
Abstract
Human cartilage glycoprotein 39 (YKL-40) is related with presence and extent of atherosclerosis, which can be a new biomarker of inflammation and endothelial dysfunction. The relationship between YKL-40 and endothelial dysfunction in patients with essential hypertension (EH) has not been intensively investigated. The relationship between serum level of YKL-40 and endothelial dysfunction was evaluated in 60 EH subjects and 50 normal control (NEH) subjects. Enzyme-linked immunosorbent assay (ELISA) was used to measure serum levels of YKL-40. Brachial artery flow-mediated vasodilation (FMD) was used to measure endothelial-dependent nitric oxide-mediated vasodilatory capacity as the function of endothelial index. This study demonstrated that YKL-40 expression was significantly increased (p < 0.05) in EH subjects compared with NEH subjects. The FMD was significantly impaired in EH subjects compared with NEH subjects. YKL-40 was not only negatively correlated with FMD, but also with carotid artery intima-media thickness (IMT). Multiple liner regression analysis identified that YKL-40 was independent of FMD development. The level of YKL-40 was elevated in EH patients and inversely related with FMD and may be independent of endothelial dysfunction in EH.
Introduction
YKL-40 has been studied as a potential biomarker of inflammation and endothelial dysfunction, which are associated with cardiovascular disease. 1 Furthermore, YKL-40 is related to cardiovascular and all-cause mortality in patients with stable coronary artery disease. 2 Increased YKL-40 levels predict poor long-term cardiovascular survival in patients with peripheral arterial disease. Further-more, YKL-40 correlates with patients’ ankle-brachial index in peripheral arterial disease in the absence of mediasclerosis. 3 As an impact factor of arterial wall stiffness, the mechanism is possibly due to its connection with arterial endothelium dysfunction. 4 Flow-mediated dilation (FMD) is often used as a noninvasive assessment of endothelial dysfunction. Both 1-year atorvastatin and rosuvastatin treatments significantly improved endothelial function, when assessed with FMD and measured by ultrasonography. 5 Jafari et al. and Jafari and Mohsenin6,7 reported that there was a significantly inverse correlation between YKL-40 and FMD in hypertensive obstructive sleep apnea (H-OSA) and obstructive sleep apnea (OSA) patients. 6 Serum pentraxin-3 levels are closely related with the measures of indirect noninvasive evaluation methods (FMD) in both dipper and non-dipper hypertension patients. 8
Yet little research has been exploring the relationship between essential hypertensive (EH) patients and normotensive people. In this study, the relationship between YKL-40 and endothelial dysfunction in patients with essential hypertension was explored.
Methods
Subjects
Sixty EH non-treated subjects were recruited from the Second Hospital of Shandong University in this case-control study. According to the 2013 Guidelines for the Management of Arterial Hypertension of the European Society of Hypertension and the European Society of Cardiology, the patients were diagnosed. 9 Blood pressure was measured by triplicates. Subjects with secondary hypertension, diabetes, chronic nephrosis, hyperlipidemia, cardiovascular diseases, and/or autoimmune diseases were excluded from this study.
Two experimental groups: EH group (N = 60) and healthy normal patients without essential hypertension (NEH group, N = 50). The mean of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured. The body mass index (BMI) was calculated by the formula of weight/height2 (Kg/m2). The FMD, carotid intima-media thickness (IMT), and YKL-40 were measured. The clinical information were collected for all the subjects, including total cholesterol (TC), fasting blood glucose (FBG), total triglyceride (TG), low density lipoprotein cholesterol (LDL), high density lipoprotein cholesterol (HDL), BMI, and so on (Table 1). This study was approved by ethic committee of the Second Hospital of Shandong University and written consents were obtained from all subjects.
Basic characteristics of two groups.

FPG: fasting blood glucose; TC: total cholesterol; HDL: high density lipoprotein cholesterol; LDL: low density lipoprotein cholesterol; TG: triglyceride; BUN: blood urea nitrogen; Cr: serum creatinine; BMI: body mass index; SBP: systolic pressure; DBP: diastolic pressure; PP: pulse pressure.
Data are presented as mean ± SD or number.
p < 0.05 versus NEH group.
