
Abstract
Background
Tandem mass spectrometry (MS/MS) has recently become an alternative method for the newborn screening of sickle cell disorders (SCD), as it is able to detect haemoglobin (Hb) peptides following digestion of bloodspots with trypsin. Using the SpOtOn Diagnostics Reagent Kit, we previously developed a screening protocol to detect only the disease states of SCD, using action values based on the ratio between the variant Hb peptide to wild-type peptide abundances for the HbS, C, DPunjab, OArab, E and Lepore peptides.
Methods
Action values using the ratios between the wild type HbA (ßT1-3) peptides and the foetal Hb (γT2) peptide were developed to identify bloodspot samples from premature and transfused infants. An evaluation was undertaken to assess the transferability of the action values onto an additional MS/MS instrument. We report here our experience using this MS/MS protocol.
Results
During a three-year period, we screened 100,456 babies and identified 10 SCD cases (1 HbS/HPFH, 5 HbS/S and 4 HbS/C) and a case of HbE/ß-thalassaemia that was identified as a by-product. The Hb variant to wild-type peptide ratio action values were transferable to a second MS/MS instrument. Our protocol prevented the identification of an estimated 810 carrier infants. Gestational age-related action values for HbA to HbF peptide ratios were required to minimize the number of samples referred for second-line testing to exclude ß-thalassaemia.
Conclusion
MS/MS is a robust alternative screening technology for SCD; in addition, it also optimizes the use of equipment and expertise that currently exist in newborn screening laboratories.
Introduction
Sickle cell disorders (SCD) are due to genetic mutations that alter the structure of the haemoglobin (Hb) peptide molecule. SCD is associated with high morbidity and mortality during early childhood. 1 The aim of newborn screening is to identify infants with the disease states to ensure early treatment to prevent adverse outcomes. 1 Those Hb variants for which there is evidence that early intervention is likely to be beneficial, and are therefore specified as part of the UK National Screening Programme, are as follows: sickle cell anaemia (HbS/S), Hb S/ß-thalassaemia (inclusive of Hb S/ß+, Hb S/ß0, HbS/δß, HbS/γδß and Hb S/Lepore), Hb S/HPFH, Hb S/C, HbS/DPunjab, HbS/E and HbS/OArab.
High-performance liquid chromatography (HPLC) and isoelectric focussing (IEF) have been utilized for screening in many countries worldwide. However, these analytical platforms identify carriers and other non-clinically significant variants as by-products. More recently, tandem mass spectrometry (MS/MS) has been used as an alternative technology for the screening of SCD.2–4 MS/MS is able to detect Hb peptides following digestion of bloodspots with trypsin, which results in the formation of 15 reproducible peptides of the wild-type HbA ß-chain (ßT1-15).5,6 Mutations alter cleavage sites and generate peptides specific to the mutation present. Mutations for the HbS and C variants are located in the ßT1 peptide, HbE in the ßT3 peptide and OArab and DPunjab in the ßT13 peptide. If these mutations are present, the abundances of these specific peptides are increased relative to the normal wild-type peptides.
Using the SpOtOn Diagnostics Reagent Kit for MS/MS, 7 we recently described a screening protocol that utilized action values based on the ratio between the Hb variant peptide abundance and the wild-type peptide abundance. This protocol was designed to detect only the disease states of SCD. 4 MS/MS acquisition data are exported into Excel and then analysed using an ‘In house’ Excel macro programme. The macro sorts the quality control (QC) samples from the routine screening samples and then analyses the peptide abundances and ratios. Only the internal standard, HbA (ßT1-3) and foetal Hb (HbF) peptide abundances and corresponding ratios to HbF are revealed to the laboratory scientist. These are the parameters required to check for; appropriate sample digestion with trypsin, prematurity and transfusion status. All other data are locked and not available to be routinely viewed. Those bloodspot samples with an S:A ratio <0.1 are classified as not suspected as having SCD. Those with an S:A ratio ≥2.1 (99th centile of an HbS carrier infant group) are classified as suspected for SCD (i.e. HbS/S, HbS/C, HbS/ß-thal, HbS/Lepore and HbS/HPFH) and then referred for second-line confirmatory testing (HPLC). For those samples with an S:A ratio ≥0.1 but <2.1, the postanalytical macro programme checks for other interacting peptides that may cause SCD (i.e. HbS/C (C:A ≥ 0.5), HbS/DPunjab (D:A ≥ 1.2), HbS/E (E:A ≥ 0.1) and HbS/OArab (O:A ≥ 0.2). If an additional variant peptide is identified, the results are flagged to alert the laboratory scientist, and the sample is then referred for second-line testing. In the absence of an interacting peptide, the sample is reported as not suspected. Action values were also developed to identify bloodspot samples from premature and transfused infants using the ratios between the wild-type HbA (ßT1-3) peptides and the HbF (γT2) peptide. Therefore, MS/MS offers the ability to detect only the clinically relevant Hb variant peptides.
There are several issues to consider for the newborn screening of SCD. The first is the low expression of the HbA ß-chains during the first week of life, particularly in premature infants. 1 HbA can be detected as early as 24 weeks’ gestation, but the results obtained from premature infants must be interpreted with caution to prevent false-negative cases. 1 In addition, the presence of transfused red cells in a newborn will also affect the interpretation of results. 1 To mitigate this, UK policy states that all newborn babies should have a pretransfusion bloodspot sample collected where possible. The primary method to identify that an infant has been transfused is by the information provided on the newborn screening card, but this is not always stated. 1 Those samples from infants who have received a red cell transfusion should be referred for analysis to detect the presence of the sickle globin gene. 1 In addition, UK screening policy states that babies up to the age of one year should be offered screening. However, older infants have increased amounts of HbA relative to HbF, and such samples may be misinterpreted as being a sample taken from a transfused infant. It is therefore important that the screening protocol is able to identify samples from premature infants, older infants and those infants who have received a transfusion. To identify such samples, we assessed the proportion of HbA and HbF present in the sample by using ratios between the wild-type HbA peptides (ßT1-3) and the HbF (γT2) peptide. Action values were then generated based on the 0.1st and 99.9th centile values for these ratios. Due to the changes in Hb chain production during development, the gestational age of the infant will have a significant effect on the action values. The process to identify samples from premature or transfused infants will result in the detection of cases of ß-thalassaemia as clinically relevant by-products. Screening programmes using HPLC with an HbA action value of ≤1.5% of the total Hb have been shown to be reliable for the detection of ß-thalassaemia. 8 However, no study has evaluated this HbA action value of ≤1.5% to that of the HbA and HbF peptide ratios obtained using MS/MS.
