
Abstract
Background
The National Institute for Health and Care Excellence (NICE) published NG12 in 2015. The referral criteria for suspected colorectal cancer (CRC) caused controversy, because tests for occult blood in faeces were recommended. Faecal immunochemical tests for haemoglobin (FIT), which estimate faecal haemoglobin concentrations (f-Hb), might more than fulfil the intentions. Our aim was to compare the utility of f-Hb as the initial investigation with the NICE NG12 symptom-based guidelines.
Methods
Data from three studies were included. Patients had sex, age, symptoms, f-Hb and colonoscopy and histology data recorded. Sensitivity, specificity, positive (PPV) and negative predictive value (NPV) of f-Hb and NG12 were calculated for all significant colorectal disease (SCD: CRC, higher risk adenoma and inflammatory bowel disease). Overall diagnostic accuracy was also estimated by the area under the receiver operating characteristic curve (AUC).
Results
A total of 1514 patients were included. At a cut-off of ≥10 µg Hb/g faeces, the sensitivity of f-Hb for CRC was 93.3% (95% confidence interval (CI): 80.7–98.3) with NPV of 99.7% (95%CI: 99.2–99.9). The sensitivity and NPV for SCD were 63.2% (95%CI: 56.6–69.4) and 96.0% (95%CI: 91.4–94.4), respectively. The NG12 sensitivity and NPV for SCD were 58.4% (95%CI: 51.8–64.8) and 87.6% (95%CI: 85.0–89.8), respectively. The AUC for CRC was 0.85 (95% CI: 0.87–0.90) for f-Hb versus 0.65 (95%CI: 0.58–0.73) for NG12 (P < 0.005). For SCD, the AUC was 0.73 (95%CI: 0.69–0.77) for f-Hb versus 0.56 (95%CI: 0.52–0.60) for NG12 (P < 0.0005).
Conclusion
f-Hb provides a good rule-out test for SCD and has significantly higher overall diagnostic accuracy than NG12.
Keywords
Introduction
Summary of NICE NG12 guidelines for suspected gastrointestinal cancer and number of study participants fulfilling the individual criteria for referral.
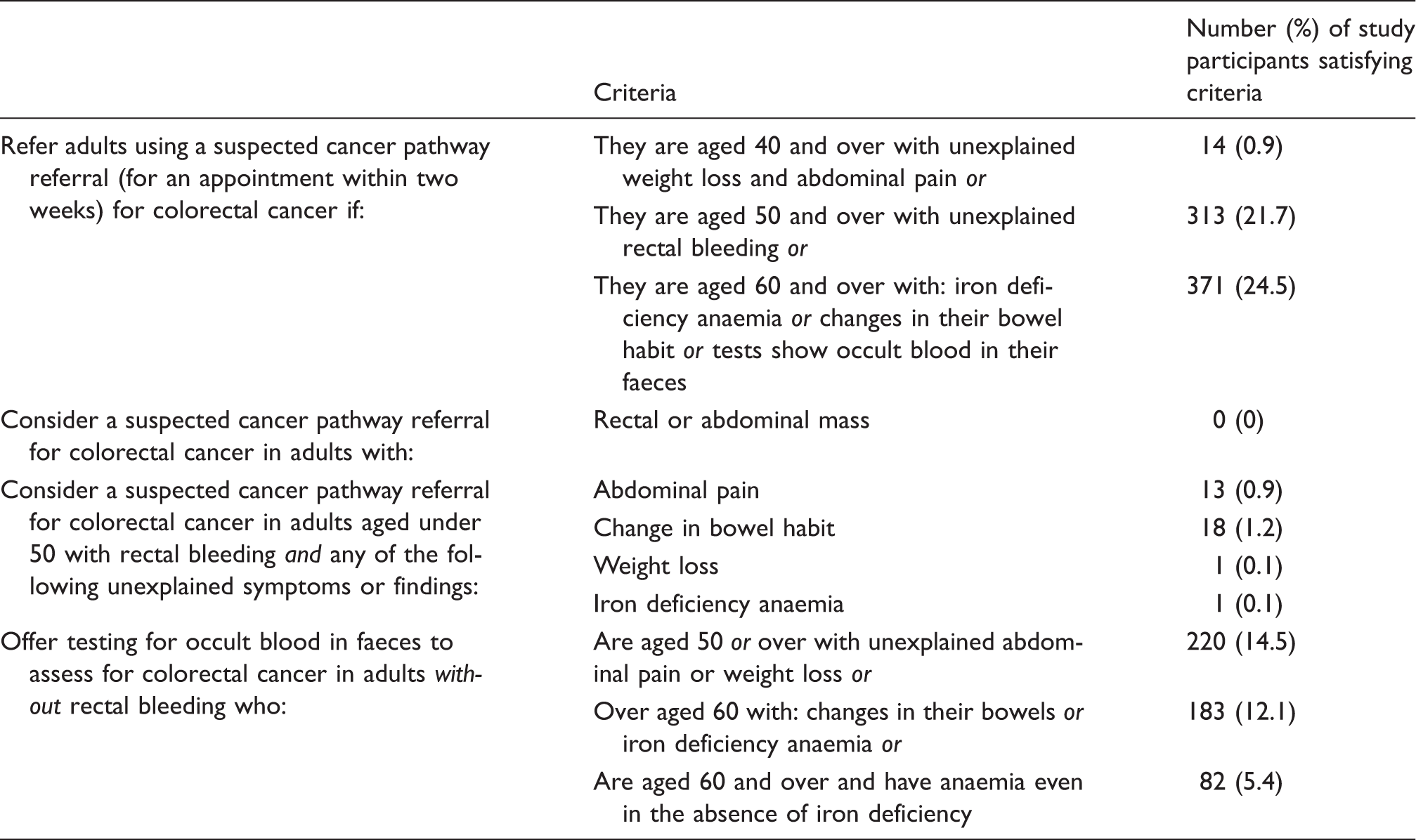