Clinical data
The floor stand model mercurial sphygmomanometer (YUTU, Shanghai, China) was used for measuring blood pressure from the right arm of each subject. Blood pressures were tested twice, at intervals of 2 min with the mean value. Mean pulse pressure was calculated as PPv = SBP − DBP. Anthropo-metric measurements and venous blood samples were obtained. Autonomic Biochemical Analyzer (DVI1650, Bayer, Germany) was applied for measuring FBG, TG, LDL, TC, HDL, and BUN.
Determination of serum YKL-40
Enzyme linked immunosorbent assay (ELISA) was used to measure the serum level of YKL-40. Blood samples were centrifuged at 3000 rpm for 5 min after being left at room temperature for 30 min. The plasma was collected and placed in Eppendorf tuber respectively and stored at −80°C.
Ultrasound measurement
With reference to methods described by Celermajer et al., 10 FMD measurement applied the American GE company LOGIQ7 color Doppler diagnostic system. People in the supine position, right upper limb outreach 15°, palms up and 3 cm brachial artery segment of right elbow joint as target organ. The diameter of brachial artery of people under the conditions were measured 3 times and the mean value was taken as the foundation value. At the same time, the velocity of the blood flow was measured. Then in the right elbow joint of 5.0 to 17.5 cm, we attached a width of 12.5 cm cuff to it, connected to the blood vessel function determination of pressure system (Hokson, American), accelerated pressure to 200 mmHg lasting for 5 min, decompressed to 0 mmHg quickly, waited for 60~90 s and finally measured brachial artery diameter.
FMD was calculated as %change:
(Hyperemia diameter (Dh)−Baseline diameter (Db))/Baseline diameter × 100%,
FMD (%) = (Dh−Db)/Db. IMT was measured by ultrasound in carotid artery according to the guideline for the hypertension in ESH/ESC. 9
Statistical analysis
Statistical analysis was performed using SPSS 20.0. The quantitative variables were expressed as mean ± standard deviation. The comparison of EH and NEH was analyzed with student t-test. The relationship between FMD and correlative index was executed by Pearson correlation. The FMD and the correlation index were studied by multiple liner regression (Ordinary Least Square).
Results
Comparison of common clinical data
SBP of EH was 167.33 ± 18.51 mmHg (range of 115–200 mmHg) and the mean of DBP was 97.30 ± 14.70 mmHg (range of 69–113 mmHg). Fifty normotensive controls (22 females and 28 males) were with a mean age of 57.7 ± 13.4 years (range of 24–84 years). Their SBP was 115.9 ± 10.67 mmHg (range of 90–135 mmHg) and DBP was 76.8 ± 5.9 mmHg (range of 65–90 mmHg). There were no significant differences between the EH and NEH in the age, gender, FBG, TG, BUN, and serum Cr. The hypertensive patients were more likely to develop elevated TC, LDL, BMI. Meanwhile, SBP and DBP were much higher in subjects with HT compared with NEH subjects (Table 1).
The comparison of serum YKL-40 and FMD
Serum level of YKL-40 was compared in EH subjects and normotensive subjects. The level of YKL-40 in EH subjects was 98.04 ± 16.94, while the level of YKL-40 in normotensive subjects was 62.17 ± 19.17. YKL-40 was increased in hypertensive subjects in comparison with in normotensive subjects (p < 0.05). Serum level of FMD was compared in hypertensive subjects and normotensive subjects. The change of FMD in hypertensive subjects is 5.89 ± 1.77, while the change of FMD in normotensive subjects was 7.22 ± 1.28. FMD was decreased in hypertensive subjects than in normotensive subjects (p < 0.05) (Table 2).
Comparison of FMD, IMT, and YKL-40 in two groups.

p < 0.05 versus NEH group.
Correlation analysis between YKL-40 and FMD, IMT
Significant negative correlations were noted between YKL-40 and FMD (Figure 1(a)). Significant positive correlations were observed between YKL-40 and IMT (Figure 1(b)).

(a) Scatter diagram of YKL-40 and FMD in hypertension. (b) YKL-40 and IMT in hypertension.