Our initial validation work was undertaken on a single MS/MS instrument (Waters Xevo-TQ). 4 To ensure the robustness of the screening programme for SCD, we assessed the transferability of our screening action values onto an additional MS/MS instrument (Waters Xevo-TQS). Our protocol to detect only the disease states of SCD was endorsed by the UK National Screening Committee and implemented in Wales in June 2013. We report here our experience with screening for SCD using MS/MS and our protocol to detect only the disease states of SCD.
Methods
Samples
Dried bloodspots collected and sent for analysis to the Wales Newborn Screening Laboratory as part of the routine Wales Newborn Bloodspot Screening Programme from June 2013 to May 2016 were used. PerkinElmer 226 paper was used for routine bloodspot collection and for the preparation of QC samples.
Analysis of Hb peptides in bloodspots by MS/MS
Analysis of bloodspot Hb tryptic peptides was undertaken as described previously using the Hb variant Kit from SpOtOn Clinical Diagnostics (London UK). 7 In brief, bloodspots (3.2 mm diameter) were punched into 96-deep well microplates, 50 μL of internal standard (modified stable isotope labelled sickle T1 peptide) was then added and mixed. Fifty microlitres of trypsin reagent was then added to each bloodspot, mixed for 30 min at 37℃ and then diluted in 1 mL of mobile phase (acetonitrile:water [50:50], with 0.025% formic acid). The plates were then sealed, centrifuged and placed onto the auto-sampler of the MS/MS.
Two Waters MS/MS instruments (Xevo-TQ and Xevo-TQS) were used. Due to the difference in sensitivity of the instruments, different volumes of the prepared bloodspot samples were injected (10 µL on the TQ-MS/MS and 2 µL on the TQS-MS/MS) into the mobile phase stream using a Waters Acquity system. The sample was directly introduced into the electrospray source in the positive ionization mode without prior chromatographic separation. Analysis was performed using the multiple-reaction monitoring mode with a dwell time of 0.2 s per channel. The total acquisition time was 2 min. A postinjection wash cycle was included to prevent any sample carryover. Multiple-reaction monitoring acquisition mode is used to restrict the analysis to the specific clinically relevant peptides to detect only those disorders as outlined previously. 1
MS/MS acquisition list for the relevant Hb peptides and internal standard, their parent and daughter ions and the peptide ratios used in the screening protocol.
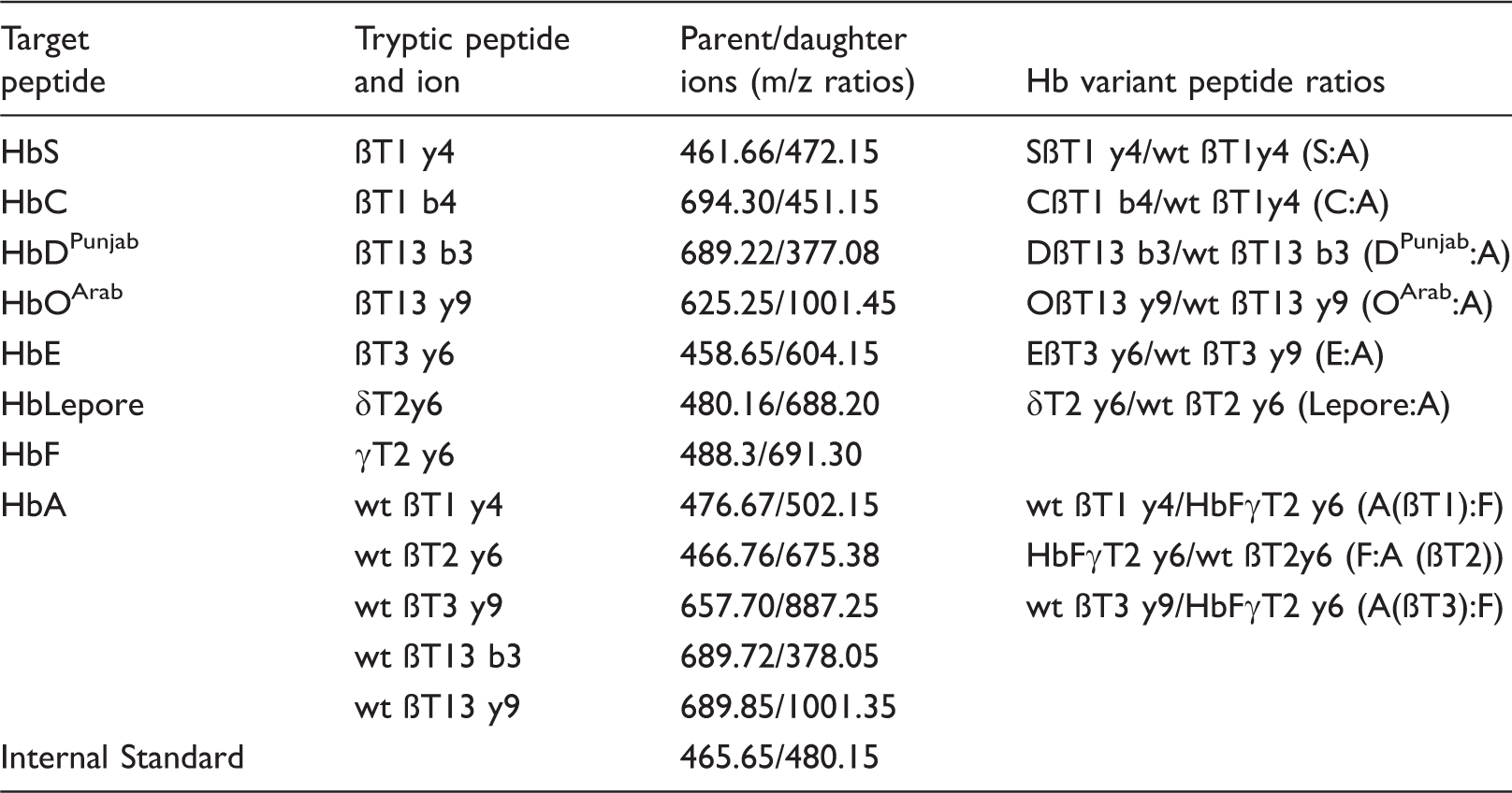
wt: wild-type.
