
Abstract
Background
Reflective addition of iron studies to elevated ferritin results can be a useful first step towards making a diagnosis of haemochromatosis; however, the criteria for doing so are poorly defined and the efficiency of different stages of this process are not well documented. We studied the efficiency of current practice at York Teaching Hospitals NHS Foundation Trust with the aim to identify areas for improvement.
Methods
Data were gathered from the laboratory database on the number of iron studies and subsequent interpretive comments reflectively added by laboratory staff during an eight-month period. Reflective addition of iron was based on individual practice of the reporter. Standardised interpretive comments were added to suggest HFE genotyping when both the ferritin and transferrin saturation were raised. The number of patients successfully followed up and found to have pathological HFE gene mutations was used to evaluate efficiency.
Results
A total of 2651 raised ferritin results were reported during the evaluation period, which resulted in the reflective addition of 381 iron studies and 43 interpretive comments by the duty biochemists. This led to 33 requests for HFE genotyping and the identification of 13 individuals with pathological mutations. The number of iron studies reflectively added to diagnose one patient (NND) was found to be 29.3.
Conclusions
Reflective addition of iron studies and interpretive comments can assist in the early detection of patients with hereditary haemochromatosis. Better guidance for laboratory staff undertaking reflective testing and for general practitioners facilitating patient follow-up may increase the efficiency of this diagnostic process.
Introduction
Hereditary haemochromatosis (HH) is a recessive disorder characterised by continuous absorption of iron from the gut despite excessive iron stores. The result of this iron accumulation is systemic tissue damage, including liver cirrhosis and diabetes mellitus. Early detection can prevent organ damage and increase life expectancy. 1
Mutations in the HFE gene account for the majority of HH cases, in particular, homozygosity for the C282Y variant. 2 A second mutation, H63D, is less commonly associated with iron overload, but compound heterozygotes (C282Y/H63D) are still at risk.
The British Society for Haematology have published guidelines for the diagnosis and treatment of HH, which state that Northern European adults with unexplained raised serum ferritin, raised transferrin saturation (TSAT) and normal full blood count results should have molecular testing for HH. 2 Raised ferritin is a frequent incidental finding in primary care, and iron studies should be used to guide genotyping requests in these patients. 2
The addition of further laboratory tests based on initial findings can be categorised as automated reflex testing, or reflective testing by a laboratory professional following review of available results and clinical information. Previous studies have consistently demonstrated greater efficiency for reflective testing than reflex testing; however, criteria for reflective addition of iron studies based on elevated ferritin results are not well defined.
Current practice at York Teaching Hospital NHS Foundation Trust is to reflectively add iron and TSAT to unexplained raised ferritin results and to add standardised interpretive comments to recommend HFE genotyping when appropriate. The aim of this work was to retrospectively evaluate the efficiency of this strategy to aid the diagnosis of HH and identify potential areas for improvement.
Methods
All serum ferritin results above the local reference range (>291 μg/L for females, >322 μg/L for males) were reviewed by a clinical scientist or chemical pathologist during routine clinical validation. Reflective addition of iron studies was based on the individual practice of the reporter. When TSAT was also raised (>50%), standardised interpretive comments were added to recommend HFE genotyping.
Data on the number of iron studies and interpretive comments added, and the number HFE genotyping requests made, were extracted from the laboratory information system for an eight-month period between November 2016 and June 2017. The data were analysed to identify HFE genotyping requests made following reflective addition of iron and interpretive comments by the duty biochemist. Genotyping results were reviewed to identify the number of patients carrying two pathological HFE gene mutations. The number of iron studies added to make a single diagnosis of HH (NND) was used as an indication of the efficiency of the diagnostic strategy.
Results
In the eight-month period, 381 iron studies were reflectively added, generating 50 TSAT results >50%. Interpretive comments suggesting HFE genotyping were added to 43 of these, and 33 patients went on to have genotyping samples collected. Of these 33 genotyping requests, eight were rejected due to normal TSAT on follow-up, one was missed from the request form at request entry in the laboratory and one was not tested due to a pre-existing HFE genotyping result. Of the 23 patients who were tested, 13 were identified as homozygous or compound heterozygous for pathological HFE variants and a further four were found to be heterozygous carriers. The NND for the entire process was 29.3. These findings are summarised in Figure 1.
