
Abstract
Background
Spurious hyperkalaemia is a relatively common occurrence in samples originating from primary care. Failure to identify spurious hyperkalaemia carries a significant risk of patient mismanagement. We have carried out a retrospective evaluation to review the impact of the use of centrifuges in primary care for biochemistry blood samples on the management of hyperkalaemia.
Methods
Serum potassium concentrations in samples received from primary care were reviewed for six months prior to and after the implementation of on-site centrifugation. Samples exhibiting significant hyperkalaemia (serum potassium >6.0 mmol/L) were further investigated to ascertain the degree of patient follow-up.
Results
There was a significant decrease in the number of samples exhibiting marked hyperkalaemia following the implementation (2244 versus 524; P < 0.0001). In terms of patient follow-up, we observed a reduction in the number of patients exhibiting pseudohyperkalaemia that previously had led to inappropriate hospital admissions over the same time period (6 cases postimplementation versus 22 cases preimplementation). We also observed an increase in the number of patients exhibiting true hyperkalaemia during the six-month period postimplementation (33 cases postimplementation versus 6 cases preimplementation).
Conclusions
The centrifugation of serum samples in primary care improves the sample quality and the integrity of the potassium results reported. We have also demonstrated evidence of an improvement in patient management and quality of care.
Introduction
Pseudohyperkalaemia is a phenomenon characterized by apparently increased serum potassium concentration in vitro in the context of a normal in vivo blood potassium concentration. Commonly encountered causes include thrombocytosis, ‘leaky cell syndrome’ and preanalytical variables such as haemolysis, extremes of temperature and delays in sample centrifugation. 1
The Clinical and Laboratory Standards Institute recommends that serum samples are centrifuged within two hours of collection to ensure acceptable sample integrity. 2 The National Quality Standards Institute supports this by recommending that laboratory management should establish a procedure for the transport of samples which ensure they arrive within a timeframe appropriate to the nature of the requested examinations and are protected from deterioration. The use of serum separator tubes and their centrifugation in a correct and timely manner stabilizes the majority of biochemical analytes and helps overcome these problems. 3
Pseudohyperkalaemia causes uncertainty in the interpretation of increased serum potassium concentration, as it is often difficult to ascertain whether the occurrence of hyperkalaemia is genuine. A telephone conversation with the general practitioner (GP) or out-of-hours primary care service maybe required. The GP must decide whether repeat venepuncture is required (with rapid transport of the sample to the laboratory) resulting in inconvenience to the patient. In many such cases, the potassium concentration on repeat sampling is found to be within the reference interval. However, failure to undertake repeat sampling may result in failure to identify a true case of hyperkalaemia. 4,5
An evaluation was carried out to investigate the impact of centrifugation of samples originating in primary care on pseudohyperkalaemia. We also investigated the ‘appropriateness’ of following-up patients with marked hyperkalaemia (potassium concentration >6.0 mmol/L).
Methods
The laboratory information system APEX (iSOFT, Banbury, Oxfordshire, UK) was interrogated for primary care serum potassium data from January to June 2010 (when <20% of samples were centrifuged at source) and January to June 2011 (when >95% of samples were centrifuged at source). All samples from the 86 GP practices across National Health Service Grampian were included. The total numbers of samples received exhibiting normokalaemia (potassium 3.5–5.2 mmol/L), hypokalaemia (potassium <3.5 mmol/L), moderate hyperkalaemia (potassium 5.3–6.0 mmol/L) and marked hyperkalaemia (potassium >6.0 mmol/L) both pre- and postimplementation were compared by Chi-squared contingency testing (Graphpad Prism 5, La Jolla, CA, USA). Clinical records on patients exhibiting marked hyperkalaemia were examined to ascertain the follow-up received by patients. If pseudohyperkalaemia was confirmed by the finding of normokalaemia (potassium 3.5–5.2 mmol/L) in a fresh repeat sample then the follow-up testing was classified as inappropriate since the original result was most likely due to a delay in sample centrifugation. Conversely, if hyperkalaemia was confirmed on the repeat specimen, then the follow-up was deemed as appropriate.
Results
Effect of primary care centrifugation on the serum potassium results.