NICE published NG12 in June 2015. 5 These guidelines caused much controversy when published in both draft and final formats. In particular, the recommendation of a ‘test for occult blood in faeces’, which was initially interpreted by most as a recommendation for the traditional guaiac-based faecal occult blood test (gFOBT), was very controversial and became the subject of some concern and debate.9–11 Previously published authoritative guidelines from NICE, the Scottish Intercollegiate Guidelines Network (SIGN) and the British Society of Gastroenterology did state that there was no role for such gFOBT in assessment of patients presenting in primary care with lower GI symptoms, or in the investigation of iron deficiency anaemia. 12 In consequence, gFOBT were eliminated from the repertoires of many laboratories and its use in clinical settings other than screening very much discouraged. 12 Indeed, NICE did note that the new 2015 NG12 recommendation to test for occult blood in faeces in patients at low risk of CRC would necessitate a change in practice, because such tests were not currently available. 5 However, realization quickly grew that faecal immunochemical tests for haemoglobin (FIT), which are able to quantitate faecal haemoglobin concentrations (f-Hb), could well more than fulfil the intentions of NG12. 10 It was recognized by NICE that some evidence did exist to suggest that FIT might have applicability in triaging patients presenting in primary care. 9 FIT, a newer type of test for the detection of occult blood in faeces, use antibodies specific to human haemoglobin. They have been developed as a significant improvement on gFOBT, which are based on the pseudo-peroxidase activity of the haem component of haemoglobin and produce a blue colour change on the test card if positive. Sometimes, this colour change occurs because of moieties with peroxidase activity in the diet, or with medicines being taken, leading to false-positive test results. Because FIT are designed to specifically detect human haemoglobin, they do not suffer from interference from dietary constituents. Moreover, FIT target the globin component of haemoglobin, which degrades as it travels through the GI tract; hence, FIT are less likely to detect globin from upper GI bleeding. 13 In addition, FIT are analytically much more sensitive than gFOBT and so detect smaller amounts of blood in faeces.
