
Abstract
Background
Common variable immunodeficiency is a rare clinically symptomatic primary immunodeficiency disorder which manifests a wide variability of symptoms, complications. Atherosclerosis in common variable immunodeficiency patients has not been investigated yet contrary to other severe clinical complications. We aimed to investigate the chitotriosidase enzyme's role as an inflammation and atherosclerosis marker in paediatric common variable immunodeficiency patients.
Methods
Common variable immunodeficiency patients (n = 24) and healthy controls (n = 23) evaluated for chitotriosidase activity with other inflammation markers (hsCRP, myeloperoxidase, serum amyloid A, ferritin), lipid profile and echocardiographic findings (carotid artery intima media thickness – cIMT, brachial artery flow-mediated vazodilatation – FMD%).
Results
In patients, the mean chitotriosidase activity (8.98 ± 6.28) was significantly higher than the controls (5.17 ± 3.42) (P = 0.014). Chitotriosidase showed positive relation with hs-CRP (P = 0.011) and SAA (P = 0.011) but had no relation with ferritin (P = 0.155), HDL (P = 0.152) or LDL-cholesterol (P = 0.380). Mean cIMT increased in patients compared with the controls (P < 0.001) but did not show any relation with chitotriosidase (P = 0.546). FMD% decreased in patients (P < 0.001) also showing no relation with chitotriosidase (P = 0.298). Ventricular myocardial performance indexes had no significant difference, but RVEF% decreased in patients (P = 0.043).
Conclusions
High chitotriosidase activity in common variable immunodeficiency patients demonstrated in vivo the presence of activated macrophages indicating ongoing inflammation. Echocardiographic diastolic functional deficiency, increased cIMT and decreased FMD% may be accepted as early atherosclerotic findings, but none of them showed relationship with chitotriosidase activities.
Introduction
Common variable immunodeficiency (CVID) is a rare, clinically symptomatic primary immunodeficiency disorder with a prevalence of approximately 1:50,000 to 1:25,000. 1 The disease represents with a heterogeneous group of disorders characterized by hypogammaglobulinemia, defective specific antibody production, increased susceptibility to infections of the respiratory and gastrointestinal tracts and a variety of clinical presentations and complications such as autoimmunity, lymphoproliferation, splenomegaly, malignancy and granulomas.2–5 It is considered as a diverse group of diseases of unknown aetiology as many different immune system defects have been found to lead this syndrome. Besides well-known molecular genetical defects, in 80% of CVID patients, the underlying mechanism of pathology is not well defined and the recent researches are focusing on both innate and adaptive immune reactions.2,3
CVID manifests a wide variability of symptoms, complications and range of severity. Clinical aspects of atherosclerosis in CVID patients have not been investigated yet contrary to other severe clinical complications though chronic inflammation has been accepted as the common process in the physiopathogenesis of both diseases. 6
Recently, many new biomarkers have been investigated for chronic inflammation in addition to classical markers as C-reactive protein (CRP), serum amyloid-A (SAA), ferritin, etc. Chitotriosidase, as an inflammation marker, was firstly discovered in plasma yielding 1000-fold elevation synthesized from lipid-laden macrophages of patients suffering from Gaucher disease. 7 Van Eijk et al. 8 reported that polymorphonuclear neutrophils (PMNs) and activated macrophages were a source of chitotriosidase and the enzyme was located in the specific granules of human PMNs and secreted following stimulation with granulocyte macrophage colony-stimulating factor (GM-CSF). It is thought to play an important role in the mammalian innate immune response against fungi, bacteria and other chitin comprised pathogens. 8 As chitotriosidase is synthesized exclusively by activated macrophages, its activity has been proposed as a biochemical marker of macrophage accumulation in several diseases. It is also elevated in other pathological inflammatory (or not) diseases including familial Mediterranean fever (FMF), 9 interstitial and chronic obstructive lung diseases 10 , tuberculosis, 11 thalassemia, 12 sarcoidosis, 13 multiple sclerosis, 14 malignity 15 and in parasitic infections. 16
Recent studies showed the enzyme' s crucial role in atherosclerosis,17,18 coronary artery disease, 19 acute ischemic stroke, 20 Alzheimer's disease 21 and glucose intolerance 22 indicating that the enzyme might have a certain role in inflammation.