Correlation analysis between YKL-40 and other indexes
Significant negative correlations were indicated between FMD and SBP, DBP, FBG, TC, LDL, BMI, and IMT (Table 3). Significant positive correlations were mentioned between YKL-40 and SBP, DBP, FBG, TC, LDL, BMI, and IMT (Table 4).
Correlation co-efficiency between FMD and some parameters (n = 60).
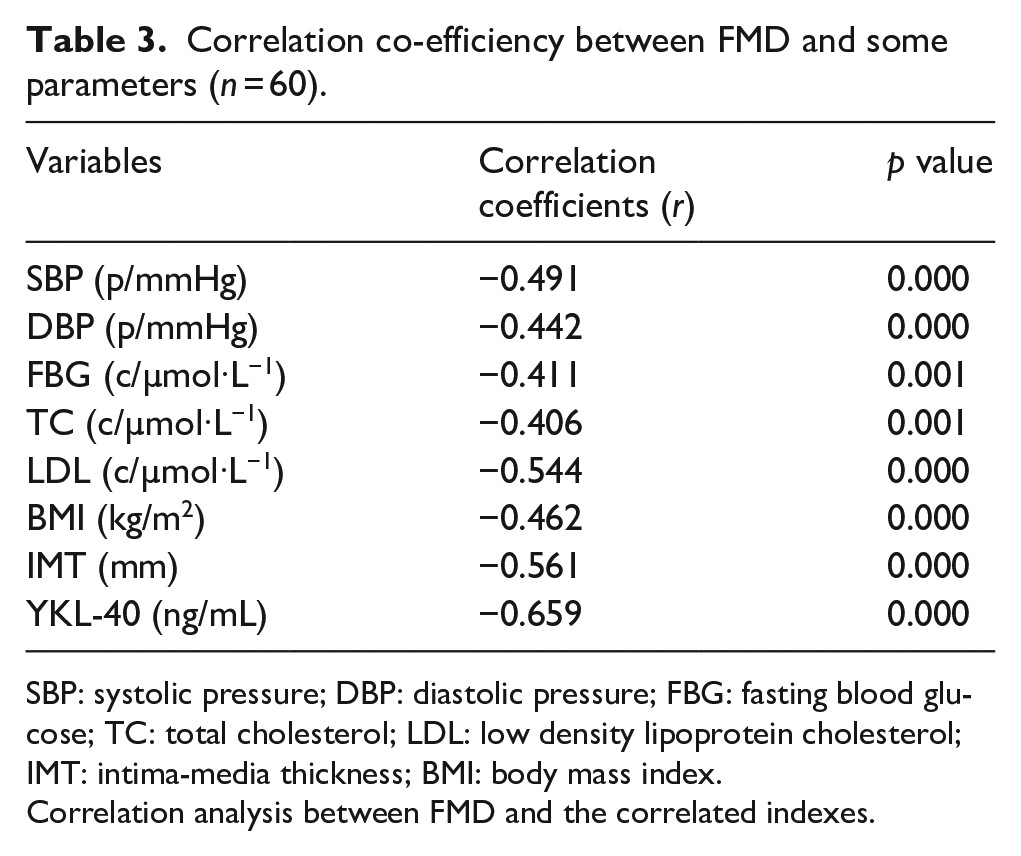
SBP: systolic pressure; DBP: diastolic pressure; FBG: fasting blood glucose; TC: total cholesterol; LDL: low density lipoprotein cholesterol; IMT: intima-media thickness; BMI: body mass index.
Correlation analysis between FMD and the correlated indexes.
Correlation co-efficiency between YKL-40 and some parameters (n = 60).