There is now significant evidence that FIT do have applicability as the initial approach to the assessment of symptomatic patients presenting in primary care, including those who warrant urgent referral. It has been shown that the use of f-Hb performs better than previous high-risk symptom-based strategies from NICE and SIGN for fast-tracking suspected CRC referrals.6,12,14–19 Moreover, and most importantly, f-Hb with very low cut-off concentration has very high NPV for the detection of SCD in this clinical setting. 10 In consequence, a ‘negative’ test result provides considerable reassurance that referral for colonoscopy is not required urgently or even at all. There is no doubt that f-Hb measurements have considerable potential to contribute to reducing unnecessary colonoscopy for the majority of symptomatic patients. However, the question remains of whether f-Hb, a laboratory-based investigation, is better than the recent NG12 symptom-based referral guidelines as the initial approach in primary care to rule in CRC (the purpose of NG12) or rule out SCD. We did not aim to examine the diagnostic accuracy of the groups detailed in NG12 as shown in Table 1 since this was comprehensively documented in the guideline. 5 The aim of this study was to undertake such a comparison, particularly investigating sensitivity as a measure of goodness as a rule in test and NPV as a good estimate of utility as rule-out test, for both CRC and SCD.
Methods
Data from three studies conducted in Scotland were included in our analysis; these are described in detail in the relevant peer-reviewed publications, and are summarized below.17–19 The studies, on the role of f-Hb in assessment of patients presenting in primary care with lower GI symptoms, were conducted between 2010 and 2015 and included only patients with sex, age, details of symptoms leading to referral for lower GI endoscopy, f-Hb and complete colonoscopy data with histology where applicable. The referrals were done as described in the publications and did not follow the NG12 criteria. Reasons for referral were based on symptoms including rectal bleeding, change in bowel habit, iron deficiency anaemia, abdominal pain, bloating, polyp/CRC surveillance, family history and assessment of IBD. An f-Hb of greater ≥10 µg Hb/g faeces was deemed a positive test result. The results were collated from the three study databases. Referral symptoms were reviewed and categorized as in keeping with NG12 referral criteria or not.
Study one (FITS) 17 was an investigation on diagnostic accuracy based on a consecutive series of participants; no intervention was made based on the f-Hb concentration. Patients who had been referred from primary care for endoscopic examination of the lower GI tract in NHS Tayside from February 2010 to March 2012 were invited by a colorectal specialist research nurse to participate in the study by completing a single sample faecal collection for f-Hb. The returned samples were analysed for f-Hb using one of two OC-Sensor Diana automated immunoturbidimetric analysers (Eiken Chemical Co., Ltd, Tokyo, Japan). Analyses were carried out in the Scottish Bowel Screening Centre Laboratory.
Study two (FITS2) 19 aimed to determine whether patients with lower abdominal symptoms can be investigated quickly using results of f-Hb and whether this investigation could form part of a diagnostic pathway for SCD. Participants referred from primary care for colonoscopy in NHS Lanarkshire from June 2013 to December 2013 inclusive were recruited by sending one faecal specimen collection device with the appointment for endoscopy and the bowel cleansing materials. The returned samples were analysed for f-Hb using one HM-JACKarc analyser (Kyowa-Medex Co., Ltd, Tokyo, Japan).
Study three (FITS+) 18 assessed the diagnostic accuracies of quantitative f-Hb and faecal calprotectin tests in patients presenting to primary care with lower GI symptoms who were then referred for investigation. All adult patients referred in NHS Tayside over a six-month period from October 2013 to March 2014 were eligible. Estimates of f-Hb were generated using one OC-Sensor IO analyser (Eiken Chemical Co., Ltd, Tokyo, Japan).
