
Abstract
Background
Serum YKL-40 has been proved to be a promising biomarker for estimating the disease activity of several autoimmune diseases. However, its utility in polymyositis or dermatomyositis has not been established. The aim of this study was to investigate the utility of YKL-40 in patients with polymyositis/dermatomyositis.
Method
Patients with definite polymyositis/dermatomyositis who visited the Second People’s Hospital of Wuxi between April 2016 and March 2017 were prospectively enrolled. Eighty-seven healthy individuals were set as a control. Serum YKL-40 of all participants was determined using ELISA. The associations between YKL-40 and clinical characteristics of polymyositis/dermatomyositis were analysed using the Student’s t-test, Mann-Whitney test and receiver operating characteristic curve analysis.
Results
A total of 99 patients with polymyositis/dermatomyositis were enrolled. The patients with polymyositis/dermatomyositis had significantly higher serum YKL-40 concentration. Patients with interstitial lung disease had significantly higher YKL-40 concentration than those without. Serum YKL-40 was positively correlated with myositis disease activity assessment visual analogue scale, C-reactive protein, erythrocyte sedimentation rate and ferritin. The area under receiver operating characteristic curve of YKL-40 for identifying interstitial lung disease was 0.82.
Conclusions
Serum YKL-40 is a useful biomarker for estimating disease activity or severity of polymyositis/dermatomyositis.
Introduction
Polymyositis (PM) and dermatomyositis (DM) are autoimmune diseases primarily affecting skeletal muscles and skin. They are serologically characterized by a high titre of serum autoantibodies and muscle enzymes and histologically by inflammatory infiltrates in skeletal muscle tissue. 1 The inflammatory cells infiltrate in muscle tissue, release cytokines and cytotoxic molecules, leading to muscle damage.2,3 Disease activity estimation and complication prediction are crucial step for PM/DM management, as they can largely affect treatment approach. 4 Interstitial lung disease (ILD) is a common complication in PM/DM patients 5 and associates with poor outcomes. 6 Identification of patients with ILD in PM/DM patients is of great value because it can greatly affect treatment selection and thus has potential to improve the prognosis of patients. High-resolution computed tomography (HRCT) is usually used to identify PM/DM patients with ILD; however, high cost and subjective nature are its two major limitations. To date, some biomarkers have been proved to be associated with disease activity and complication of PM/DM, such as B-cell activating factor, 7 interleukin-35 8 and soluble CD163. 9 However, none of these biomarkers, when used alone, can accurately estimate the disease activity and complication of PM/DM. 10 Therefore, it is of great value to explore novel biomarkers for estimating disease status of PM/DM.
YKL-40, also referred to as human cartilage glycoprotein-39 (HC gp-39), is produced by human chondrocytes, macrophages, neutrophils and synovial cells.11–13 Although the biological function of YKL-40 remains largely unknown, its abnormal expression is associated with several inflammatory-related disorders, 13 such as cardiovascular diseases14,15 and autoimmune diseases. Previous studies indicated that serum YKL-40 is increased and associated with disease activity or severity 16 in several types of autoimmune diseases, including inflammatory bowel disease, 17 systemic lupus erythematosus 18 and rheumatoid arthritis.19,20 However, its utility in PM or DM has been largely unknown. A recently published work demonstrated that serum YKL-40 is increased in PM/DM patients with ILD, 21 and increased YKL-40 is associated with poorer prognosis. However, it remains unknown whether YKL-40 was correlated with disease activity of PM/DM. Therefore, we performed a study to investigate the clinical utility of serum YKL-40 in PM/DM patients.
Materials and methods
Subjects
Patients with definite PM/DM who visited the Second People’s Hospital of Wuxi between April 2016 and March 2017, irrespective of their disease durations, were prospectively enrolled. The diagnoses of PM and DM were based on the criteria established by Bohan and Peter. 22 Patients were excluded if complicated with following disorders: autoimmune diseases other than PD/DM, malignant diseases, end-stage renal disease, infected by hepatitis virus, infection events within four weeks prior admission. Disease activity of PM/DM was estimated using myositis disease activity assessment visual analogue scale (MYOACT). 23 ILD was identified using HRCT.
A total of 99 patients, including 58 PMs and 41 DMs, were included in present study. Eighty-seven individuals who visited hospital for annual healthy checking were enrolled as controls. The results of routine laboratory tests (e.g. blood count and differentiation, glucose, lipid proteins, urine analysis, liver and renal function tests) in controls were generally within reference intervals, and they did not have any complaints when visiting hospital.