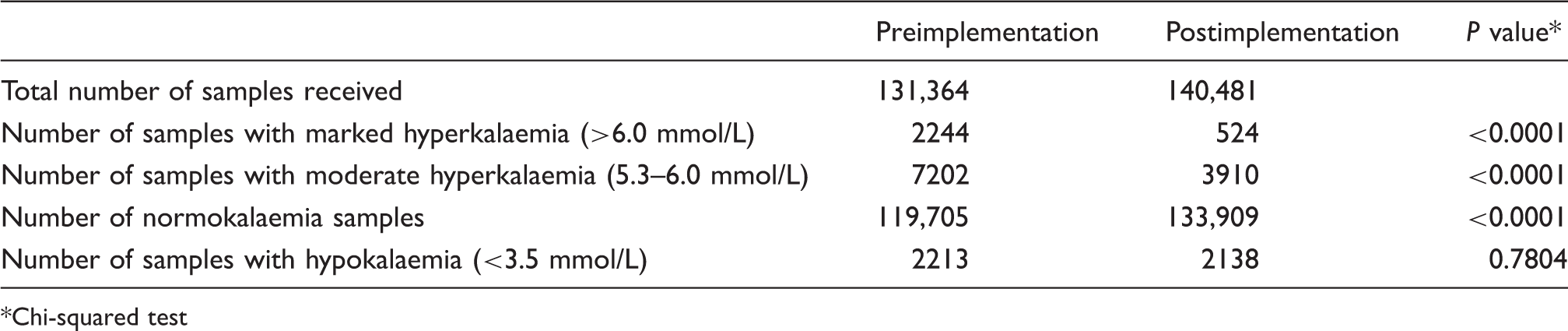
Chi-squared test
The number of cases representing appropriate follow-up and investigation of genuine hyperkalaemia by GPs increased significantly as a result of primary care centrifugation. During the preimplementation period, a single case of hyperkalaemia confirmed on follow-up by the GP (serum potassium >5.3 mmol/L on repeat sampling) was identified. In contrast, in the postimplementation period, there were 23 such cases identified. In addition, the number of hospital admissions resulting from cases of marked hyperkalaemia in the community requiring urgent treatment increased from 5 to 10 with the introduction of primary care centrifugation.
Prior to implementation, eight patients were inappropriately admitted to hospital with pseudohyperkalaemia compared with no such admissions in the postimplementation period. A similar trend occurred with GPs, where repeat blood testing was carried out following the identification of a falsely elevated serum potassium concentration. There were 14 such cases prior to the implementation. In contrast, only six cases were observed in the postimplementation period.
Discussion
The findings from our study have demonstrated that the timely centrifugation of blood samples originating from primary care not only improves sample quality, but also improves the patient care pathway. We observed a significant decrease in the number of samples exhibiting hyperkalaemia, with a concurrent increase in the number of samples exhibiting normokalaemia. Consequently, there has been a reduction in the number of cases of presumed pseudohyperkalaemia. The centrifugation of samples in primary care enables GPs and laboratory staff to have more confidence in the potassium results obtained and allows appropriate follow-up of hyperkalaemia. The number of actual cases of patient admission and GP follow-up due to pseudohyperkalaemia has decreased as a result of the implementation.
In addition, as training and education were gradually rolled-out to all GP practices, the handling of samples and centrifugation improved significantly. This has since resulted in further decreases in the number of cases of pseudohyperkalaemia. Importantly, the number of true hyperkalaemia cases identified increased, where previously they may well have been overlooked and ascribed to delays in sample separation. The observations from this study are consistent with previously published data highlighting that the rapid centrifugation of blood samples improves the quality of results reported by laboratories. 3,5,6
In addition to the obvious improvements in patient management, there were many other benefits to both primary care and the laboratory. Centrifugation in practices has the potential to reduce the number of repeat bloods required. This approach also reduces time constraints on the GP practices regarding the timing of blood collection and sample transport to the laboratory.
In conclusion, we have shown that centrifugation of blood samples in primary care improves the quality of results obtained, and positively impacts on patient care.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
N/A.
Guarantor
HET.
Contributorship
HET and RWAP wrote the paper and performed all data analysis. All authors reviewed and edited the final version of the manuscript.