Statistical analysis
To determine the differences in clinical performance between f-Hb and NG12 referral criteria as an initial investigation, we performed the following analyses. Sensitivity, specificity, PPV and NPV (all with 95%CI) were calculated using a cut-off of ≥10 µg Hb/g faeces for CRC, HRA, advanced neoplasia (AN = CRC plus HRA), IBD and SCD. Receiver operating characteristic (ROC) curves for CRC and SCD were constructed and the area under the curve (AUC), with 95%CI, was determined as a simple easy to understand estimate of overall diagnostic accuracy. AUC were calculated overall and separately for the three analytical systems used, for men and women and for those aged <50 years and ≥50 years. AUC were compared using VassarStats: Website for Statistical Computation (http://vassarstats.net/roc_comp.html). Associations between categorical variables were examined using chi-squared tests for linear trend unless otherwise specified. A P-value of <0.05 was considered statistically significant. Statistical analyses were performed using SPSS software (SPSS Inc., Chicago, IL, USA).
Results
Patient population
A total of 1514 patients were included in our analysis. Patient sex and age, two variables proven to affect f-Hb, 20 presenting symptoms, f-Hb and final diagnosis following investigation were recorded in the study specific databases: 280 patients were recruited to the FITS study, 484 patients to FITS2 and 750 patients to FITS+. CRC was found in 45 patients (3.0%), HRA in 95 (6.3%), AN in 140 (9.3%), IBD in 91 (6.0%) and SCD in 231 (15.3%). The number who would be directly referred in all three studies for colonoscopy following NG12 guidelines was 731 (48.3%), and the number who would be referred for testing for occult blood in faeces was 485 (32.0%). The criterion used for a positive outcome from f-Hb in those who would have been referred for testing for occult blood using NG12 was f-Hb ≥10 µg Hb/g faeces. A total of 1216 (79.7%) would have a further action taken as a result of the NICE NG12 guidelines. No gFOBT was done on the last three groups in Table 1 in any of the three studies because the patient had been referred for endoscopy based solely on a priori clinical assessment in primary care, and gFOBT were unavailable in both NHS Tayside and NHS Lanarkshire.
Comparison of the three FIT analytical systems
Comparison of overall diagnostic accuracy assessed by the area under the receiver operating characteristic curve, with 95% CI, for faecal haemoglobin concentration, overall, and by FIT analyser and study, and for the NICE NG12 guidelines for colorectal cancer.
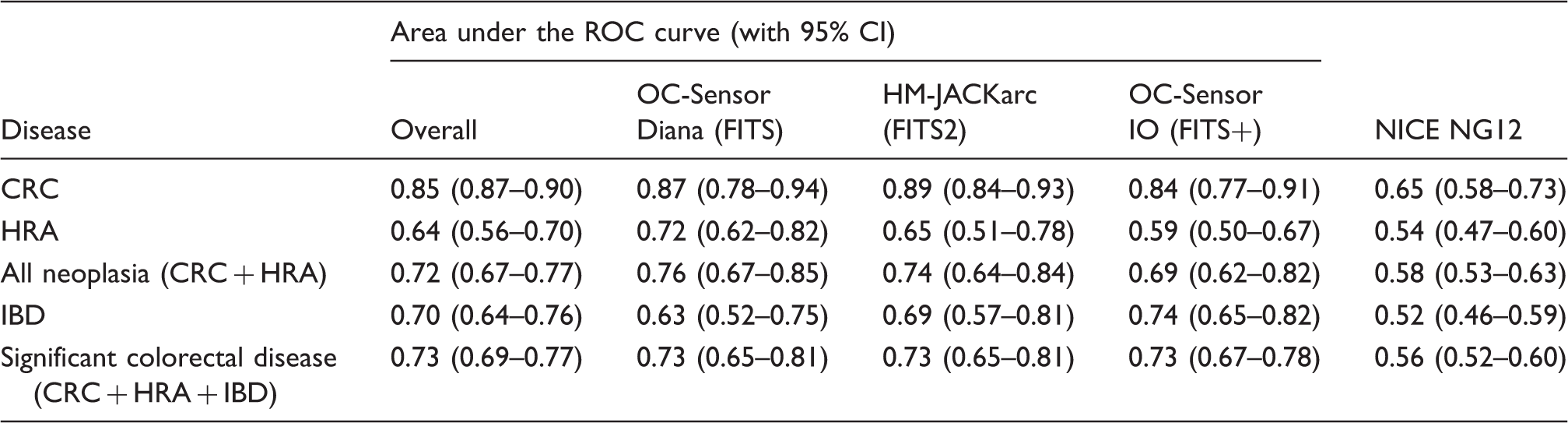
CRC: colorectal cancer; HRA: higher risk adenoma; IBD: inflammatory bowel disease; ROC: receiver operating characteristic.