This study was approved by the ethic board of the Wuxi Second People’s Hospital. All participants were given informed consent.
YKL-40 and routine laboratory tests
Routine laboratory tests (C-reactive protein [CRP], creatine kinase, lactate dehydrogenase, ferritin and erythrocyte sedimentation rate [ESR]), YKL-40, ILD involvement and MYOACT of all patients were evaluated within 24 h after enrolment.
For YKL-40 determination, 5 mL venous blood sample of each subject was collected in a tube without anticoagulant agent. The blood specimens were centrifuged at 3000 r/min for 15 min to obtain serum. YKL-40 concentration in serum was determined using an ELISA kit (Quidel Co., San Diego, California, United States). The detection limit of this assay was 5.4 ng/mL. The precision CVs within-run was 5.6%–6.6% and between-run was 6%–7%.
Statistical analysis
Normal distribution of continuous variables was tested by the Kolmogorov-Smirnov test. Continuous variables between two groups were compared by the independent Student’s t-test or Mann-Whitney test, if appropriate. Receiver operating characteristic (ROC) curve analysis was used to determine the accuracy of YKL-40 for identifying patients with ILD. Categorical variables were compared using Chi-square test. Correlation between two continuous variables were analysed using the Spearman or Pearson approach, if appropriate. All statistical analyses were performed using SPSS 18.0 (IBM SPSS Statistics, IBM Corporation, Chicago, IL, USA) for Windows and GraphPad Prism 6.0 (GraphPad Software Inc., La Jolla, CA, USA). P-value less than 0.05 was defined as statistical significance.
Results
Summary of subjects
Table 1 lists summary of eligible studies. The median age of subjects was 62 years, and two-thirds of the subjects were females. The median disease duration was eight months.
Summary of eligible studies.
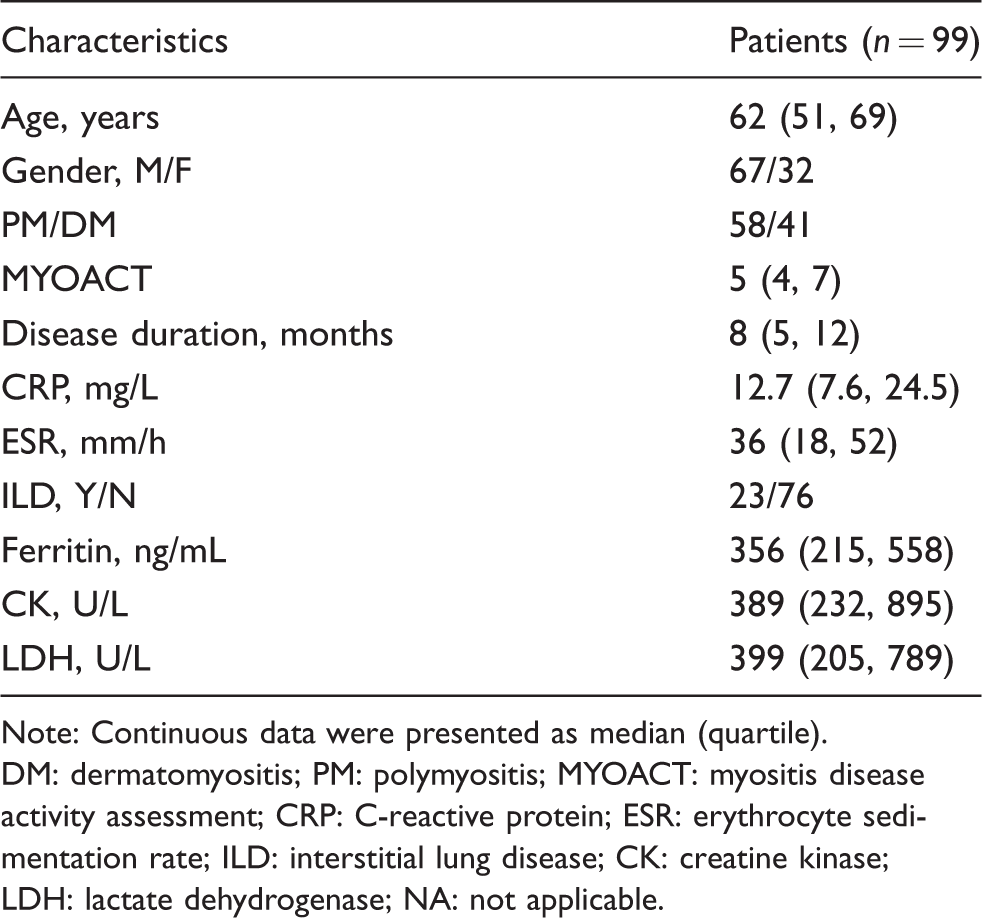
Note: Continuous data were presented as median (quartile).