The formation of lipid-laden foam cells from activated macrophages that are activated by cytokins IFN-ϒ/TNF-α, represents a landmark for atherosclerosis and secretes chitotriosidase enzyme. Boot et al. 23 have shown that chitotriosidase activity was elevated up to 55-fold in extracts of atherosclerotic tissue.
CVID patients' life expectancy is increasing due to definitive molecular diagnosis and usage of efficient antibiotics or intravenous immunoglobulin (IVIg) therapy. Atherosclerotic changes in paediatric CVID patients have not been investigated yet in contrast to other severe complications. In the present study, we investigated the chitotriosidase enzyme activity in pediatric CVID patients as an inflammation marker in conjunction with other well-known inflammation markers and early atherosclerosis indicators determined by echocardiography as carotid intima media thickness etc. (cIMT). So we aimed to investigate chronic inflammatory changes and also atherosclerotic modification in these patients independently from other severe complications.
Patients and methods
The patient group consisted 24 paediatric CVID patients who were followed up in the outpatient and inpatient clinics of Ege University Faculty of Medicine, Department of Pediatric Immunology, Izmir, Turkey. Written informed consents were obtained from parents. The study was approved by the hospital's ethics committee and was conducted in accordance with the Helsinki Declaration. Patients were diagnosed and classified according to both clinical and laboratory criteria reported by European Society for Immunodeficiencies (ESID). 24 Diagnosis criteria for CVID were as follows: (1) marked decrease of IgG (at least two SDs below the mean for age), (2) reduced serum IgA and/or IgM, (3) specific-antibody deficiency, (4) age > 2 years, and (5) exclusion of other known causes of hypogammaglobulinemia. All demographic information including name, gender, date of birth, age at onset of symptoms, age at admission, age at diagnosis, family history and consanguinity, clinical symptoms or complications (autoimmune disease, chronic giardiasis, granulomatosis, lymphoma or any malignancy, lymphadenomegaly, hepatomegaly, splenomegaly, bronchiectasis, musculoskeletal system findings, celiac-like disease), follow-up duration and laboratory data were recorded. The control group consisted 23 healthy children within the similar age range.
Whole blood count, leukocyte counts, absolute lymphocyte counts were performed with a haemocounter (Cell-Dyn 3700, Abbott Diagnostics, USA).
Serum immunoglobulins (IgG, IgA, IgM), high sensitive CRP (hs-CRP), SAA and ferritin concentrations were analysed quantitatively by Dade Behring BNII Nephelometer, Siemens, Germany.
Other serum parameters (total cholesterol, triglyceride, HDL-cholesterol, iron and total iron binding capacity) were determined by routine laboratory methods with DxC800 autoanalyser, Beckman Coulter, USA. LDL-cholesterol concentrations were calculated according to the formula of Friedewald.
Blood samples were obtained in an EDTA-containing tube for plasma chitotriosidase activity measurements. Chitotriosidase activity was measured fluorometrically according to Hollak et al. 7 with minor modifications. Briefly, chitotriosidase activity was determined by incubating plasma with 22 μmol/L fluorogenic substrate 4-methylumbelliferyl-β-D-N,N′,N″″-triacetylchitotrioside (Sigma) in buffer (100 mmol/L citric acid and 200 mmol/L sodium phosphate, pH 5.2) for 15 min at 37 ℃. The reaction was stopped by mixing at room temperature. The substrate hydrolysis by chitotriosidase produced the fluorescent molecule 4-methylumbelliferone, which was quantified with a fluorometer (Varioskan Flash Fluorometer, Thermo Scientific, USA), and compared with a standard calibration curve. Chitotriosidase activity was expressed as micromoles of substrate hydrolysed per hour per liter of incubated plasma.
Myeloperoxidase (MPO) activities were measured according to the modified method of Grisham et al. 25 MPO activity was measured spectrophotometrically by measuring the H2O2 -dependent oxidation of 3,3′,5,5′-tetramethylbenzidine. One unit of enzyme activity was defined as the amount of MPO present that caused a change in absorbance.
