
Abstract
Background
Red blood cell distribution width (RDW) and neutrophil to lymphocyte ratio (NLR) have been reported to be associated with outcomes of acute cerebral infarction. However, their prognostic value in patients with subarachnoid haemorrhage (SAH) remains largely unknown. The aim of this study was to investigate the prognostic value of RDW and NLR in SAH patients.
Methods
Medical records of adult SAH patients admitted to intensive care unit (ICU) were extracted from Multiparameter Intelligent Monitoring in Intensive Care II (MIMIC II, version 2.6), a publicly accessible ICU database. Prognostic value of RDW and NLR was analysed using logistic regression model, Kaplan-Meier curve analysis and Cox regression model.
Results
A total of 274 SAH patients were included. Patients died in hospital had significantly higher RDW and NLR. RDW and NLR were significantly associated with hospital death, with adjusted odds ratios of 1.39 (95% CI, 1.06–1.82) and 1.04 (95% CI, 1.00–1.08), respectively. Furthermore, increased RDW and NLR were associated with higher one-year mortality, with an adjusted hazard ratio of 1.20 (95% CI, 1.02–1.41) for per 1% increased RDW and 1.03 (95% CI, 1.00–1.05) for per 1 increased NLR.
Conclusion
RDW and NLR are useful indices to evaluate the outcomes of ICU admitted patients with SAH.
Keywords
Introduction
Red blood cell distribution width (RDW) is a routinely tested index to describe the size variation of red blood cells. 1 Over the past decades, RDW has been proved to be a useful index in exploring the aetiology of anaemia, especially in differentiating thalassaemia and iron deficiency-related anaemia. 2 However, recent studies revealed that RDW is useful in estimating the risk, prognosis or disease activity of non-haematologic diseases, such as cardiovascular diseases,3–7 liver diseases,8,9 autoimmune diseases10–12 or stroke. 13 In patients with acute subarachnoid haemorrhage (SAH)14,15 or acute cerebral infarction, 16 RDW was proved to be associated with short-term and functional outcome of patients. However, whether RDW is associated with long-term outcome of SAH remains unknown.
Neutrophil to lymphocyte ratio (NLR), which is defined as the ratio of neutrophils percentage to lymphocytes percentage, is an easily acquired haematological index. Similar to RDW, NLR has been revealed to be a prognostic factor for patients with acute cerebral infarction. 17 However, whether NLR can be used in evaluating the prognosis of SAH remains largely unknown.
In this study, with the use of a large clinical database named Multiparameter Intelligent Monitoring in Intensive Care II (MIMIC II, version 2.6), we investigated the prognostic value of RDW and NLR in adult patients with SAH.
Materials and methods
Summary of database
MIMIC II is a large clinical database consists of more than 30,000 patients admitted to intensive care unit (ICU). 18 All these patients were enrolled in Beth Israel Deaconess Medical Center (Boston, MA) from 2001 to 2008. This database is composed of 38 tables, which record patients’ information, such as demographics characteristics, treatment outcomes and laboratory tests. All patients in this database are de-identified to protect patients’ privacy.
After completing a training course on the website of National Institutes of Health (NIH), an author (Z-D Hu, certification number: 1678079) was approved to access the database. The accessing process was well documented by Zhang. 19
Informed consent was waived since the establishment of this database is approved by the Institutional Review Boards of the Massachusetts Institute of Technology (Cambridge, MA) and Beth Israel Deaconess Medical Center (Boston, MA).
Data extraction
Similar to our previous studies,7,20,21 data were extracted using structure query language (SQL) with pgAdmin (version 1.12.3), an open source development and administration platform for PostgreSQL. Five tables in MIMIC II database were used in our study, including ICD9, COMORBIDITY_SCORES, LABEVENTS, D_LABITEMS and ICUSTAY_DETAIL. ICD9 was used to define the patients with SAH (code = 430 and sequence = 1). D_LABITEMS and LABEVENTS were used to extract results of laboratory tests. ICUSTAY_DETAIL was used to extract age group, clinical outcomes, simplified acute physiology score (SAPS) I. 22 In MIMIC II database, adult is defined as patients more than 15 years old. As to patients received a laboratory test more than one time during their hospitalization, only the initial test results were analysed. Patients who have been previously admitted to ICU were excluded.