Assessment of assay performance
The assay and the postanalytical data analysis protocol were quality assured by the use of QC samples prepared using anonymized residual liquid blood samples from subjects with confirmed Hb variant disorders (Cardiff Haemoglobinopathy Laboratory). Bloodspot QC samples were prepared by pipetting 50 µL of liquid blood onto filter paper. Due to the rarity of the of the OArab and Lepore variants, liquid QC samples were prepared by pooling and mixing bloodspot extracts. The limit of detection of the method was assessed by preparing sequential dilutions of a liquid blood sample from a patient with SCD (HbSS) into anonymized residual pooled cord blood samples. Two separate series were prepared and analysed on both MS/MS instruments and by HPLC (Bio-Rad Variant™ II).
Transferability of screening cut-offs on MS/MS instruments
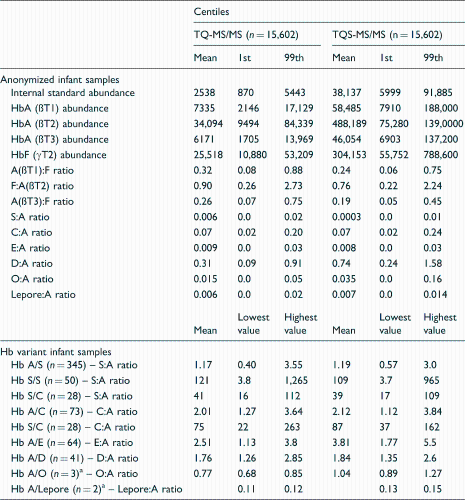
To assess the effect of MS/MS instrument bias, the samples for the generation of screening action values for the Hb peptide abundances and ratios were analysed on two MS/MS systems (Waters Xevo-TQ and Xevo-TQS). To assess the transferability of the S:A ratio action values, we analysed bloodspot tryptic extracts on both instruments using normal Hb infant samples (n = 5539), HbS carrier infants (n = 345), HbS/S (n = 50), HbS/C (n = 28), HbS/ß-thalassaemia (n = 3) and HbS/HPFH (n = 2) infant samples (Figure 1). In addition, a larger number of routine screening samples were also analysed (n = 15,602) on both instruments. The mean, 1st and 99th centiles for the various Hb variant to wild-type peptide ratios were calculated for those samples from normal Hb infants and the HbS carrier infants. Ratios for the various Hb variants (both heterozygous and homozygous states) were calculated as the mean, lowest and highest values observed (Table 2). The samples from the Hb variant infants were provided by the Great Ormond Street Hospital, Newborn Screening Laboratory and were classified on the basis of first line testing with HPLC (Variant™NBS, Bio-Rad Laboratories) and with second-line testing by IEF (Perkin Elmer). Due to the rarity of the Lepore and OArab variants, the samples from two Hb Lepore and three Hb OArab adult carriers were used to demonstrate the ability of the assay to detect these peptides. Samples from 12 ß-thalassaemia cases were also included (six of which had corresponding HPLC %HbA results).
Relationship between the S:A ratio in samples analysed on both the TQ and TQS-MS/MS platforms (NB – the majority of the results obtained for HbAA samples are <0.01). Comparison of Hb peptide abundances and ratios obtained in anonymized normal Hb infant samples and in various Hb variant phenotypes using two different MS/MS instruments. Adult samples.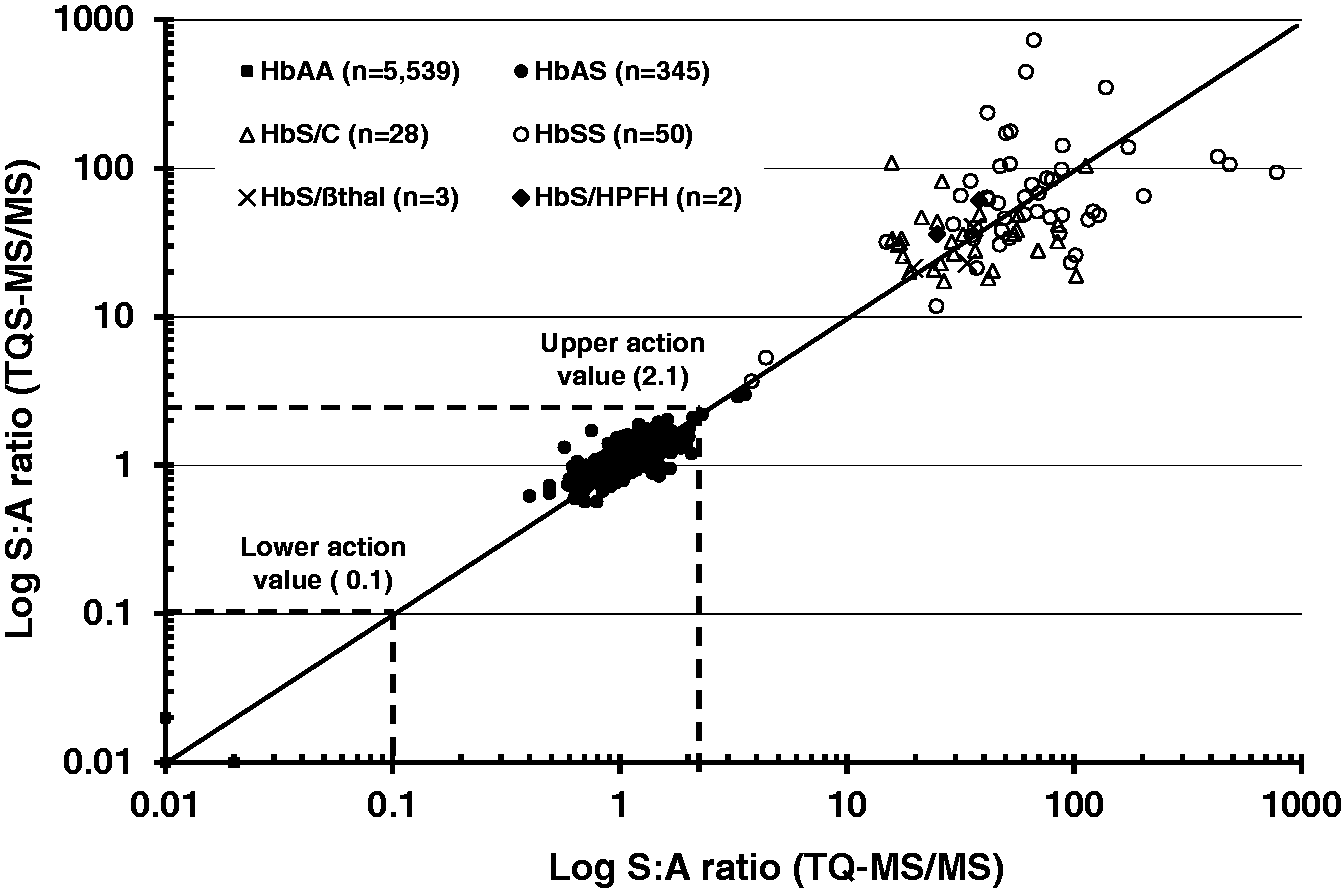
Assessment of Hb peptides by MS/MS to detect samples from premature and transfused infants
Using 13,239 screen-negative samples from our parallel study, 4 the A(ßT1):F, F:A(ßT2) and A(ßT3):F ratios and the gestational age (GA) of the infant were correlated to provide information on the expected amounts of HbA and HbF relative to the GA of the infant. Routine newborn bloodspot samples received marked as transfused were also analysed and the various HbA and HbF ratios were calculated.