All patients and healthy controls had echocardiographic evaluation by a paediatric cardiologist. Carotid artery intima media thickness (cIMT) was assessed by an ultrasound device (GE Vingmed, Vivid 7.0, Ultrasound AS, Horten, Norway) equipped with high resolution. All measurements were obtained at end diastole by electrocardiographic triggering. Imaging of the distal right carotid was performed, and repeated measures were obtained at the common carotid far wall. The mean of three measurements was accepted as the cIMT value.
The myocardial performance index (MPI) was calculated using the following equation: [isovolumetric contraction time + isovolumetric relaxation time] / left ventricular ejection time. Left ventricular shortening fraction (LVFS), left ventricular ejection fraction (LVEF), left ventricular myocardial performance index (LVMPI), right ventricular shortening fraction (RVFS), right ventricular ejection fraction (RVEF) and right ventricular myocardial performance index (RVMPI) were also determined.
Flow-mediated dilatation measurements of the internal diameter of the brachial artery were assessed at the end diastole and were calculated as the mean of three consecutive measurements. After the baseline measurements of the brachial artery diameter had been recorded, the cuff was inflated to 50 mm Hg higher than the systolic blood pressure for 5 min to create forearm ischaemia. The cuff was subsequently deflated, and the arterial diameter was measured at 45 to 60-s intervals after deflation. Flow-mediated dilatation of the brachial artery was expressed as the percentage change in the brachial artery diameter from baseline to reactive hyperemia (FMD%).
Statistics
All clinical and laboratory data were evaluated in relation with each other and compared in different patient profiles and control groups. Statistical analyses were performed by using SPSS Windows Version 16.0, SPSS Inc., Chicago, IL, USA. Data were expressed as mean ± SD except when indicated otherwise. Correlation comparisons between paired samples were made by Pearson's product moment correlation coefficient. Statistical comparisons of numeric data were made using Student's t-test or Mann Whitney U test. Classified data were evaluated by chi-square test. A two-sided P value < 0.05 was considered to indicate statistical significance.
Results
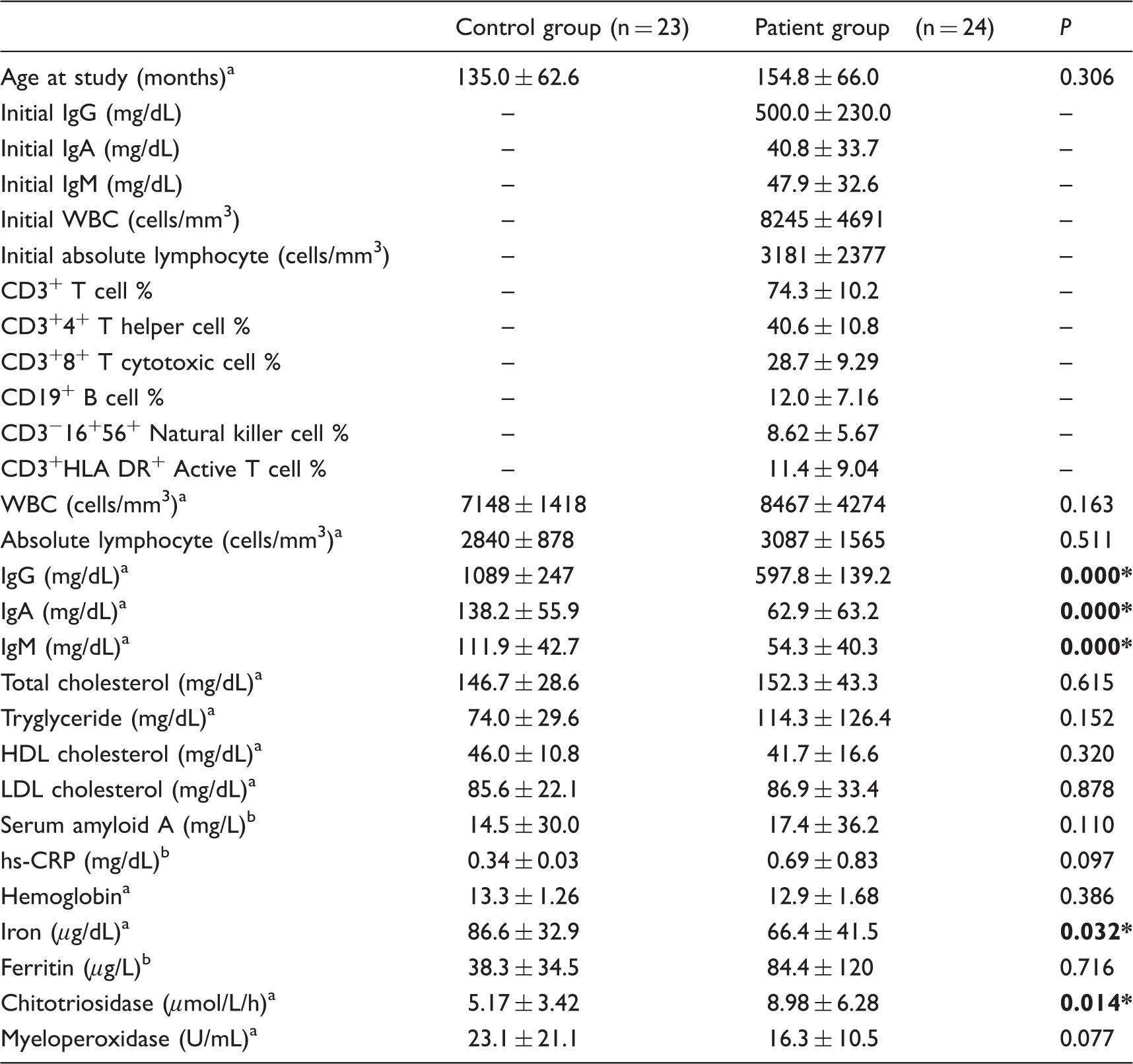
Baseline laboratory data of both control and patient groups.
t-test.
Mann Whitney U test.