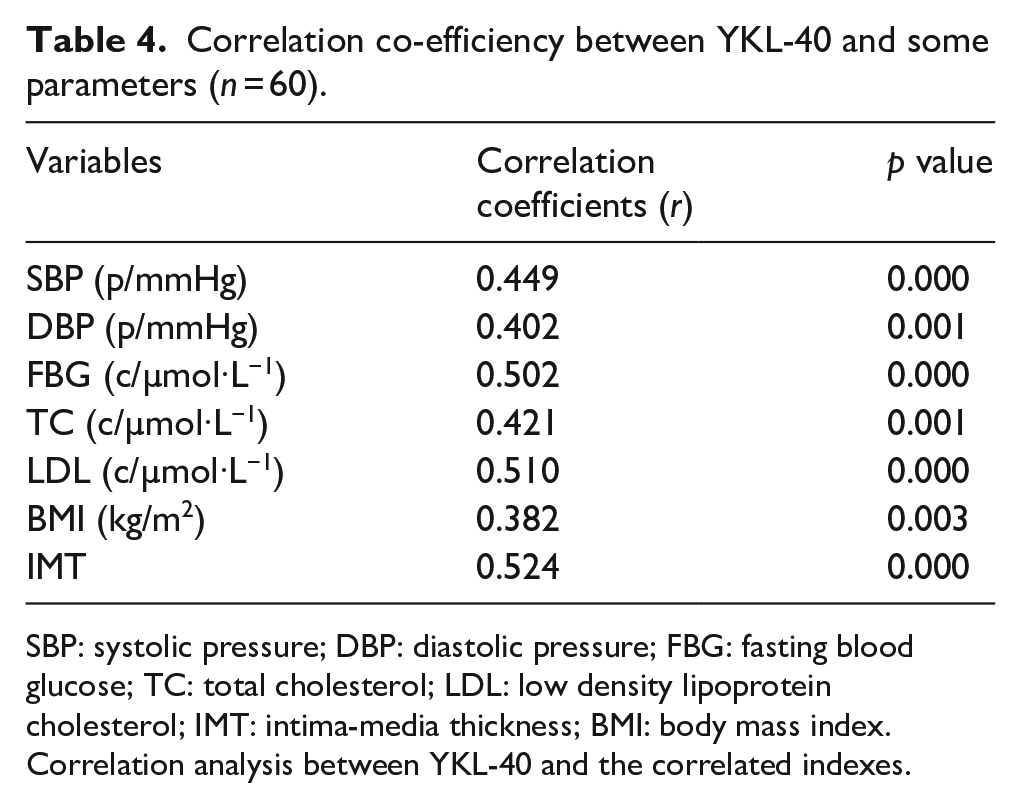
SBP: systolic pressure; DBP: diastolic pressure; FBG: fasting blood glucose; TC: total cholesterol; LDL: low density lipoprotein cholesterol; IMT: intima-media thickness; BMI: body mass index.
Correlation analysis between YKL-40 and the correlated indexes.
Multiple liner regression analysis
Multiple liner regression analysis showed that YKL-40 was an independent determinant of FMD (Table 5).
Multivariate linear regression of the FMD and the correlated indexes.

BMI: body mass index; SBP: systolic pressure; DBP: diastolic pressure; LDL: low density lipoprotein cholesterol; FBG: fasting blood glucose; TC: total cholesterol; IMT: intima-media thickness.
Multivariate linear regression of FMD and the correlated indexes (R2 = 0.622) (n = 60).
Ultrasound measurement of two groups
The peoples’ brachial artery with the color dopplar probe was detected, which indicated that the velocity of blood flow is 142 cm/s (Figure 2(a)). It was found that the blood-flow was slower than before (Figure 2(b)). The rate of change of brachial artery diameter before and after the reactive hyperemia is FMD. An EH patient, was detected the carotid vascular by ultrasound probe, the intima of vascular wall was unsmooth and incrassated, then measurement of the thickness of intima-media of the artery wall was 0.115 cm (>0.09 cm) (Figure 2(c)). A healthy people was detected the carotid vascular by ultrasound probe, and the results was that the intima of vascular wall was very smooth and thin (Figure 2(d)). Result indicated that IMT was thicker in EH subjects than NEH subjects.

Blood flow of the brachial artery in EH (a) and after FMD in EH subjects (b). We pressured to the brachial artery wall to 200 mmHg, and left it to last for 5 min, then decompressed it to 0 mmHg quickly and waited for 60 to 90 s. Carotid artery intima-media thickness (IMT) in EH patients (c) and NEH subjects (d).