DM: dermatomyositis; PM: polymyositis; MYOACT: myositis disease activity assessment; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; ILD: interstitial lung disease; CK: creatine kinase; LDH: lactate dehydrogenase; NA: not applicable.
Serum YKL-40 was increased in PM/DM patients
Age and gender between PM/DM patients and healthy controls were not statistically significant (P > 0.05 for both). As shown in Figure 1, the median (interquartile range) concentrations of YKL-40 in PM/DM patients and healthy controls were 51.6 (36.4–63.8) μg/L and 27.8 (22.6–35.0) μg/L (P < 0.01 by Mann-Whitney test). YKL-40 concentration in all controls were less than 100 μg/L, while seven of PM/DMs had YKL-40 more than 100 μg/L.
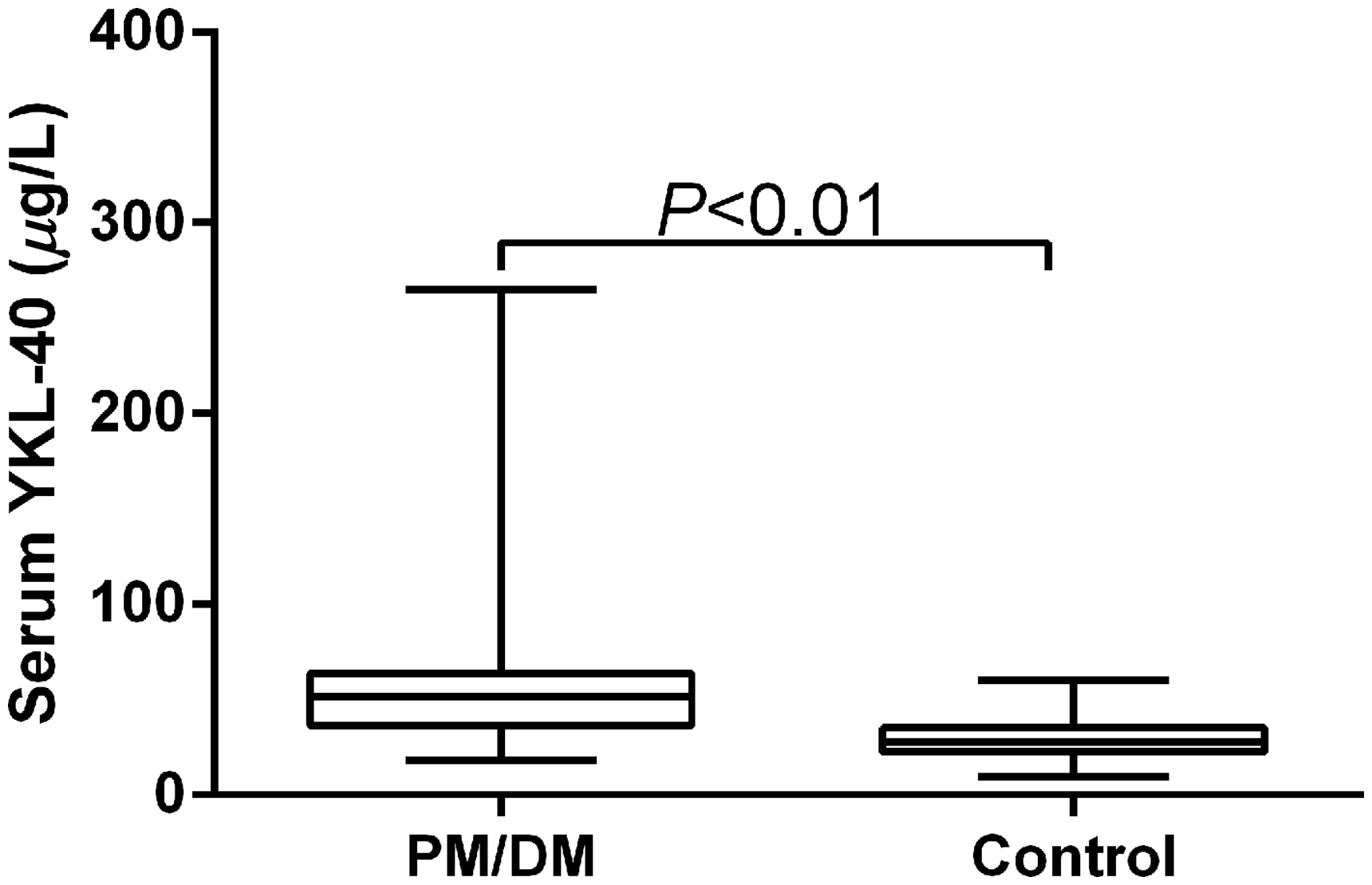
Comparison of YKL-40 between polymyositis/dermatomyositis patients and healthy controls.