Assessment of the HPLC %HbA cut-off and F:A(ßT2) peptide ratios by MS/MS to detect cases of ß-thalassaemia
To assess the recommended HPLC action value of HbA ≤ 1.5% to identify cases of ß-thalassaemia, we analysed a series of bloodspot samples from infants (n = 55) with a varying GA (23–42 weeks) and bloodspots from cases of ß-thalassaemia major (n = 6) using both HPLC and MS/MS to correlate the association between the two variables.
Assessment of Hb peptides by MS/MS to detect samples from older infants
Residual anonymized bloodspot samples from 354 infants from one month of age up to one year were collected and analysed.
Statistical analysis
Data were exported to Excel 2007 for analysis and centiles for the relevant peptide abundances and ratios were calculated using SPSS statistical package (SPSS v16).
Results
Assay performance
The inter-assay CVs for the various peptide ratios ranged from 8.9% to 21.2%. For the limit of detection experiments, the first sample series gave %HbS results ranging from 39% to 1.7%, with corresponding S:A ratios of 3.4 to 0.1 on the TQ-MS/MS and 3.6 to 0.16 on the TQS-MS/MS. The %HbS for the second series ranged from 8.6% to 0.7% with the S:A ratios ranging from 0.74 to 0.06 on the TQ-MS/MS and 0.77 to 0.07 on the TQS-MS/MS.
Data from screening programme
During the three-year period (June 2013 to May 2016), a total of 100,456 newborns were screened for SCD using our protocol. Ten true-positive and six false-positive SCD cases were identified. One clinically significant by-product was also detected. To date, no false-negative cases have been identified.
The 10 true-positive SCD cases (one HbS/HPFH, five HbS/S and four HbS/C) all had S:A ratios above the action value of ≥2.1 and were confirmed by the Cardiff Haemoglobinopathy Laboratory. The S:A ratio in the HbS/HPFH case was 25.5; in the HbS/S patients, the S:A ratios ranged from 20.6 to 51.1. In the HbS/C patients, the S:A ratios ranged from 14.2 to 24.4 and the C:A ratios from 25.9 to 48.7. The HbE/ß-thalassaemia case was detected as a by-product due to the presence of a low ßT3 peptide abundance of 609 (action value ≤1094) and a low A(ßT3):F ratio of 0.05 (action value ≤0.06).
The six false-positive cases were classified on screening as one HbS/S, one HbS/C, one case with a low A(ßT1):F ratio and three HbS/D cases. The false-positive HbS/S case had an increased S:A ratio of 2.34, but the A(ßT1):F ratio was normal. HPLC analysis of this sample showed an HbS of 11.1% and an HbA of 11.4%. This infant had been confirmed as an HbS carrier by prenatal genetic testing. The false-positive HbS/C case was a premature HbC carrier infant (GA: 33 weeks) and had a C:A ratio of 3.04 and an S:A ratio of 0.15. The infant with the low A(ßT1):F ratio (0.04, action value ≤0.08) was a premature HbS carrier infant (GA: 34 weeks). The three false-positive HbS/D cases were referred for second-line testing by HPLC and were shown to be HbS carrier infants. These cases had S:A ratios above the action value of ≥0.1 (1.02, 1.14 and 1.47) in conjunction with a D:A ratio above the action value of ≥1.2 (1.47, 1.87 and 1.24), these infants were all premature (GA: <34 weeks).
Our protocol is designed not to identify carrier states. 4 To assess the number of carrier infants who were appropriately not identified by our protocol, the excel data sheets for six months data (n = 17,737 infants) were anonymized and un-blinded. A total of 143 carriers were revealed (52 HbS, 7 HbC, 65 HbD and 19 HbE). Therefore, based on the total numbers screened during this three-year period (100,456), it is estimated that approximately 810 carrier infants were appropriately not identified.
MS/MS instrument comparisons
Differences in the abundances of the internal standard, HbA(ßT1-3) and HbF peptides were observed between the two instruments (Table 2). Differences were also observed for the various A:F ratios. The relationships for the various HbA to HbF peptide ratios between the two different MS/MS systems were linear (r values obtained > 0.95, data not shown). Excellent agreement for the S:A ratio was observed between the two instruments (Figure 1). The mean (1st and 99th centile) ratio for 345 HbS carrier samples was 1.17 (0.58 and 2.09) on the TQ-MS/MS and 1.19 (0.63 and 2.07) on the TQS-MS/MS. In addition, no bias was observed in the S:A ratios at two different peptide concentrations in QC samples (data not shown). The various variant to wild-type peptide ratios were able to distinguish between the normal Hb infant group, heterozygous and homozygous states. However, the ability of the D:A ratio to distinguish between the normal Hb infant group and the Hb DPunjab carrier infants was less well resolved on the TQS-MS/MS instrument (Table 2). The mean (lowest and highest) F:A(ßT2) ratio observed in the samples from the 12 ß-thalassaemia cases was 192 (17.7 and 693) on the TQ-MS/MS and 230 (13.4 and 845) on the TQS-MS/MS.