Discussion
Chronic inflammation reaction run through the development of hypertension. Hypertensive patients usually have higher plasma concentrations of pro-inflammatory cytokines. 11 YKL-40 is an inflammatory glycoprotein involved in endothelial dysfunction by promoting chemotaxis, cell attachment and migration, reorganization, and tissue remodeling as response to endothelial damage. 12 It can be seen in macrophages and smooth muscle cells in atherosclerotic plaques with the highest expression in macrophages in the early lesion of atherosclerosis. 12 Moreover, it has been proposed as a new marker of endothelial dysfunction and atherosclerosis. 13 Our study found that YKL-40 is obviously elevated in EH subjects compared with NEH patients (p < 0.05).
Endothelial function is a crucial factor in the pathogenesis of atherosclerosis, hypertension and heart failure. 14 Evidences showed that endothelial function is closely related to cardiovascular disease, and endothelial dysfunction is one of the vital factors leading to atherosclerosis disease. 15 FMD is the most widely used method to assess endothelial function. It is considered as the most reproducible, predictive, inexpensive and low-risk non-invasive method of endothelial function evaluation. 16 FMD stimulated the endothelium cells to release nitric oxide, resulting in vasodilation. It can be quantified as an index of vasomotor function. 14 The early stage pattern of atherosclerosis is the increase of IMT of artery. FMD and IMT are associated with increased cardiovascular risk in symptomatic peripheral arterial disease. 17 Michelsen et al. 18 found that patients with carotid stenosis had a high level of YKL-40. Their clinical experiments found that YKL-40 increased MMP-9 expression and THP-1 monocytes activation, involving p38 mitogen-activated protein kinase activation. YKL-40 affected the carotid stenosis probably by releasing macrophage and degrading substrate. YKL-40 level could reflect the extent of atherosclerosis in essential hypertensive patients.
Growing clinical evidences have indicated that aberrant expression of YKL-40 is closely connected with endothelial dysfunction and poor cardiovascular outcome.2,19 And it was reported that YKL-40 is closely associated with hypertension incidence. 19 Jafari et al. found that YKL-40 was significantly elevated in hypertensive OSA (55.267.9 ng/mL vs 35.664.2 ng/mL in normotensive OSA, p = 0.02), while the FMD (r = 20.52, p = 0.013) decreased in hypertensive OSA. And they found that there was a significant negative correlation between FMD and YKL-40 (r = 0.52, p = 0.013). 6
Multiple linear regression suggested that YKL-40 (B = −0.281, p < 0.05) was correlated with FMD, independent of BMI, LDL, TC, TG, FBG, and IMT (Table 5), which suggested that YKL-40 is an independent impact factor of endothelial function in EH groups. Since YKL-40 is an inflammation factor secreted by macrophage in the artery plaque. Inflammation has been shown to suppress NOS activity. 11
To some extent, YKL-40 possibly indicated the degree of endothelial dysfunction in hypertensive people. The early stage of coronary atherosclerosis is characterized by endothelial dysfunction. FMD as a noninvasive peripheral endothelial function test has the prognostic value for cardiovascular disease. 20 Endothelial dysfunction is an early marker for atherosclerosis and essential hypertension, and it can be detected before structure changes to the vessel wall which are apparent on angiography or ultrasound.15,21 Fortunately, total 3 years’ following studies found that FMD remained a significant predictor of TOD (target organ damage) number increase in essential hypertensive patients. 22 Our results indicated that YKL-40 was negatively correlated with FMD. Thus, YKL-40 might be a useful prognostic indicator for early target organ damage in EH patients.
There are some limitation in this study. Firstly, our study was a case-control study, but the sample size was small. Secondly, the underlying mechanism of YKL-40 was not explored due to limited funding and experimental design. Finally, our results need further research and more complete experimental design to verify.
Conclusion
In conclusion, YKL-40 levels of subjects with EH were elevated and expression of YKL-40 was negatively correlated with FMD. In most cases, YKL-40 levels reflected endothelial dysfunction and early changes in atherosclerosis in patients with EH. Therefore, YKL-40 may be used as a prognostic marker for early target organ damage in patients with EH.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of The Second Hospital of Shandong University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grant from the Scientific Development Plan of Shandong Province (grant number 2017G006029).
Informed consent
Written informed consent was obtained from all subjects before the study.