
Abstract
Background
In acutely ill patients with new onset hyperglycaemia, plasma glucose cannot reliably distinguish between stress hyperglycaemia and undiagnosed diabetes mellitus. We, therefore, investigated the diagnostic reliability of glycated haemoglobin (HbA1c) in acute illness by prospectively evaluating the effect of the systemic inflammatory response, as provoked by elective orthopaedic surgery, on HbA1c.
Methods
HbA1c and serum C-reactive protein concentrations were compared before and two days after elective knee or hip surgery in 30 patients without diabetes. C-reactive protein was used to assess the systemic inflammatory response.
Results
The mean (standard deviation) serum C-reactive protein increased following surgery (4.8 [7.5] vs. 179.7 [61.9] mg/L; P<0.0001). HbA1c was similar before and after surgery (39.2 [5.4] vs. 38.1 [5.1] mmol/moL, respectively; P = 0.4363).
Conclusions
HbA1c is unaffected within two days of a systemic inflammatory response as provoked by elective orthopaedic surgery. This suggests that HbA1c may be able to differentiate newly presenting type 2 diabetes mellitus from stress hyperglycaemia in acutely ill patients with new onset hyperglycaemia.
Introduction
An acutely ill patient with new onset hyperglycaemia may either have stress hyperglycaemia or it may be their first manifestation of type 2 diabetes mellitus (type 2 DM), but it is impossible to differentiate between them based on their plasma glucose concentrations.
Stress hyperglycaemia, a feature of the systemic inflammatory response (SIR), is the transient elevation of the blood glucose which resolves on recovery from the acute illness. 1 It is, therefore, retrospectively defined as an elevated fasting or random plasma glucose that returns to normal after leaving hospital. 2 Awaiting exclusion of stress hyperglycaemia may, therefore, delay the diagnosis and management of patients with type 2 DM.
Glycated haemoglobin (HbA1c) is a widely accepted diagnostic test for type 2 DM and also identifies those at high risk of developing type 2 DM. 3 The recommendations on the diagnostic use of HbA1c in acutely ill patients are conflicting,3,4 possibly because there are no prospective data on the effect of acute illness on HbA1c. We, therefore, prospectively studied the effect of the SIR, as provoked by elective orthopaedic surgery, on HbA1c.
Methods
Patients and study design
Patients undergoing elective knee or hip surgery were recruited at their preoperative assessment. Exclusion criteria included: those less 18 years, pregnant, with diabetes, difficult to bleed, with conditions known to affect HbA1c including perioperative blood transfusion within the last three months, haemoglobinopathy, stage 4 or 5 chronic kidney disease, anaemia and those with a screening fasting glucose ≥ 7.0 mmol/l and/or HbA1c ≥ 48 mmol/mol. Subjects gave written informed consent to participate in this study which was approved by the National Research Ethics Service (NRES Committee South Central – Hampshire B; study code 14/SC/1396).
Blood samples were collected into Sarstedt S-monovette sample tubes (Sarstedt, Numbrecht, Germany) on the morning of and 48 h after surgery. No patients were receiving intravenous fluids at the time of venous blood sample collection. Fluoride EDTA tubes were used for glucose; potassium EDTA tubes for HbA1c and serum gel tubes for C-reactive protein (CRP) and creatinine. Serum and plasma were separated within 2 h of collection. Haemoglobin (Hb), HbA1c and glucose were measured immediately after collection. Samples for CRP and creatinine were aliquoted and frozen at −80℃ until analysed in a single batch.
Analytical methods
HbA1c was measured in whole blood lysate by high-performance liquid chromatography on a Tosoh G7 analyser (Tosoh Bioscience Inc., San Francisco, USA). Hb was measured using flow cytometry (Sysmex XN-10®, Sysmex Corporation, Kobe, Japan). Glucose (hexokinase/glucose-6-phosphate dehydrogenase method), CRP (immunoturbidimetry) and creatinine (corrected Jaffe method) were measured using methods and reagents supplied by Abbott diagnostics on the Abbott ARCHITECT c16000 analyser (Abbott Diagnostics, Abbott Park, IL, USA). The intra-assay and inter-assay coefficients of variation (CV) are for HbA1c 0.9% and 1.2% at 21 mmol/moL (4.1%), Hb 0.8% and 1.0% at 123 g/L, CRP 0.78 % and 1.97% at 5.1 mg/L, creatinine 0.64% and 1.53% at 58 µmol/L and glucose 1.7 % and 1.0 % at 7.0 mmol/L, respectively.
Statistical analysis
The Kolmogorov-Smirnov test assessed normality of data. CRP data were non-parametric but were normally distributed following logarithmic transformation. Other data were parametric. Student’s t-test was, therefore, used to assess the significance of differences between raw parametric data or logarithmically transformed CRP data. Pearson’s linear correlation assessed the significance of association between raw or logarithmically transformed parametric variables. Data processing and statistical analyses were performed using GraphPad Instat version 3.00 for Windows 95 (GraphPad Software, San Diego, California, USA). Data (including pretransformed raw CRP data) are expressed as means with standard deviation in parentheses.
Results
Mean (SD) biochemical data in 30 patients before and 48 h after elective knee or hip surgery.