In the patient group, the mean age for the initiation of symptoms, on admission and on diagnosis was 63 ± 60.1 months, 85.2 ± 54.5 months and 89.3 ± 53.6 months, consecutively. All the patients had infections on admission and sinopulmonary infections were the most frequent type (n = 21). Vasculitis, lymphadenomegaly and haemolytic anaemia were accompanied in each case. Family history for primary immunodeficiencies in siblings or first-degree relatives was positive for four patients (16.7%) and five patients (20.8%) were born to consanguineous parents. The complications which were common as follows: hepatomegaly (n = 6, 25%), splenomegaly (n = 7, 29.1%), autoimmunity (n = 2, 8.3%), musculoskeletal findings (n = 3, 12.5%), celiac-like disease (n = 1, 4.1%), lymphoma (n = 1, 4.1%), bronchectasia (n = 5, 20.8%), lymphadenomegaly (n = 7, 29.1%) and giardiasis (n = 2, 8.3%), respectively.
In the patient group, mean IgG (100%, n = 24), IgA (66.7%, n = 16) and IgM (70.8%, n = 17) concentrations were below age comparison mean values. Mean hs-CRP, SAA and ferritin concentrations were increased in the patient group, but this increase was not statistically significant (P = 0.097, P = 0.110, P = 0.716). Total cholesterol (P = 0.615), triglyceride (P = 0.152) and LDL-cholesterol (P = 0.878) concentrations also increased and HDL-cholesterol (P = 0.320) decreased in patients but showed no statistically significant difference in comparison to the control group (Table 1). Increase of hs-CRP showed negative correlation with HDL-cholesterol (P = 0.059, r = −0.409) and iron (P = 0.030, r = −0.462) concentrations.
The scatter graph for study group chitotryosidase enzyme concentrations is shown in Figure 1. In the patient group, mean concentrations (8.98 ± 6.28) were significantly higher than the control group (5.17 ± 3.42) and the difference between both groups were statistically significant (P = 0.014) (Table 1). As we evaluated the enzyme concentrations in comparison to control group's mean value, all patients except one (if mean ± 2SD values were evaluated, seven patients had high enzyme concentrations) had high values. Chitotriosidase activity increases significantly with respect to the presence of splenomegaly (P = 0.017) and hepatomegaly (P = 0.010) in three patients. Increase in chitotriosidase showed good relation with increase of hs-CRP (P = 0.011) and SAA (P = 0.011), but had no relation with ferritin (P = 0.155), HDL-cholesterol (P = 0.152) or LDL-cholesterol (P = 0.380) concentrations.