Serum YKL-40 was associated with clinical characteristics of PM/DM patients
Next, we analysed the association between YKL-40 and clinical characteristics of PM/DM patients. As shown in Figure 2, there was no significant difference between PM/DM patients group with treatment at the time of study enrolment and those without (P = 0.81 by Mann-Whitney test). Notably, patients with ILD had significantly higher YKL-40 than those without (P = 0.02 by Mann-Whitney test). Besides, using Spearman correlation analysis, we found that YKL-40 was positively correlated with MYOACT, CRP, ESR and ferritin, with coefficients of 0.64, 0.34, 0.61 and 0.61 (P < 0.01 or all), respectively.
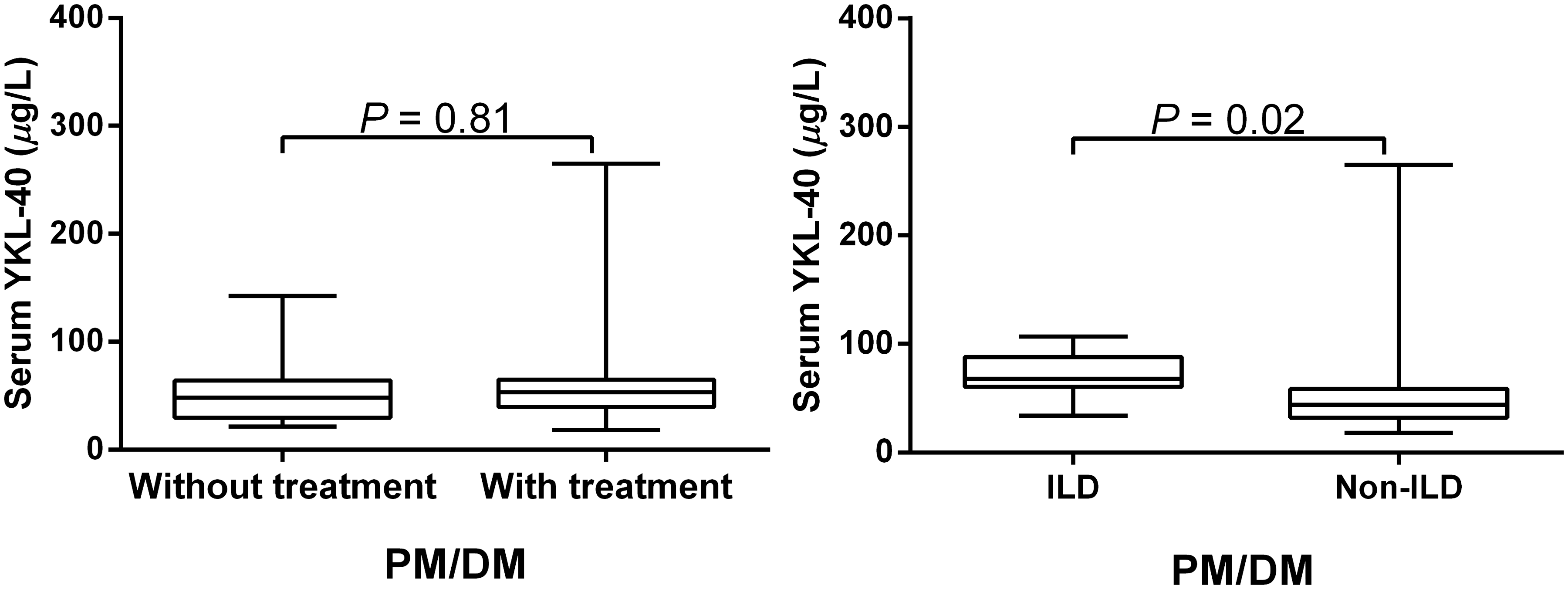
Comparison of YKL-40 between polymyositis/dermatomyositis patients with or without treatment or interstitial lung disease.