Assessment of Hb peptides by MS/MS to detect samples from premature and transfused infants
A positive association between the GA of the infant and the A(ßT1):F ratio was observed, whereas an inverse association between GA and F:A(ßT2) ratio was observed (Figure 2). During the three-year period, we received a total of 71 samples from infants following a red cell transfusion where a pretransfusion sample had not been collected. The mean (range) A(ßT1):F, F:A(ßT2) and A(ßT3):F ratios were: 12.1 (0.7–235), 0.14 (0.0–0.42) and 7.43 (0.42–107), respectively. All 71 samples were referred for sickle mutation analysis (HBB gene in exon 1 [c.20A > T], p.[Glu7Val]). Of these 71 cases, two HbS carriers were identified. On repeat full analysis, the S:A ratio was < 0.1 in both cases. However, the HbS peptide abundance was elevated more than four times the background signal. All carrier infants identified as false positives were referred for follow-up.
Relationship between the gestational age and HbA(ßT1):F ratio (a) and HbF:A(ßT2) (b).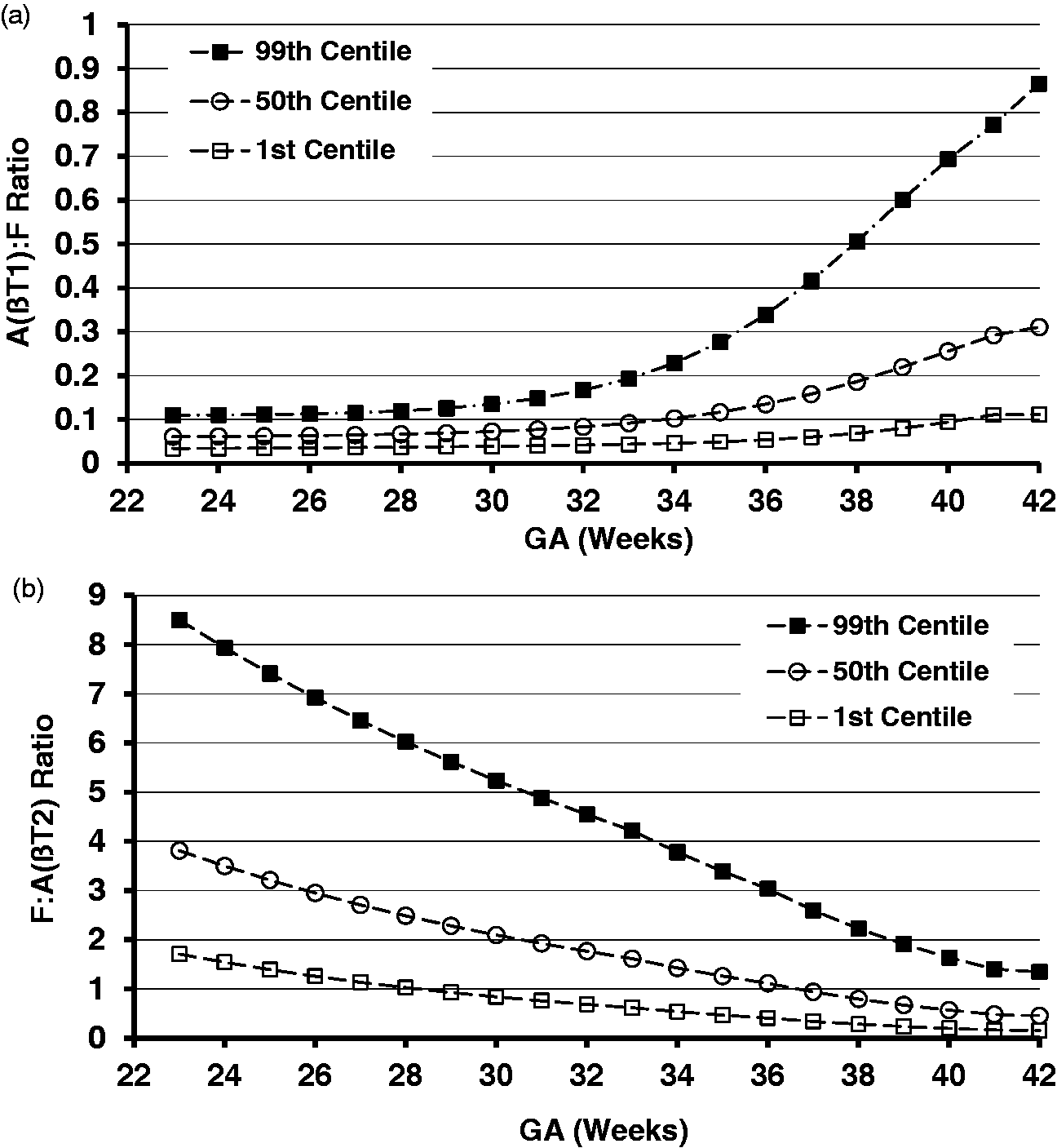
Comparison of %HbA by HPLC and F:A(ßT2) ratios by MS/MS results to detect cases of ß-thalassaemia
The corresponding %HbA results by HPLC and F:A(ßT2) ratios by MS/MS from the premature and term infants and the ß-thalassaemia cases are shown in Figure 3. In the term infant group (n = 20), the GA ranged from 36 to 42 weeks and %HbA ranged from 10.2 to 34% and the F:A(ßT2) ratio 2.2 to 0.4, respectively. In the premature infant group (GA: 23–34 weeks), the %HbA ranged from 1.9 to 10.2 and the F:A(ßT2) ratio 5.6 to 1.6, respectively. The six cases of ß-thalassaemia all had %HbA results <1.5% and F:A(ßT2) ratios >10.
