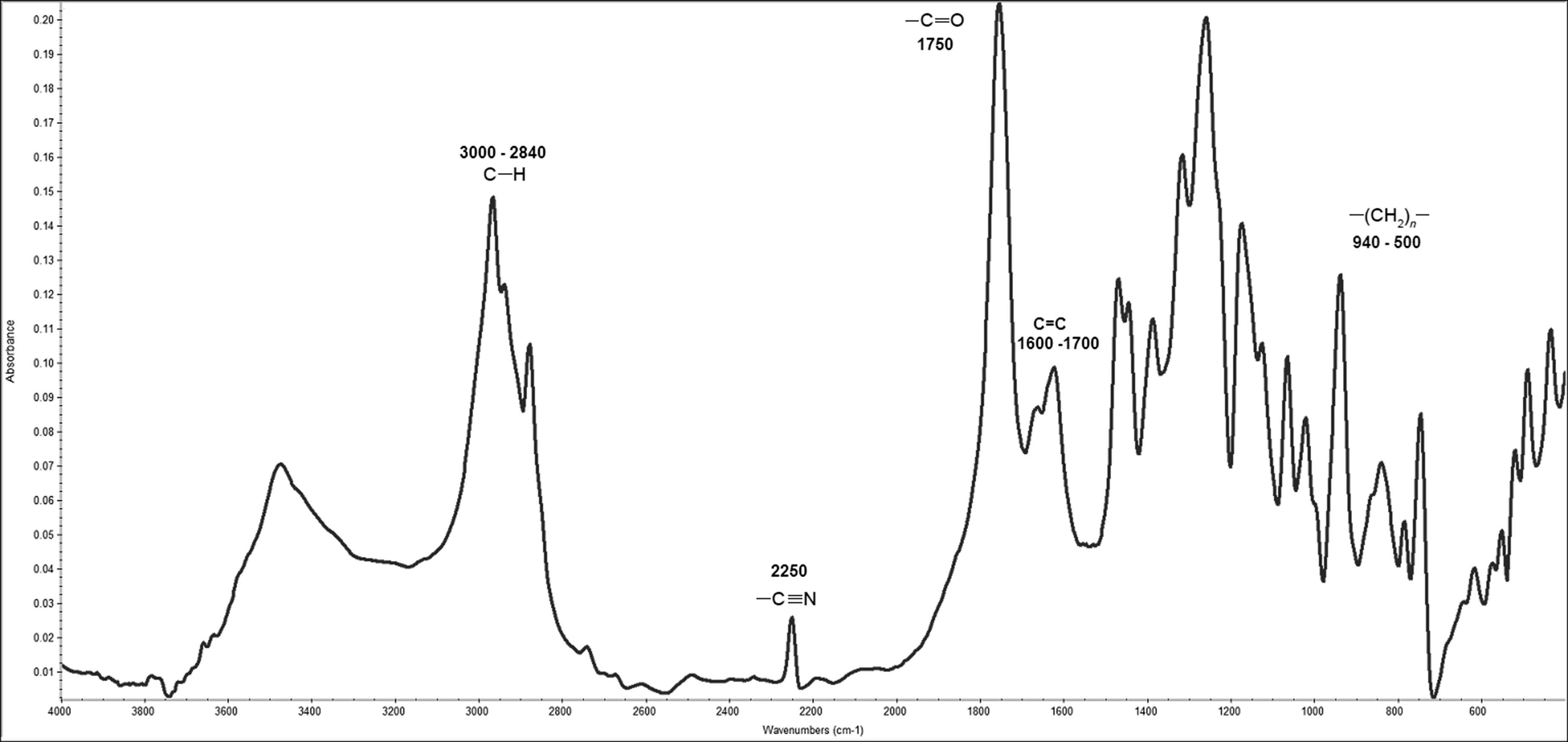
IR spectrum of a concretion containing n-polybutylcyanoacrylate (alkane groups – 3000–2840 cm−1, cyanide groups – 2250 cm−1, ketone groups – 1750 cm−1, polyalkyl groups – 940–500 cm−1, 1600–1700 cm−1 C=C group showing the presence of methacrylate).
Discussion
The patient’s anamnestic data showed that he had been subjected to the laparoscopic hernioplasty four months earlier. The patient said that during the follow-up visit after the hernioplasty, the doctor had applied ‘some kind of glue’ due to persisting wound secretion one month after the hernioplasty. He felt an annoying pain at the site where the glue had been added. It is well known that polymerized synthetic biodegradable cyanoacrylate-based substances attribute high adhesive and haemostatic properties and create an efficient antiseptic barrier against the infective or pathogenic agents during surgical intervention. The use of cyanoacrylate-based glues in laparoscopic hernial surgery is documented and widely used.6–12 The presence of poly n-butylcyanoacrylate as a major component of urine bladder stone in our patient leads to an assumption that poly n-butylcyanoacrylate used in therapy of seroma was released into the bladder and thus became the crucial part of the concretion formation. The mechanism of the cyanoacrylate release into the bladder could be also explained by the mesh erosion caused by secondary migration as a result of erosion of the surrounding tissue,13–15 but this was not the case of our patient. Some recent studies demonstrated cyanoacrylate bladder stone formation following occlusion of vesicosigmoid fistula.16,17 Moreover, we did not detect any polypropylene (mesh) as part of the investigated concretion. The possible mechanism of the stone formation in the presented case could be explained by the fact that during the cyanoacrylate application, instillation of the cyanoacrylate into the bladder through the bladder wall on the left side led to the formation of the concretion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Project (Ministry of Health, Czech Republic) for conceptual development of research organization 00064203 (University Hospital Motol, Prague, Czech Republic).
Ethical approval
Patient has given written informed consent.
Guarantor
KK.
Contributorship
KK performed concretion analysis, prepared the draft of the text, edited the text, researched the literature, MP performed concretion analysis and revised the text, RP collected and prepared clinical data, reviewed and edited the article, AB reviewed and edited the article.