Chitotriosidase enzyme activities in patient and control groups.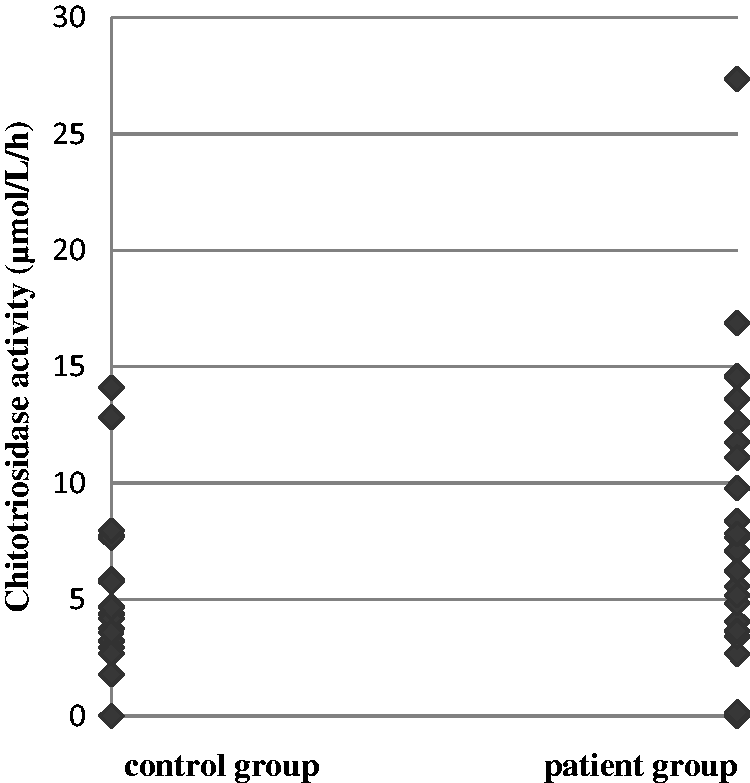
Mean MPO activities were lower in patients (16.3 ± 10.5) than controls (23.1 ± 21.1) but showed no statistically significant difference (P = 0.077) (Table 1). Seventeen patients had lower MPO activity than control group's mean minus 2SD values. MPO enzyme activities showed positive correlation with SAA increases (P = 0.024, r = 0.459).
In echocardiographic functional evaluation, RVMPIs and LVMPIs showed no significant difference. LVMPI values were higher (P = 0.561) and RVMPI values were lower (P = 0.182) in the patient group. In diastolic functional evaluation, mean mitral A (atrial contraction signal) and mitral E (early diastolic flow signal) values, which were obtained from left ventricular diastolic functions, were similar between both groups, and mitral E/A values (deceleration time) were higher in the diseased group (P = 0.196). RVEF percentages showed statistically significantly decrease in the patient group (P = 0.043). Right ventricular shortening fraction (RVFS) had negative correlation with chitotriosidase activities (P = 0.038, r = −0.478) (Figure 2).