Relationship between %HbA measured by HPLC and HbF:A(ßT2) in a series of bloodspot samples. The dotted lines represent the %HbA action value of 1.5% and the 99.9th centile value for the F:A(ßT2) ratio of 3.6.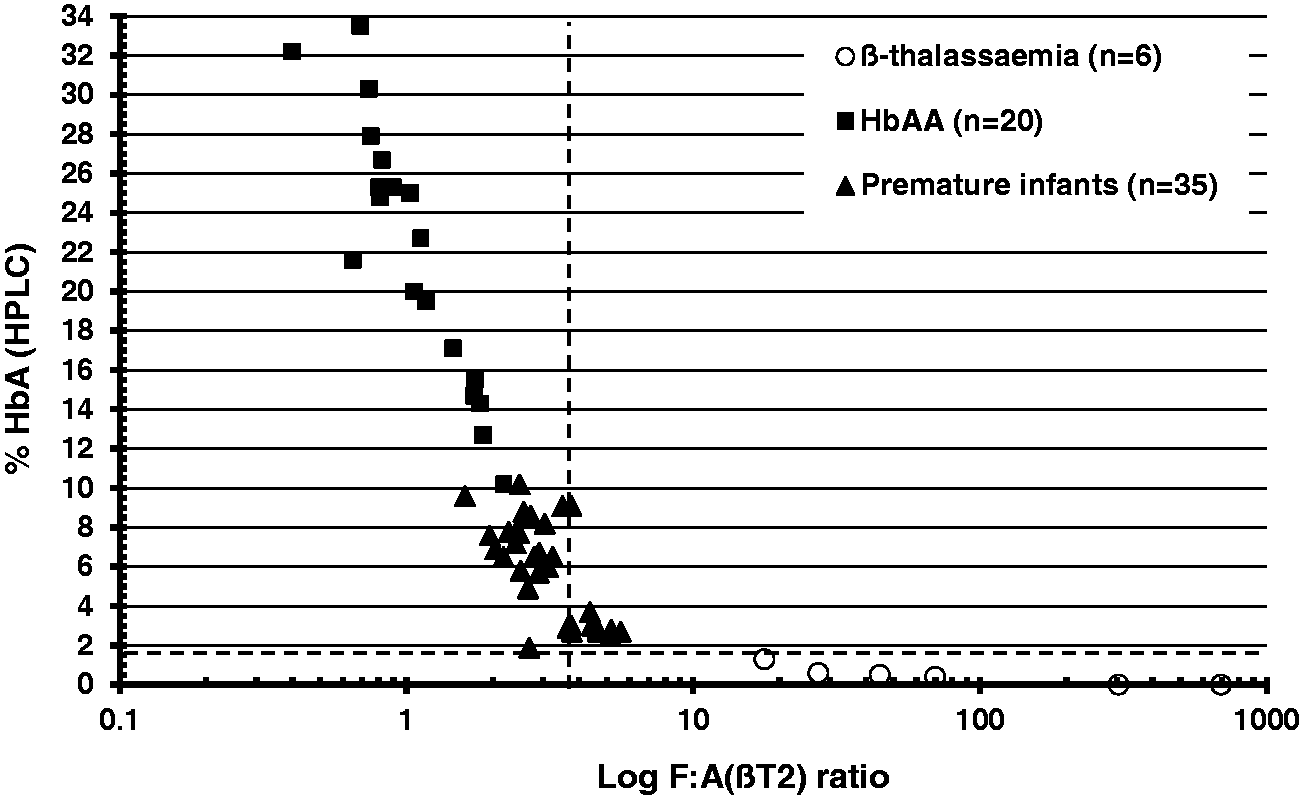
Assessment of Hb peptides by MS/MS to detect samples from older infants
Data from a total of 354 routine samples from older infants aged one month to one year received into the Wales Newborn Screening Laboratory were analysed to construct graphs on the expected HbA and HbF ratios (Figure 4).
Relationship between HbA(ßT1):F ratio (a) and HbF:A(ßT2) (b) with age (days after birth) in older non-transfused babies (n = 354) age one month to one year.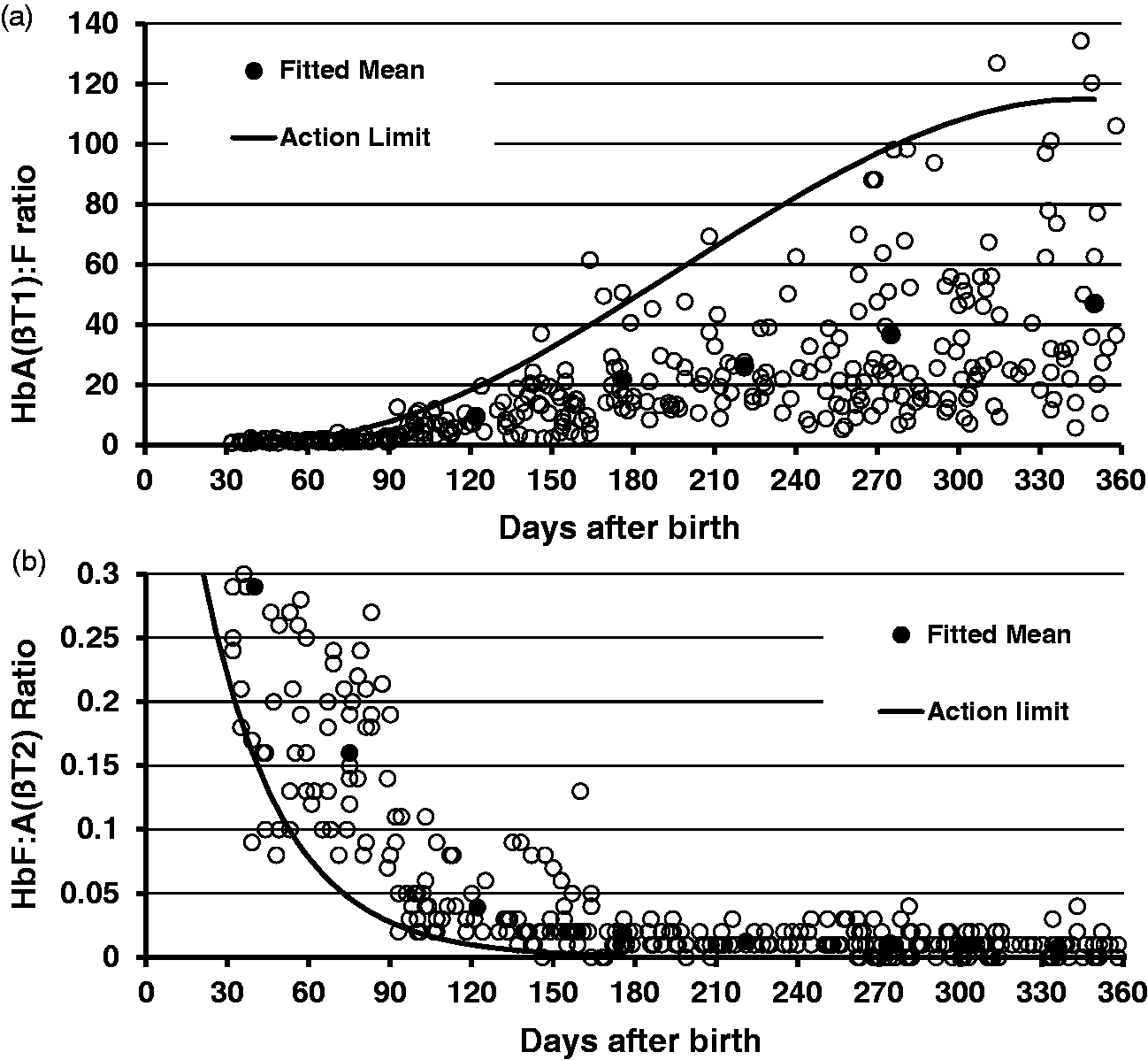
Discussion
We screened a total of 100,456 infants during a three-year period using our MS/MS protocol, which was designed to detect only the disease states of SCD. The birth prevalence of 1:10,000 in Wales is similar to other low prevalence areas in the UK. 9 The use of our protocol prevented large numbers of carrier infants being identified as by-products. On the basis of six months data, it is estimated that this protocol prevented the identification and referral of 810 carrier infants during the three-year period.
The screening action values developed in our original validation study were generated using a single MS/MS instrument (Waters Xevo-TQ). In order to ensure resilience for the screening service, further validation work was undertaken to assess the transferability of the screening action values onto an additional MS/MS instrument (Waters Xevo-TQS). The routine analysis of the Hb peptide ratios was reproducible on both MS/MS platforms, with intra- and inter-assay CVs similar to those reported previously.2,4 Both MS/MS instruments used were able to detect HbS peptides in bloodspots at concentrations <1% of the total Hb present.
The SpOtOn Diagnostics Kit contains an HbS stable isotope internal standard, which acts as a control for the digestion step needed to release the Hb fragments and to monitor changes in the MS/MS instrument response. Due to differences in the abundance observed between the MS/MS systems, individual laboratories must establish assay/sample rejection limits for each instrument. Differences in the peptide abundances and some of the Hb variant to wild-type peptide ratios between the two MS/MS instruments were observed. However, the HbS, C, E, OArab and Lepore variant to wild-type peptide ratios generated on both MS/MS systems were able to distinguish between the normal, heterozygous and homozygous states. The ability of the D:A ratio to distinguish between normals and DPunjab carriers was less well resolved.