Clinical characteristics of f-Hb
Sensitivity, specificity, positive predictive value, negative predictive value, as percentages, and area under the ROC curve, with 95% CI, of faecal haemoglobin concentration overall and by sex and age, using a cut-off of ≥10 µg Hb/g faeces.
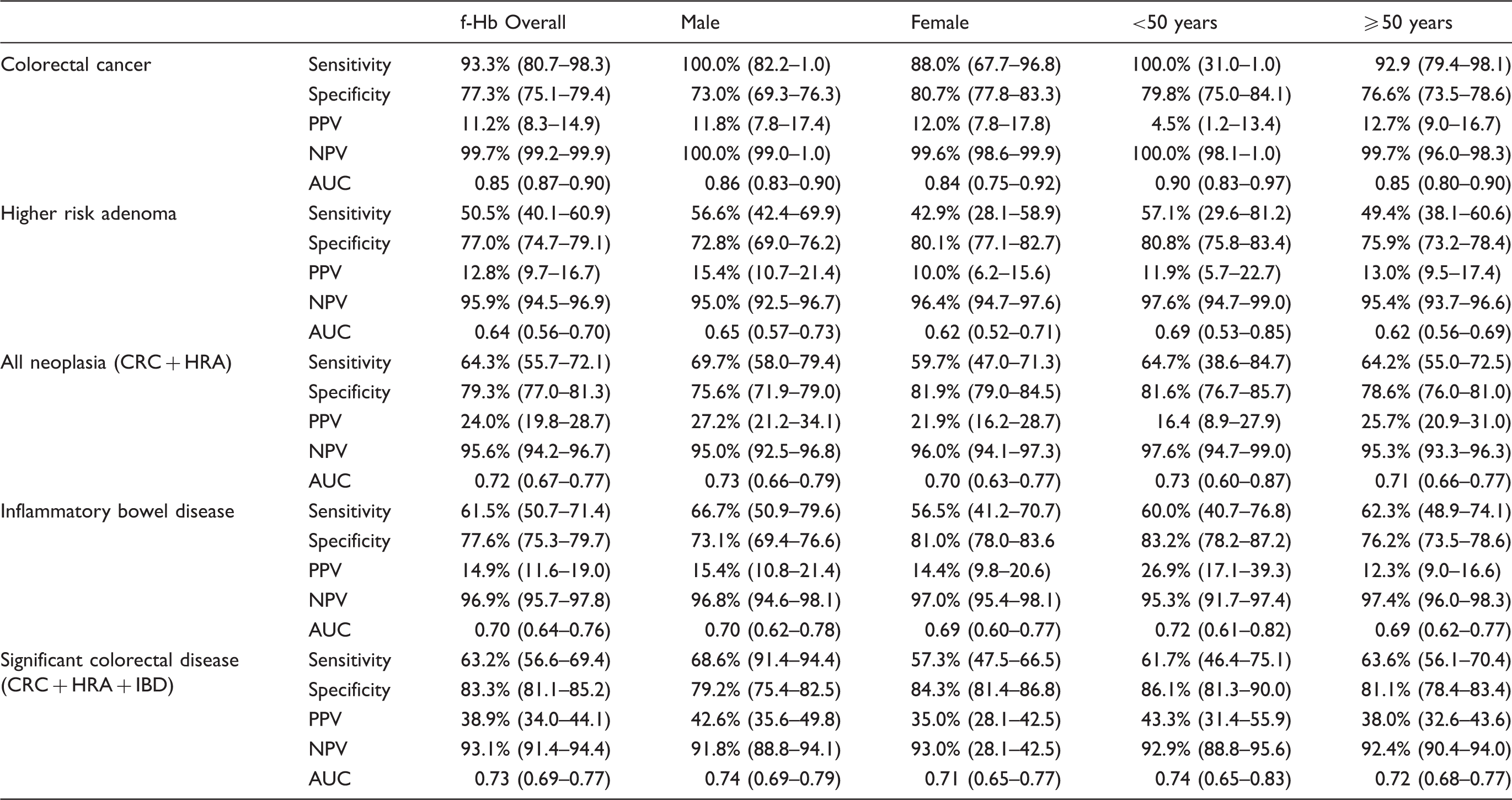
PPV: positive predictive value; NPV: negative predictive value; AUC: area under the ROC curve; f-Hb: faecal haemoglobin; CRC: colorectal cancer; HRA: higher risk adenoma; IBD: inflammatory bowel disease.