Negative correlation between chitotriosidase activities and echocardiographic RVFS (right ventricular shortening fraction) measures in CVID patients (P = 0.038, r = −0.478).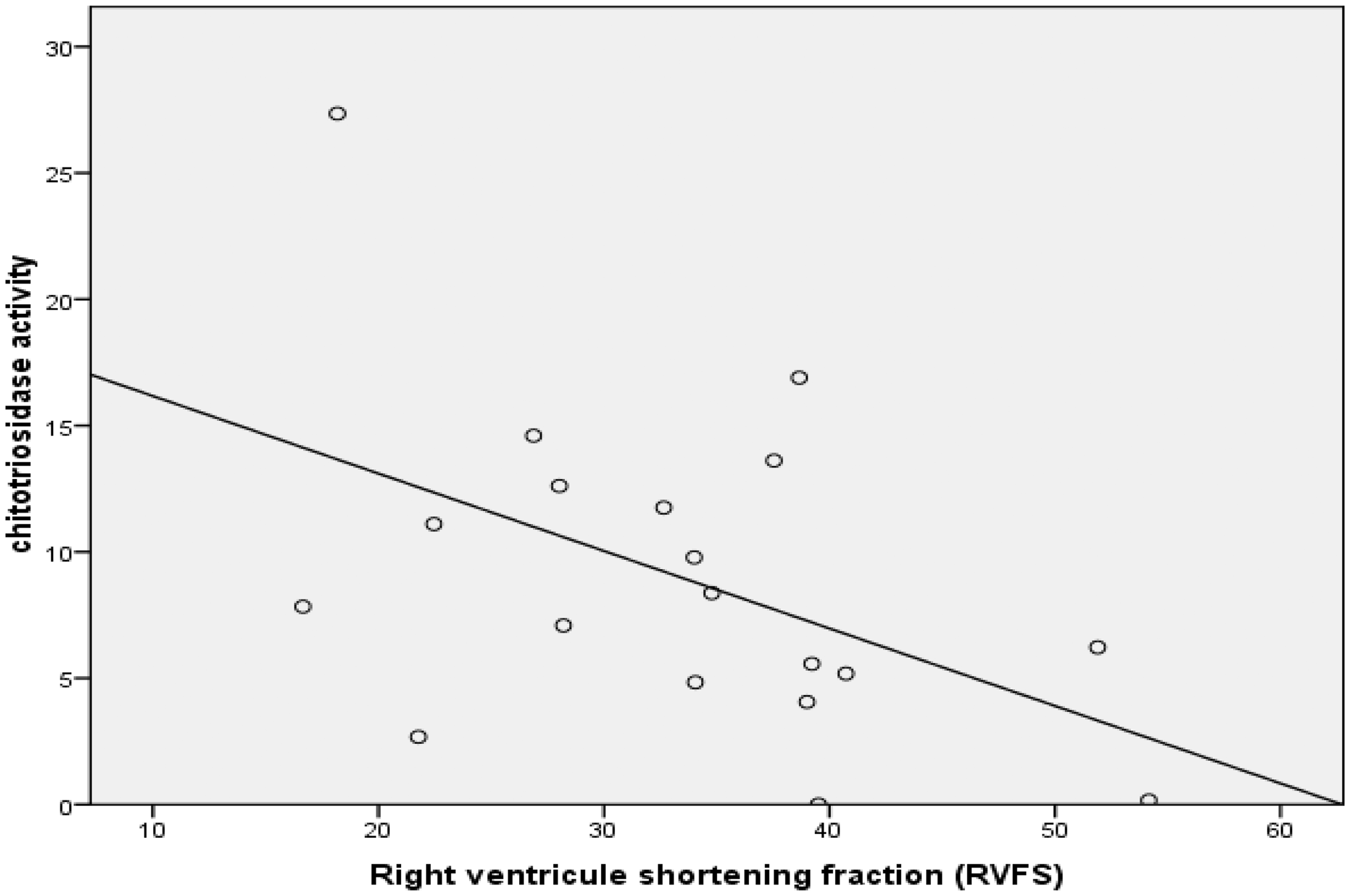
B-mode echocardiographic data in the patient and control groups (Student's t-test).