Excellent agreement was demonstrated between the two MS/MS systems for the S:A ratios obtained using bloodspot samples from the HbS carrier infants and infants with HbS/S, S/C, S/HPFH and HbS/β-thalassaemia (Figure 1). The consistency of the S:A ratio across various MS/MS platforms has previously been reported. 10 The high sensitivity and specificity of this assay for the HbS peptide enabled us to develop action values for the S:A ratio, and these were pivotal to our protocol to identify only the disease states of SCD. The S:A ratios in the normal Hb infant group were all <0.05 and the lowest ratio observed in HbS carrier infant group was 0.4. The lower S:A ratio action value in our protocol was set at 0.1 to identify the presence of HbS peptide in bloodspots. 4 The utility of this lower S:A ratio action value of 0.1 has also been reported and is recommended for use in England.10,11 An upper S:A ratio action value of ≥2.1 was used to identify the clinically relevant cases (i.e. HbS/S, S/C, S/β-thalassaemia, S/Lepore and S/HPFH). This action value of ≥2.1 was a pragmatic one and resulted in only a few false-positives cases. The majority of the clinically relevant cases (HbS/S, S/C, S/ß-thalassaemia, S/HPFH) had S:A ratios >20. We have observed four cases just above the action value of ≥2.1 (Figure 1). Two of these samples were from our original evaluation study. 4 These two samples were classified on the basis of the HPLC results where the %HbS was greater than the %HbA; however, the final outcome of these two cases is unknown. The lowest S:A ratio observed in the 20 HbS/S cases was 3.8 on the TQ-MS/MS and 3.7 on the TQS-MS/MS. Therefore, the same S:A ratio action value can be applied to both MS/MS systems (Figure 1).
The 99th centile value observed for the C:A ratio for the normal Hb infant group was comparable on both MS/MS systems. In addition, the C:A ratios were also comparable in those samples from HbC carrier infants and HbS/C infants when analysed both by instruments. The C:A ratio action value of 0.5 used is pragmatic. This value is based on the fact that the 99.9th centile of normal Hb infant group was 0.3 and the lowest ratio observed in the HbC carrier group was 1.27 (TQ-MS/MS) and 1.12 (TQS-MS/MS) and the lowest C:A ratio in the HbS/C cases (n = 28) was 22 (TQ-MS/MS) and 37 (TQS-MS/MS). In practice, the HbS/C cases have S:A ratios that are similar on both instruments (S:A > 15) and would be identified by the first-line action value (S:A ≥ 2.1). It should be noted that infants with HbCC and HbC/ßthalassaemia will also be detected as by-products of this screening protocol due to the low/absent ßT1 peptide. Both the HbS and C mutation are located in this peptide which results in a falsely elevated S:A ratio (≥0.1 but <2.1) and a raised C:A ratio.