Statistical analysis
Continuous variables were presented as mean and standard deviation (SD) and compared by Mann-Whitney U test. Categorical variables were compared using Chi-square test. Logistic regression model, Cox regression model and Kaplan-Meier survival curve analysis were used to evaluate the prognostic value of RDW, SAPS, NLR and platelet. All statistical analyses were performed using SPSS 17.0. P value less than 0.05 was defined as statistically significant.
Results
Characteristics of subjects
Characteristics of subjects.
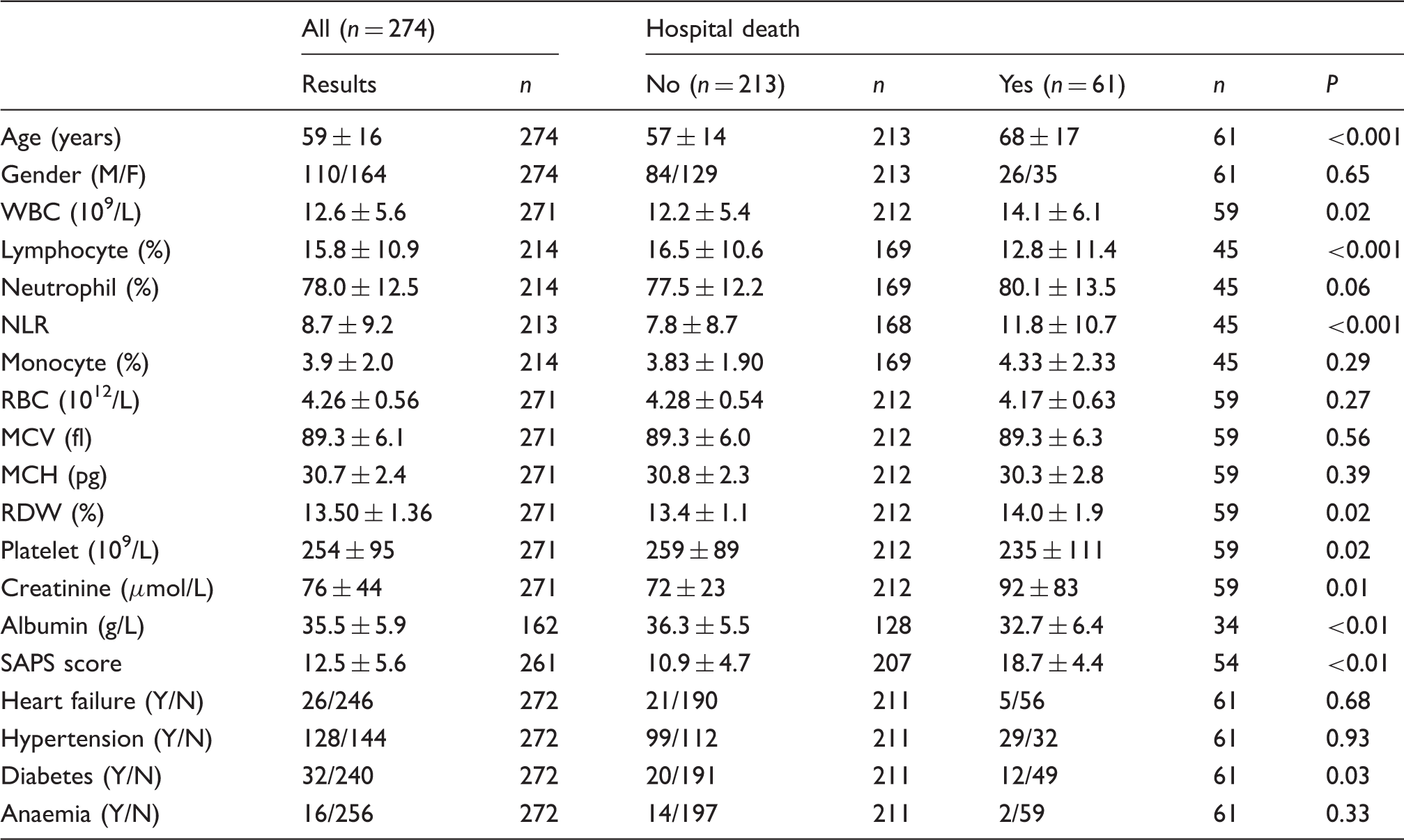
Note: Values are presented as mean and standard deviation or number of subjects, where appropriate.