Clinical characteristics of f-Hb by sex
Differences were observed in sensitivity, specificity, PPV and NPV between men and women, although the AUC was not significantly different in CRC, HRA, AN, IBD or SCD between the two groups (Table 3; P > 0.05). Sensitivity for CRC, HRA, AN, IBD and SCD was higher in men than women and specificity lower. NPV was similar between men and women for CRC, HRA, AN, IBD and SCD.
Clinical characteristics of f-Hb by age
In those aged less than 50 years, the sensitivity for detecting CRC, HRA, AN, IBD and SCD was higher than in those older than 50 years. The NPV for CRC, HRA, AN, IBD and SCD were 100.0% (95%CI: 98.1–1.0), 97.6% (95%CI: 94.7–99.0), 97.6% (95%CI: 94.7–99.0), 95.3% (95%CI: 91.7–97.4) and 92.9% (95%CI: 88.8–95.6), respectively, in those less than 50 years compared with 99.7% (95%CI: 96.0–98.3), 95.4% (95%CI: 93.7–96.6), 95.3% (95%CI: 93.3–96.3), 97.4% (95%CI: 96.0–98.3) and 92.4% (95%CI: 90.4–94.0), respectively, in those aged older than 50 years. The AUC for f-Hb was not significantly different for CRC, HRA, AN, IBD and SCD in those participants less than 50 years of age and in those equal to or older than 50 years (Table 3; P > 0.05).
Overall diagnostic accuracy of f-Hb and NG12 compared
Overall, f-Hb had statistically significantly higher diagnostic accuracy than NG12 for all of CRC, HRA, AN, IBD and SCD (P < 0.0005) as shown in Table 3. For both CRC and SCD, the AUC was significantly higher for f-Hb than NG12 (P < 0.0005).
Number of cases missed using f-Hb and NG12
Number of patients with colorectal diseases missed using faecal haemoglobin concentration at ≥10 µg Hb/g faeces cut-off and number missed using NICE NG12 guidelines.
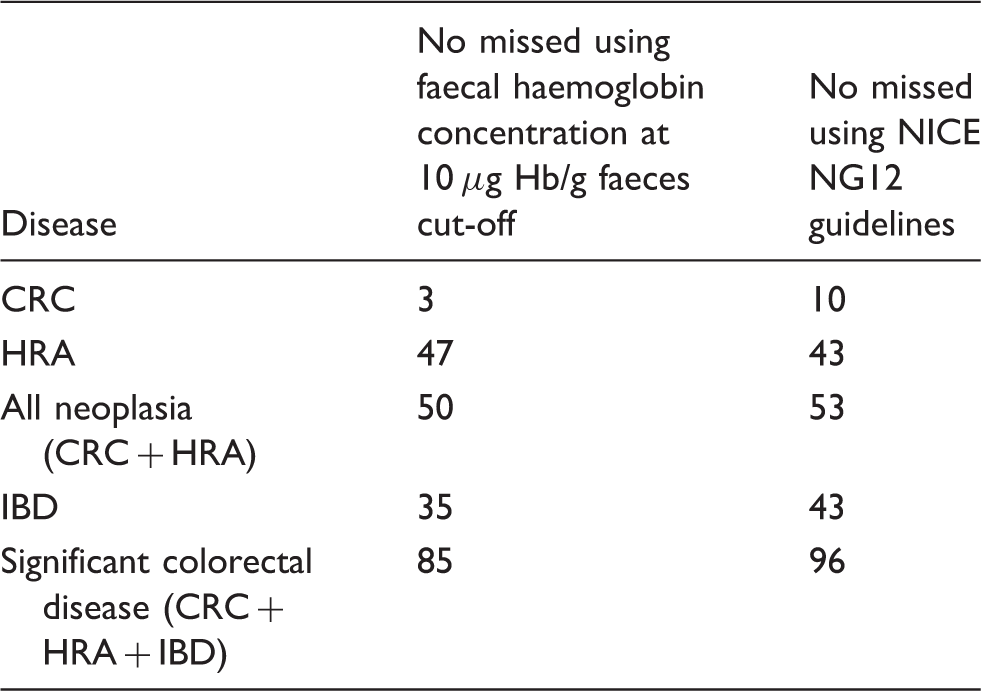
CRC: colorectal cancer; HRA: higher risk adenoma; IBD: inflammatory bowel disease.