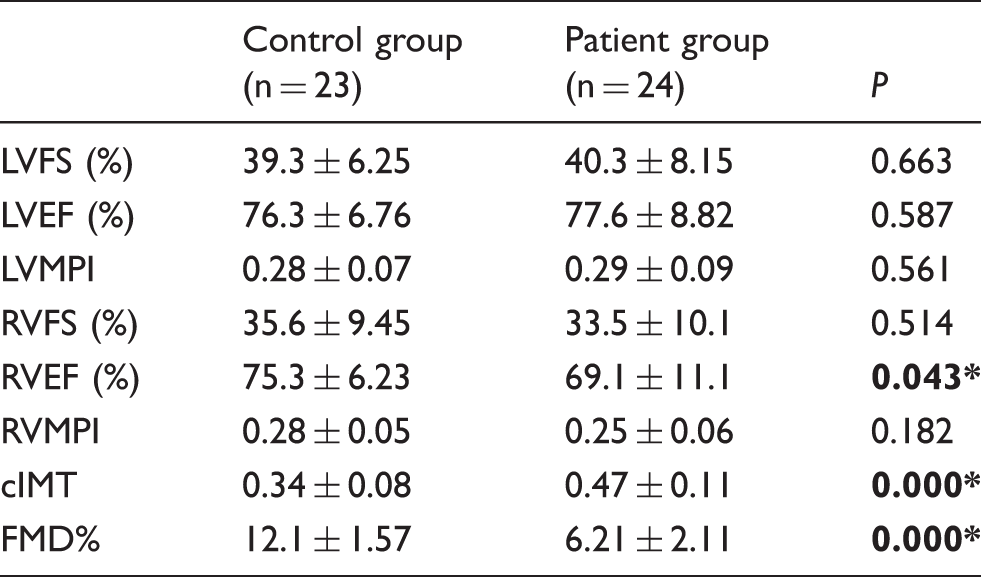
cIMT: carotid intima-media thickness; FMD: flow-mediated dilation of the brachial artery; LVFS: left ventricular shortening fraction; LVEF: left ventricular ejection fraction; LVMPI: left ventricular myocardial performance index; RVFS: right ventricular shortening fraction; RVEF: right ventricular ejection fraction; RVMPI: right ventricular myocardial performance index. Bold signifies p < 0.05.
Brachial artery mean FMD% values decreased in the patient group (6.21 ± 2.11) compared with the control group (12.1 ± 1.57) and the difference was statistically significant between both groups (P < 0.001). FMD% did not show any relation with chitotriosidase activity (P = 0.298), but hs-CRP (P = 0.468) showed good relation with SAA (P = 0.012). Three patients with high SAA values had decreased FMD%.
The patient group was evaluated as two subgroups: older (n = 7) and younger (n = 17) than 18 years. Triglyceride concentrations were higher (123.3 ± 54.7) (P = 0.031) and HDL-cholesterol concentrations were lower (28.1 ± 8.68) (P = 0.006) in older patients than younger patients (triglyceride: 77.1 ± 36.3; HDL : 47.7 ± 15.9). Inflammatory markers ferritin, hs-CRP and SAA values were higher in seven older patients but the difference was not statistically significant (P = 0.598, P = 0.252, P = 0.733). Chitotriosidase enzyme activity (P = 0.932), cMIT (P = 0.475) and FMD% (P = 0.807) did not show any difference between two groups.
Discussion
Chronic inflammation has been shown to be the cause of the development and progression of endothelial dysfunction. 26 Atherosclerosis is an inflammatory disease which initiates with the activation of endothelial cells facilitating monocyte infiltration of the vessel wall. Monocytes differentiate into macrophages which accumulate lipids forming the foam cells. These special types of macrophages are activated by growth factors and cytokines secreted by activated endothelial cells as well as macrophages. 27 Chitotriosidase is mainly produced by activated macrophages both in normal and inflammatory conditions. Boot et al. 23 have shown that chitotriosidase activity was elevated up to 55 fold in extracts of atherosclerotic tissue. CVID with chronic inflammatory process, which underlying mechanisms has not completely understood yet may need attention for atherosclerotic changes. In CVID, 4 monocytes exhibit chronic hyperactivity with heightened oxidative stress playing a role in autoimmunity, granuloma formation and impaired cell functions. The imbalance in cytokine production skews the immune system away from antibody production. This results in a failure to produce antigen-specific memory cells thus causing chronic inflammatory and granulomatous complications. In general, atherosclerosis in CVID is ignored, as more complicated clinical complications are presented and there is no research done in this field. And, since atherosclerosis begins in the childhood, it is important to define the earliest diagnostic markers as well as other well-known anatomic changes. 4
The diagnostic age for CVID shows two peaks in life, between 6 and 10 years of age and in young adulthood between 26 and 40 years. 28 It was about meanly 89.3 ± 53.6 months for our CVID patients. As generally known, our CVID patients were characterized by hypogammaglobulinemia (IgG 100%, IgA 66.7%, IgM 70.8% decreased), defective specific antibody production, increased susceptibility to infections (mostly respiratory, 87.5%) and complications such as autoimmunity (8.3%), hepatomegaly (25%), splenomegaly (29.1%), malignancy (4.1%), and bronchectasia (20.8%). Family history was positive for four patients and five patients were born to consanguineous parents.