WBC: white blood cell; NLR: neutrophil to lymphocyte ratio; RBC: red blood cell; MCV: mean corpuscular volume; MCH: mean corpuscular haemoglobin; RDW: red blood cell distribution width; SAPS: simplified acute physiology score.
Prognostic factors associated with hospital death
Next, we analysed the factors associated with hospital death among the subjects. We only analysed the prognostic value of RDW, NLR, SAPS and platelet in a logistic regression model. Age, WBC, renal function, comorbidities were excluded because they are included in SAPS score. The interactions between these three parameters and SAPS score may bias the estimates of the model. 23 Albumin was excluded because the results were only available in 162 subjects.
Logistic regression analysis for hospital death.
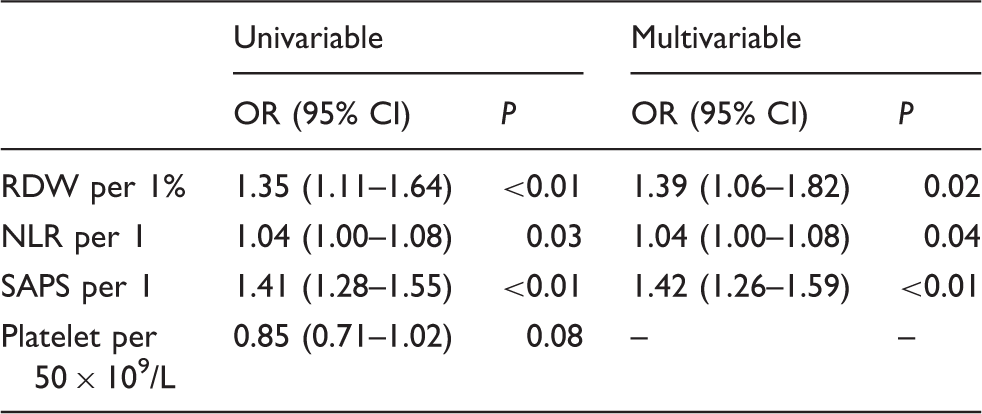
NLR: neutrophil to lymphocyte ratio; RDW: red blood cell distribution width; SAPS: simplified acute physiology score; OR: odds ratio.
Effects of RDW, NLR and SAPS on one-year mortality
Figure 1 is a Kaplan-Meier survival curve for the subjects. Figure 1(a) shows that subjects with RDW higher than 15% (upper limit of reference interval
24
) had significantly poorer outcomes. We also found that subjects with NLR higher than 6.86 (median of NLR across all subjects) had significantly poorer outcomes, as shown in Figure 1(b).