Discussion
NG12 uses the terminology ‘a test for occult blood in faeces’ and this could be interpreted as gFOBT or FIT: no studies such as ours have investigated gFOBT, an obsolete investigation, 12 and no patient in any of the three studies from which data were obtained had gFOBT performed. Most importantly, the high NPV of f-Hb for all SCD confirm the high utility of f-Hb as a rule-out test. In addition, the results demonstrate that f-Hb with a cut-off for referral of ≥10 µg Hb/g faeces, a laboratory-based investigation, has significantly higher overall diagnostic accuracy than the symptom-based NICE NG12 guidelines and would therefore be more reliable as an indication for referral for further investigation than NG12. The results add to the growing body of evidence supporting the use of FIT as the first-line investigation in in the assessment of patients presenting in primary (and secondary) care with lower GI symptoms, as recently argued. 21
There are now several studies including a meta-analysis that have evaluated the diagnostic performance of FIT in symptomatic and high-risk populations, suggesting high sensitivity and specificity for CRC.3,7 A Spanish study of 787 patients referred for colonoscopy showed that FIT was more accurate in detecting CRC than the previous 2011 NICE or the SIGN referral criteria. 6 Similar to the results observed in this study, they demonstrated that, in a high-risk population, using a f-Hb cut-off of ≥20 µg Hb/g faeces, 20% fewer colonoscopies would have been required to detect 42% more CRC. A further study done in a different region of Spain confirmed these results: NICE and SIGN guidelines detected 46.7% and 43.3% of cases of CRC, while f-Hb ≥15 μg Hb/g faeces detected 96.7% of cases. 16 In other studies investigating the use of f-Hb for detection of CRC in symptomatic patients, sensitivity has ranged from 67% to 100% and specificity from 71% to 93% dependent on the f-Hb cut-off used.6,15,17–19 As in this study, inspection of the NPV in particular demonstrates that the results of these studies provide telling evidence that the f-Hb has the potential to be a good rule-out test for SCD and could therefore reduce the number of unnecessary referrals for colonoscopy, easing the pressure on already over-subscribed services. To allow comparison between studies, we used ≥10 µg Hb/g faeces as the f-Hb cut-off, exactly in keeping with latest draft NICE guideline in development (GID-DG10005) on quantitative FIT to assess symptomatic people who are at low risk of CRC in primary care. 22
Limited data are available on the diagnostic accuracy of f-Hb for non-neoplastic SCD, particularly IBD. We have previously demonstrated that, in a population of symptomatic patients referred for endoscopy from primary care, CRC, HRA and IBD had significantly higher median f-Hb than those with less clinically important findings. 17 Using a cut-off of ≥10 µg Hb/g faeces, the current study has demonstrated a sensitivity, specificity and PPV and NPV of f-Hb for CRC of 93.3% (95%CI: 80.7–98.3), 77.3 (95%CI: 75.1–79.4), 11.2% (95%CI: 8.3–14.9) and 99.7% (95%CI: 99.2–99.9), respectively. In all, 1283 (84.7%) of our patient cohort had non-significant colonic findings – normal bowel (933 patients; 61.6%), and less significant pathology such as haemorrhoids, hyperplastic polyps and simple diverticular disease (397 patients; 26.2%). Using f-Hb as a triage investigation in this cohort would potentially have avoided a referral and subsequent invasive investigations in the 82.2% of patients without serious pathology. NG12 is concerned with the detection of lower GI cancer and therefore does not have such a broad clinical aim as the published concepts from Scotland on the application of f-Hb. As expected, f-Hb missed overall fewer cases of AN, IBD and SCD. However, in spite of missing some cases, the high NPV demonstrates that this approach of investigating all patients with lower GI symptoms with an initial f-Hb is most appropriate for use as a rule-out test for SCD, but with robust safety-netting procedures in place. This interpretation is in agreement with previous studies utilizing FIT for assessment of symptomatic populations.2,18,19