The 99th centile value for the E:A ratio in the normal Hb group was comparable on both instruments. The 99.9th centile value was 0.06 and the action value used to detect HbE was set above this at ≥0.1. Therefore, the differences in the lowest E:A ratios observed in the HbE carrier group between the two instruments (1.13 vs. 1.77) are clinically irrelevant. Differences were observed between the two instruments for the O:A ratio in the normal Hb group, with the 99th centile value of 0.05 on the TQ-MS/MS and 0.16 on the TQS-MS/MS. However, ratios > 0.65 were observed for the OArab carrier samples (n = 3) on both instruments, similar to results observed in newborn bloodspot samples, 10 and our action value was set at ≥0.2 on both instruments. Comparable 99th centile values for the Lepore:A ratio (≤0.02) were observed in the normal Hb infant group and our action value was set at ≥0.04, with observed ratios >0.1 in Lepore carrier samples (n = 2).
Differences were observed between the MS/MS instruments for the D:A ratios in the samples from the normal Hb infant group. The 99th centile on TQS-MS/MS was 1.58 compared with 0.91 on the TQ-MS/MS. However, the lowest ratios observed in the Hb DPunjab carrier group were comparable (1.35 vs. 1.26) on both instruments. Due to the large number of samples analysed in the normal Hb infant group, analyses were carried out over a longer period of time relative to the ratio determination for the DPunjab carriers. This finding may be secondary to an increased inter-assay variability for this specific peptide on the TQS-MS/MS instrument. One possible explanation for this is that the DPunjab mutation, which is located in the ßT13 peptide, has a mass shift of −0.5 dalton from the wild-type peptide. The resolution of this small mass difference in the bloodspot matrix may have affected the ratio determination on the different MS/MS instruments. The transitions used in this study for the D:A ratio (689 > 377) were outlined in the SpOtOn Kit protocol. During the last three years, we have identified three false-positive HbS/Dpunjab cases. In response to these findings, we re-assessed the mass transitions for this peptide. Daughter ion analysis revealed that a 501 ion was present in a greater abundance. Analysis of this new mass transition for DPunjab (689 > 501) on the MS/MS platforms revealed that the 501 ion gave greater specificity than the 377 ion. Ratios were re-calculated for these cases (0.71/0.78/0.49), which were lower than the 99th centile value of 0.9 calculated using routine screening samples. Therefore, if the (689 > 501) transitions had been used, then the three false-positive S/D cases would not have occurred. The kit manufacturer has also reviewed the mass transitions for this peptide and they now recommend the use of the 689 > 276 transition. We are currently in the process of reviewing the transitions for the DPunjab peptide on our MS/MS systems in collaboration with the manufacturer and the Sickle Cell & Thalassaemia Screening Programme.
To identify samples from infants who are premature or those who have received a blood transfusion, we generated action values for the A(ßT1):F, F:A(ßT2) and A(ßT3):F ratios. Increased A(ßT1):F and A(ßT3):F ratios indicate high amounts of HbA, which may be due to a red cell transfusion or a sample from an older infant or adult. A low ratio indicates a low amount of HbA, which could indicate prematurity or ß-thalassaemia major. The converse is true for the F:A(ßT2) ratio. The F:A(ßT2) action values of <0.23 (0.1st centile) and >3.6 (99.9th centile) are similar to those established by the English Sickle cell and Thalassaemia Screening Programme (<0.2 and >3.0), which are applicable to various MS/MS instruments. 11 Analysis of combined data from both MS/MS instruments gave a mean F:A(ßT2) ratio of 0.86, 0.1st centile of 0.17, 1st centile of 0.24, 99.5th of 3.0 and a 99.9th of 3.8.
Considerable overlap in the F:A(ßT2) and the A:F(ßT1&3) ratios were observed between those samples from the transfused and the non-transfused infants, and this finding is similar to that using existing technologies for Hb variant analysis. Implementing such a protocol to assess transfusion status and prematurity will result in the detection of cases of ß-thalassaemia major/intermedia (increased F:A(ßT2) ratio) and HbE/ß-thalassaemia (low A(ßT3):F ratio) as clinically relevant ‘by-products’ similar to the existing methods utilized for screening. The graphs showing the percentile data for the various ratios vs. gestational age (22 to 42 weeks) provide guidance on the expected ratios in non-transfused infants (Figure 2). These action values are used routinely in our laboratory, and those samples with a decreased F:A(ßT2) ratio and an increased A(ßT1):F ratio are referred for HbS mutation analysis. All babies up to the age of one year should be offered screening if they have not been offered screening as a newborn or have recently moved into the UK. However, older infants have increased amounts of HbA relative to HbF. The graphs shown in Figure 4 provide guidance on the expected ratios up to one year of age and should prevent unnecessary referral of samples for DNA analysis.
The use of the screening action value of %HbA ≤1.5 by HPLC has been shown to be a reliable test to identify cases of ß-thalassaemia in the newborn period and has a positive predictive value of 95% in those infants born >32 weeks’ gestation. 8 From our experience, samples with an increased F:A(ßT2) ratio should be evaluated in the context of the GA of the infant, and the samples with a ratio above the appropriate 99th centile action values should be referred for second-line testing to exclude ß-thalassaemia. However, in view of the issues of interpreting results in premature babies, it is recommended that all samples from premature infants (GA ≤ 32 weeks) with an F:A(ßT2) ratio ≥4.5 (99th centile value at 32 weeks) require further investigation to exclude ß-thalassaemia. Further work is required to validate these action values for this ratio using genetically confirmed cases of ß-thalassaemia and by monitoring the screening population centiles.
Despite some of the biases observed between the two instruments, the use of appropriate action values should prevent false negatives and result in minimal false-positive cases being identified. The production of synthetic stable isotope internal standards for the various Hb peptides is required to allow standardization of all Hb peptides across MS/MS instruments.
MS/MS is both sensitive and specific for the detection of the clinically relevant Hb peptides, and the use of MS/MS as an alternative screening technology optimizes the use of equipment and expertise that currently exist in newborn screening laboratories.
Footnotes
Acknowledgements
We would like to thank the staff working in the Newborn Screening Laboratories (Wales and Great Ormond Street Hospital) and the Cardiff Haemoglobinopathy Laboratory for their assistance. We would also thank Dr Yvonne Daniel and Joan Henthorn for advice and helpful discussion of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
SJM.
Contributorship
SJM performed the data analysis, researched the literature and wrote the first draft of the manuscript. All authors contributed to the data interpretation, review and approval of the manuscript.