Kaplan-Meier curve analysing prognostic value of RDW (a) and NLR (b).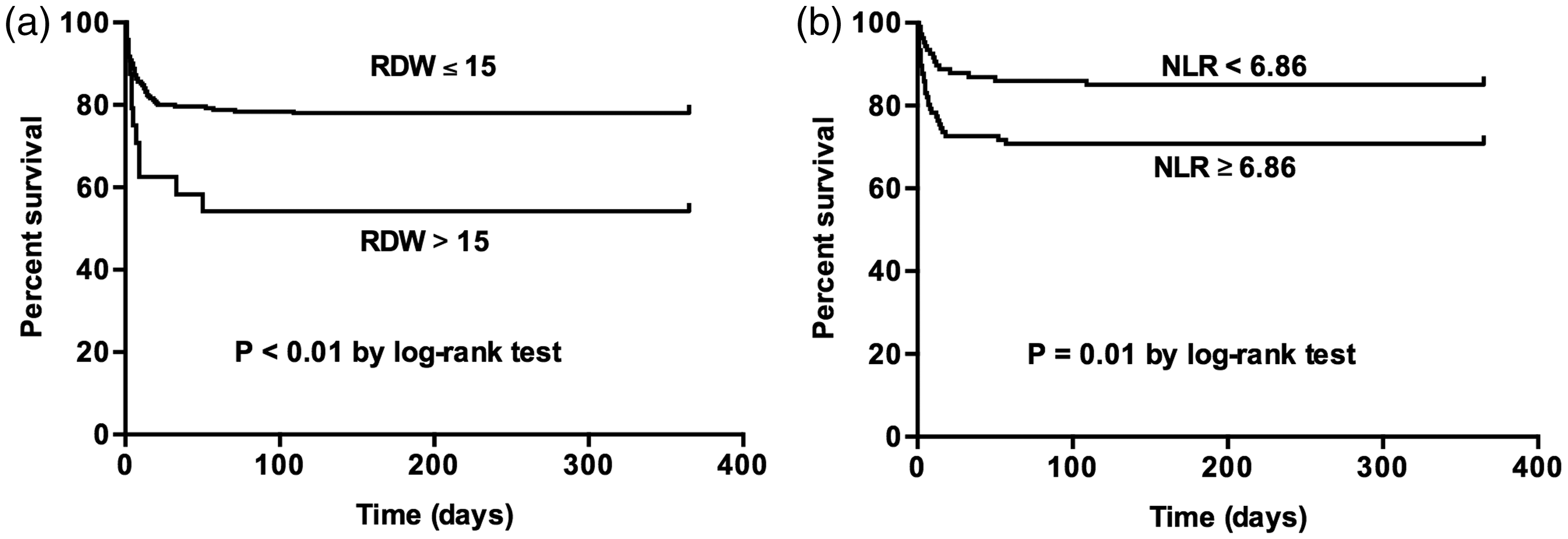
Cox regression model analysis for one-year mortality.
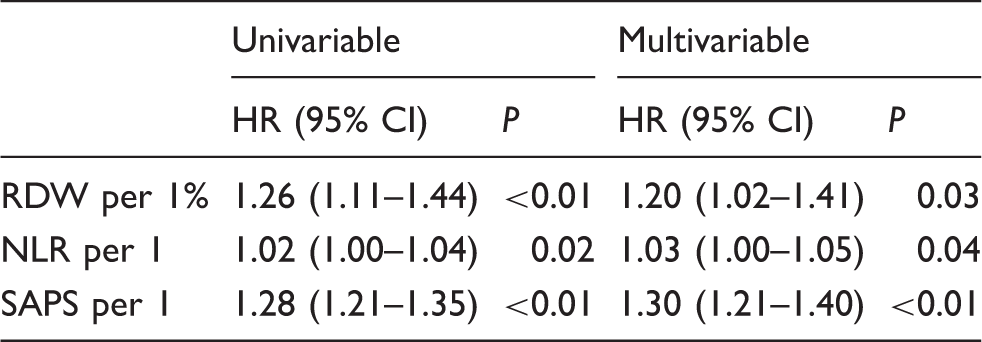
NLR: neutrophil to lymphocyte ratio; RDW: red blood cell distribution width; SAPS: simplified acute physiology score; HR: hazards ratio.
Discussion
In this study, we found that both RDW and NLR were useful indices to evaluate hospital mortality and one-year mortality in adult SAH patients admitted to ICU, and their prognostic value were independent of SAPS, a well-known score system in evaluating the outcomes of ICU patients.