We observed that 229 patients (15.1%) who had f-Hb ≥10 µg Hb/g faeces had no significant pathology as compared with 603 (40.0%) patients referred following NG12 guidelines. The concern from clinical specialists that using f-Hb in primary care to triage suspected CRC referrals could result in unnecessary colonoscopy referrals is not confirmed by this study. In addition, the number of false-positive test results that occur when using f-Hb to diagnose CRC, as shown by the PPV, would be partially offset by detecting other important and treatable bowel diseases, particularly HRA and IBD. Positive FIT should be viewed as a marker of potential SCD, irrespective of symptoms.
The strengths of this study include the large sample size, with 1514 patients providing age, sex, complete symptom data, as well as f-Hb and final diagnoses. In addition, the unselected nature of the patients referred from primary care increases the applicability of the findings to those working to identify cases of SCD in primary and secondary care. A limitation of our study is that the location of the CRC and HRA was not recorded and therefore cannot be assessed in terms of predictive value of disease detection. This will be very interesting to study further if f-Hb is rolled out into routine clinical practice, as will studies on the health economic benefits of introducing this test and potential cost-savings through reduction in referrals and number of colonoscopic (and possibly imaging) procedures undertaken. A further limitation is that it might be considered invalid to evaluate referral criteria in referred patients only. The NG12 guidelines were unavailable when these studies were done: interestingly, the Scottish referral guidelines for suspected cancer 23 are much less prescriptive than NG12, but f-Hb is now seen to have significant potential as the first-line investigation in assessment of patients presenting in primary care with lower abdominal sysmptoms. 24
In conclusion, we have demonstrated that, in the primary care setting, the reliability of f-Hb to rule-out most SCD is high and we believe that our results are widely applicable. In addition, f-Hb has significantly higher overall diagnostic accuracy than NG12 referral criteria for CRC detection. Although we do not have any data on the acceptability of FIT to patients presenting in primary care with lower GI symptoms, the need for only one faecal sample, collected in an easy to use, hygienic device, should encourage completion of the test.
Footnotes
Acknowledgements
All those who assisted us in the FITS, FITS2 and FITS+ studies are acknowledged in the relevant papers on the studies.
Declaration of conflicting interests
CGF has undertaken consultancy with Immunostics Inc., Ocean, NJ, USA, and Kyowa-Medex Co., Ltd, Tokyo, Japan, and received assistance for travel and attendance at meetings from Alpha Labs Ltd, Eastleigh, Hants, UK.
Funding
JD is supported by a grant from the Chief Scientist Office.
Ethical approval
The FITS study was approved by Tayside Research Ethics Committee, the FITS2 study by the West of Scotland ethics service and the FITS+ study by the East of Scotland REC.
Guarantor
CGF.
Contributorship
CGF, RJCS and AJQ conceived and planned the study. AJQ, CGF, JD and RJCS performed the data analysis. JD, RJCS, JAS, CM, PJMcD, FAC, IMG, HBY and CGF were investigators on the three component studies. AJQ and CGF prepared drafts of the manuscript. All authors contributed significantly to the writing of the paper.