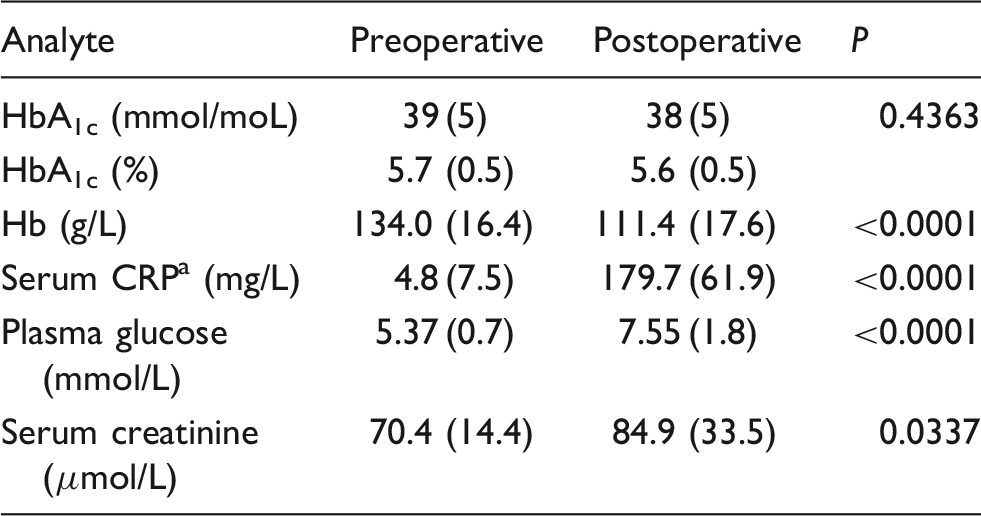
Hb: haemoglobin; CRP: C-reactive protein; HbA1c: glycated haemoglobin.
Pretransformed data shown but logarithmic data analysed.
The absolute change in CRP correlated with absolute changes in creatinine (r = 0.4389; P = 0.0152) but not with absolute changes in HbA1c (r = 0.1174, P =0.5367), Hb (r = 0.019, P = 0.9187) or glucose (r = −0.05675, P = 0.7658). There were no correlations between % change in CRP and % changes in creatinine (r = 0.2241; P = 0.2339), HbA1c (r = −0.06361, P = 0.7384), Hb (r = −0.06361, P = 0.7384) or glucose (r = −0.1796, P = 0.3424).
Discussion
The postoperative increase in serum CRP concentrations is consistent with a SIR, which was provoked solely by surgery since no patient developed postoperative infection or other acute inflammatory disease. Although plasma glucose concentrations were higher following surgery implying stress hyperglycaemia, these data must be treated with caution since although all preoperative samples were fasting, it was unclear which postoperative samples were fasting or non-fasting. HbA1c, however, was unaffected by elective orthopaedic surgery indicating that an SIR has no effect on HbA1c within two days of the surgical insult. However, the longer term effect, if any, of an SIR on HbA1c remains to be prospectively studied.
A longer term effect of acute illness on HbA1c has been investigated in an observational study by Thakker et al. 5 They evaluated intraindividual HbA1c differences in patients when attending an emergency department (ED) and after recovery from the acute illness. 5 The ED and recovery HbA1c results were highly correlated, and they concluded that HbA1c values in the emergency setting did not differ substantially from those observed on average 45 days later at outpatient follow-up5 consistent with the notion that HbA1c is unaffected by acute illness. In this study, however, the severity of illness and the presence of an SIR were not assessed.
Our study also has limitations. The lack of an effect on HbA1c by an SIR elicited by orthopaedic surgery may not be applicable to an SIR triggered by other inflammatory insults. Although the a priori sample size was powered on changes in acute phase protein biomarkers, 6 the study group was small and may have been under-powered for assessing changes in HbA1c and therefore subject to type 2 statistical errors. The effect on HbA1c was studied two days after elective surgery, and the longer term effect of an SIR on HbA1c remains to be clarified.
Given the caveats in which HbA1c may be unreliable, 3 HbA1c may therefore differentiate new type 2 DM from stress hyperglycaemia in acutely ill patients with new onset hyperglycaemia. The early diagnosis of type 2 DM in acutely ill patients may facilitate the early management of their diabetes and improve glycaemic control. 7 HbA1c would also identify those acutely ill patients at high risk of developing diabetes (prediabetes) who may warrant further follow-up after recovery for lifestyle advice and assessment of cardiovascular risk factors.
In conclusion, HbA1c is unaffected within two days of an acute SIR as provoked by elective orthopaedic surgery. HbA1c may, therefore, differentiate type 2 DM from stress hyperglycaemia in acutely ill patients with new onset hyperglycaemia within two days of presentation. We suggest that an elevated HbA1c is diagnostic of type 2 DM in acutely ill patients and this should facilitate the early management of newly diagnosed diabetes mellitus in these patients.
Footnotes
Acknowledgments
We thank Mr Pemmaraju and Mr Hart for allowing us to recruit patients under their clinical care.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted by the National Research Ethics Service (NRES Committee South Central –Hampshire B; study code 14/SC/1396).
Guarantor
RG.
Contributorship
AJC researched the literature, supervised the study, processed and analysed samples, analysed the data and wrote the first draft. EG researched the literature, designed the study, wrote the research protocol and submitted the study for ethical approval. RA and AM helped supervise the study, recruited patients, collected demographic data, took consent and collected samples. OLT, SD, SC, CF and RG contributed to the data. CF and RG helped design the study and write the research protocol. CF supervised sample analyses. RG conceived the study. All authors reviewed and edited the manuscript and approved the final version of the manuscript.