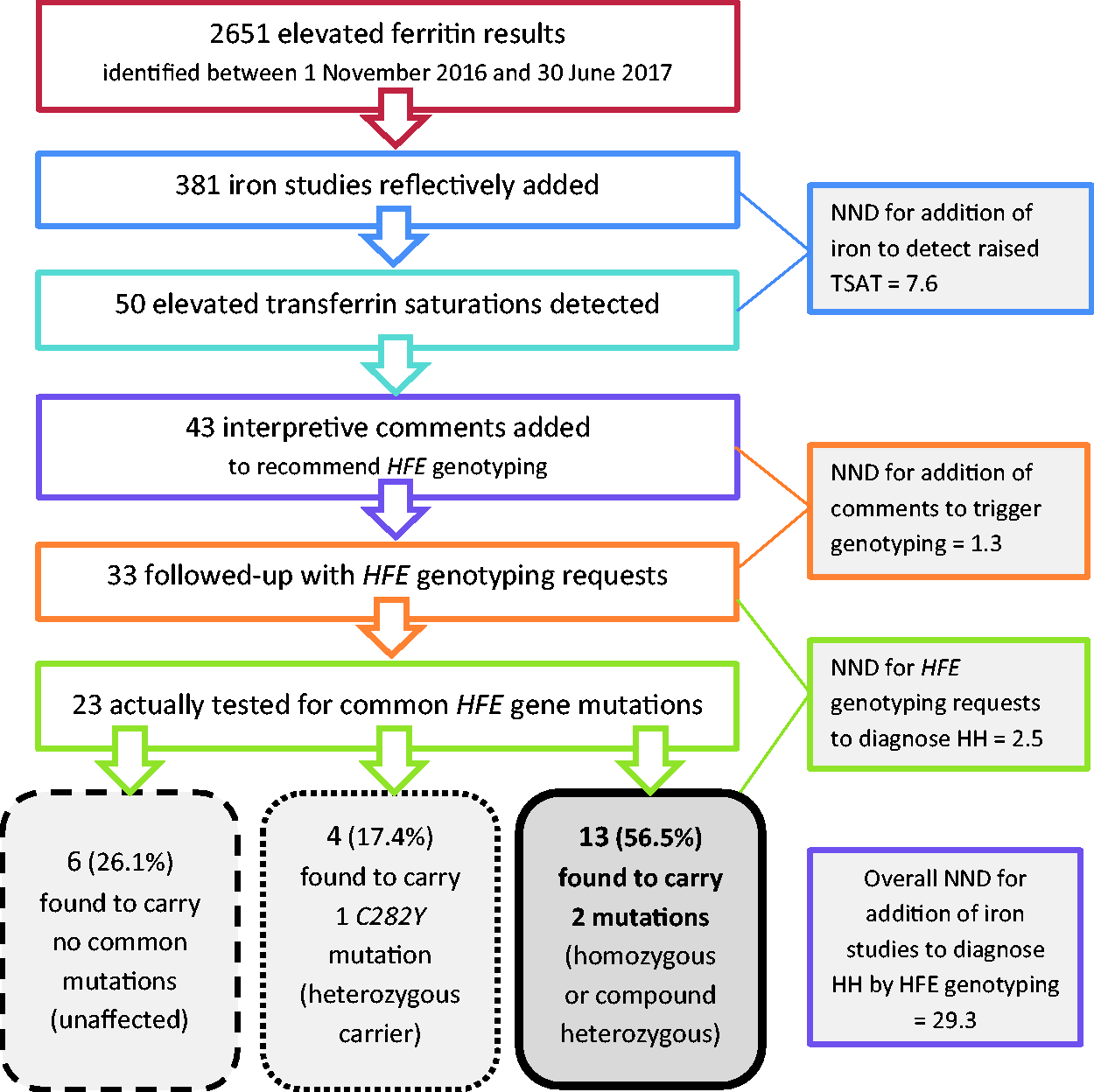
Flowchart to summarize the effectiveness of the reflective testing strategy. The total number of elevated ferritin results excludes requests made from haematology outpatients or renal dialysis units. A total of 10 requests for HFE genotyping were not processed; eight were rejected in light of a normal transferrin saturation result on follow-up, one patient had a pre-existing HFE genotyping result and one request was missed from the request form during request entry.
Discussion
This short retrospective analysis demonstrates the potential value of reflective testing for the early diagnosis of HH. There is further value in identifying heterozygous carriers of the C282Y mutation, as this may have implications for family members. The NND of 29.3 calculated from our data is comparable to published literature; Strivastava et al. 3 reported an NND of 35 when reflectively adding iron studies based on elevated alanine aminotransferase (ALT), and Paterson and Paterson 4 demonstrated an NND of 18.8 when iron studies were reflectively added based on elevated ferritin or ALT, or a combination of both.
In this study, the NND for HFE genotyping was 2.5 when genotyping was suggested. Paterson and Paterson 4 demonstrated an NND of 3.5 for patients with both elevated ferritin and TSAT and Strivastava et al. 3 reported an NND of 7 for patients with raised ALT and TSAT. Our data suggest that reflective testing based on elevated ferritin is more effective than strategies based on ALT, but the study by Paterson and Paterson 4 indicates that the overall NND can be reduced, and therefore efficiency increased, by considering ALT as well as ferritin when adding TSAT.
The number of reflectively added iron studies required to detect a raised TSAT (NND = 7.6) compares with other studies and shows greater efficiency compared to published data on reflex testing using raised ALT.3,4 The efficiency at this step of the process is limited by the multiple aetiologies of elevated ferritin and ALT and the availability of clinical information during clinical validation. Clearer guidance for adding iron studies rather than relying on individual judgement may help to improve efficiency. As a result of this work, we have developed local guidance for staff undertaking reflective testing, to highlight that the addition of iron studies should be considered when the elevated ferritin is new and unexplained, when there is no indication of iron supplementation (e.g. no previous low haemoglobin or ferritin) and particularly where ALT is also elevated.
The current study also found that interpretive comments suggesting HFE genotyping were not added to elevated TSAT results in seven cases, and three comments were added inappropriately because an HFE genotyping result already existed, thereby highlighting room for improvement in the addition of advisory comments.
Of the 50 patients in this study with elevated ferritin and TSAT, only 33 were followed up with HFE genotyping requests by the general practitioner (GP). There may, therefore, be additional patients with unidentified pathological HFE mutations in this study population. This highlights the importance of GP education in improving the overall efficiency of this diagnostic strategy. By increasing genetic testing for HH in primary care, it should be possible to achieve increased early diagnosis while potentially reducing unnecessary referrals to secondary care.
Footnotes
Acknowledgements
The authors thank Maria de Ferrars for her support with preparing the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Both authors are employees of York Teaching Hospital NHS Foundation Trust, where this work was carried out.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
KM.
Contributorship
DT conceived the idea for the study and performed the data extraction from the laboratory information system. KM researched the literature, analysed the data and wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version.