Mechanisms underlying RDW, NLR and outcomes of SAH patients remain largely unknown. We hypothesized that the prognostic value of NLR and RDW are related to inflammatory response. It is well known that inflammatory response is critically involved in the pathogenesis of SAH. 25 Previous studies have found that increased inflammatory markers, such as C-reactive protein (CRP) 26 and erythrocyte sedimentation rate (ESR), 27 were associated with poor outcomes of SAH. A recent study also revealed that increased NLR is associated with poor outcomes at three months. 28 Meanwhile, RDW and NLR have been proved as inflammatory markers. For example, Lippi et al. reported that RDW is positively correlated with inflammatory markers (CRP and ESR) in a cohort of unselected outpatients. 29 In healthy individuals, a positive correlation between RDW and inflammatory markers was also observed. 30 In our previous study, we found that RDW was correlated with inflammatory markers in primary Sjogren's syndrome 10 and systemic lupus erythematous. 11 For NLR, some studies also indicated that it is an inflammatory marker.31,32 For example, NLR is positively correlated with CRP in autoimmune disease33,34 and chronic obstructive pulmonary disease (COPD). 35 Taken together, these results indicate that inflammation at least partially mediates the association between the outcomes of SAH and both RDW and NLR.
Besides inflammation response, another possible mechanism responsible for increased RDW is hypoxaemia. It is true that hypoxaemia is very common in SAH patients, 36 and a recent study found that hypoxaemia can increase RDW. 37
Prognostic evaluation is a critical step in managing SAH patients. Previous studies found that SAPS, a well-known tool in evaluating the prognosis of critical ill patients, is useful in evaluating the prognosis of SAH. 38 Since the cohort in our study was adult SAH patients admitted in ICU, it is reasonable to evaluate the prognosis of subjects using SAPS. We found that the prognostic value of NLR and RDW was independent of SAPS, indicating that RDW and NLR may provide additional value in evaluating the prognosis of SAH. Actually, RDW and NLR were prognostic factors for critical ill patients.39–43 Given that RDW and NLR were independent prognostic factors, we suggest clinicians take them into consideration when evaluating the outcomes of SAH.
To date, many novel prognostic markers for SAH have been identified, such as thrombospondin-144 and soluble CD40. 45 Compared with these markers, NLR and RDW are easily obtained and require no additional costs. In addition, compared with other inflammatory markers which are useful in evaluating the outcomes of SAH (e.g. CRP 26 ), RDW is less affected by environmental factors, such as infection. 10 Because RDW is only determined by the size variation of red blood cell, and the life span of red blood cell is approximately 130 days 46 ; therefore, RDW may reflect a long-term inflammatory status of an individual. By contrast, acute phase protein (e.g. CRP) may only reflect short-term inflammatory status of an individual, and thus has higher biological variation. Taken together, it seems that RDW is more reliable than acute phase protein in estimating the inflammatory status of SAH, and therefore may be preferred for estimating the outcomes of SAH.
Our study has two limitations. First, some clinical data, such as CRP, D-Dimer and blood pressure variability during admission, have been proved to be associated with the prognosis of SAH.47–50 However, these parameters were absent in more than half of subjects in MIMIC II database. Therefore, we cannot analyse whether the prognostic value of NLR and RDW is independent of these factors. Second, this study was performed in SAH subjects admitted to ICU; therefore, the current findings cannot be generalized non-ICU SAH patients.
In conclusion, our study indicated that both RDW and NLR were useful prognostic factors for SAH. Further studies with prospective design and more clinical details are needed to better evaluate the prognostic value of RDW and NLR in SAH patients. Besides, it is also interesting to validate our findings in non-ICU SAH patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by grants from the National Natural Science Foundation of China (No. 81302541) and Key Program of Nanjing Military Command of PLA (No. 15DX007).
Ethical approval
Not applicable.
Guarantor
Z-D H.
Contributorship
Z-DH designed research and extracted data from database; ZJH and YLH performed statistics, wrote the first draft of manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.