Serum YKL-40 is a useful marker for identifying ILD
Considering that patients with ILD had significantly higher YKL-40 than those without, we further analysed the value of YKL-40 for identifying ILD in PM/DM patients. The area under ROC curve (AUC) of YKL-40 was 0.82 (95% CI: 0.74–0.91). At a threshold of 55.9 μg/L, the corresponding sensitivity and specificity were 0.91 (95% CI: 0.72–0.99) and 0.72 (95% CI: 0.61–0.82), respectively.
Discussion
In this study, we investigated the clinical utility of YKL-40 in PM/DM patients. The major findings of this study were: (a) serum YKL-40 concentration was increased in PM/DM; (b) YKL-40 was positively correlated with the disease activity or severity of PM/DM; (c) YKL-40 was a useful biomarker for identifying ILD in PM/DM. Compared with a recently published work concerning YKL-40 and PM/DM, 24 the strengths of this study were: (a) the subjects included in this study were PM/DM patients with or without ILD, and therefore the value of YKL-40 for identification of ILD can be evaluated; (b) the correlation between YKL-40 and disease activity of PD/DM, irrespective ILD involvement, was evaluated.
Like many autoimmune diseases, PM/DM patients had increased serum YKL-40. Elevated YKL-40 may be due to the continuous inflammation response in PD/DM patients. Previous studies have indicated that circulating YKL-40 in healthy volunteers increases after endotoxin 25 or inflammatory cytokines injection. 26 Besides, previous studies have proved that serum YKL-40 is positively associated with CRP, a widely known inflammatory marker.27,28 Besides, like CRP, YKL-40 has been proved to be a risk factor for many types of inflammation-related diseases, such as ischaemic stroke 27 and cancer. 29 These results indicated that YKL-40 is an inflammation-related biomarker.
Sources of increased serum YKL-40 in PM/DM remain largely unknown. We hypothesized that increased YKL-40 in PM/DM was associated with overactivation of monocyte and macrophage. Previous studies have indicated that sCD163, a marker of macrophage activation, 30 is increased in PM/DM patients,9,31 indicating that macrophages are overactivated in PM/DM patients. On the other hand, previous studies also indicated that the expression of YKL-40 is increased in activated macrophages.11,32 Nevertheless, we could not rule-out that other types of cells (e.g. neutrophil, chondrocytes) are not attributed to the increased circulating concentration of YKL-40.
We found that serum YKL-40 was positively correlated with MYOACT, CRP, ferritin and ESR, indicating that it was a potential marker for estimating disease activity of PM/DM. Further, YKL-40 in PM/DM patients with ILD was significantly higher than those without, indicating that it was a potential marker for ILD. The results of ROC curve analysis have greatly supported that YKL-40 is a useful marker for identifying ILD, with an AUC of 0.82. Compared with HRCT, serum YKL-40 determination is an inexpensive and objective test, and thus has potential clinical utility in identifying PM/DM patients complicated with ILD. Taken together, these results indicated that serum YKL-40 measurement in PM/DM patients might facilitate the management of PM/DM patients.
There are three limitations of this study. First, the sample size of this study is small, and the results of this study need to be validated by further studies with large sample size. Second, the study is performed in China. Therefore, the conclusion of presented study may not be extended to other areas. Third, this is a cross-sectional study and findings of this study need to be further validated by longitudinal studies.
Taken together, we found that serum YKL-40 was increased and associated with clinical characteristics in PM/DM. Therefore, it represents a useful biomarker for estimating disease activity or severity of PM/DM. Serum YKL-40 measurement may facilitate the management of PM/DM patients.
Footnotes
Acknowledgements
Comments from yunyu_wei, all the colleagues of the Department of Laboratory Medicine, Wuxi Second People’s Hospital of Nanjing Medical University significantly improved this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Natural Science Foundation of Jiangsu Province (No. BK20171147), Science and Technology Projects of Wuxi City (Nos. YGZXM1501, Q201701), Key Technologies of Prevention and Control for Major and Infectious Diseases (No. GWZX201604).
Ethical approval
Ethical approval for this investigation was obtained from the Research Ethics Committee, Wuxi Second People’s Hospital of Nanjing Medical University, Jiangsu, China
Guarantor
ZJH, TWJ.
Contributorship
(1) Conception and design: Ming-Zhu Gao, Zhi-Jun Han, Ting-Wang Jiang; (2) Administrative support: Yun-Yu, Wei, Qiang-Wei Xu, Rong Ji; (3) Provision of study or patients: Qiang-Wei Xu, Rong Ji; (4) Collection and assembly of data: Qiang-Wei Xu, Rong Ji; (5) Data analysis and interpretation: Ming-Zhu Gao; (6) Manuscript writing: All authors; (7) Final approval of manuscript: All authors.