Lipid profile changes are well-known risk factors for adult coronary artery diseases, but we can find only a few research works for CVID. Vieira et al. 29 investigated the lipid profile and other cardiovascular risk biomarkers in CVID. HDL-cholesterol (P = 0.025) and apolipoprotein A-I (P = 0.013) concentrations were significantly lower in patients which can predispose to a high cardiovascular risk and there was a negative correlation between HDL-cholesterol and triglyceride (r = −0.641; P = 0.001) concentrations. Our CVID patients had high total cholesterol (P = 0.615), triglyceride (P = 0.152) and LDL-cholesterol (P = 0.878) concentrations and low HDL-cholesterol (P = 0.320) concentrations, but no statistically significant difference was found between the patient and control groups (Table 1).
Various inflammatory markers have been well studied in coronary artery diseases. hs-CRP, which is associated with systemic inflammation has been shown to be increased in individuals with coronary artery disease.30,31 The assessment of inflammation by measuring serum CRP in childhood also might add value to the paediatric cardiovascular risk estimations. 32 CRP is found elevated in CVID patients 33 but no research has been found on its role on atherosclerotic risk estimate. In this study, the mean hs-CRP increased in CVID patients compared with controls, but the difference was not statistically significant (P = 0.097). hs-CRP elevation showed negative correlation with HDL-cholesterol (P = 0.059, r = −0.409) and iron (P = 0.030, r = −0.462). Other inflammation markers, SAA and ferritin concentrations, were also increased in the patients, but this increase was not statistically significant (P = 0.110, P = 0.716). Vieira et al. 29 showed that CVID patients had presented themselves with increased inflammatory markers – CRP (P = 0.008) and TNF-alpha (P < 0.001) concentrations were significantly higher.
In a healthy population, chitotriosidase activity is very low and originates in the circulating polymorphonuclear cells. Conversely, during the development of acute or chronic inflammatory disorders, the enzymatic activity with macrophage activation increases significantly. 34 In a few studies, serum chitotriosidase activity was investigated in patients with coronary artery disease.18,19,35,36 Kologlu et al. 17 investigated for the first time the relationship between atherosclerosis and macrophage activation markers in dyslipidaemic children. We found no research works that involved CVID patients. In CVID, activated macrophages and lymphocytes shows an increase indicating ongoing inflammation. Macrophage accumulation localized in the supraaortic and coronary vessels may be associated with increased serum chitotriosidase activity. Mean chitotriosidase activities were increased in our CVID patients compared with controls (Figure 1) and the difference between both groups was statistically significant (P = 0.014) (Table 1). All patients, except one, had high enzyme activities in comparison to controls’ mean value. Chitotriosidase activity significantly related to the presence of splenomegaly (P = 0.017) and hepatomegaly (P = 0.010) in three patients. The significant relation of chitotriosidase with hs-CRP (P = 0.011) and SAA (P = 0.011) supported the ongoing inflammation mechanism in patients.
Myeloperoxidase generates a number of reactive species that promote further oxidative modifications of LDL, and plays a significant role in the development of the atherosclerotic lesion.37,38 Mean MPO activities in CVID patients were lower compared with controls (Table 1). As MPO is the major component of the neutrophil azurophilic granules, this finding may indicate the macrophage activation is the source of chitotriosidase elevation.
Echocardiography is a noninvasive diagnostic tool for the measurement of cardiovascular disease. In functional evaluation, ventricular myocardial performance indexes of patients showed no significant difference. RVFS had negative correlation with chitotriosidase activities (P = 0.038, r = −0.478) (Figure 2). Echocardiographic measures indicated a diastolic functional deficiency.
cIMT is used as a marker for the presence of subclinical atherosclerosis in adults and children with risk factors. 39 Since cIMT values were not affected by age or gender, it is a valuable marker in clarifying the atherosclerotic process. Mean cIMT showed a statistically significant elevation (P < 0.001) in patients compared with controls (Table 2), but did not show any relation with chitotriosidase (P = 0.546), hs-CRP (P = 0.603), SAA (P = 0.603), LDL (P = 0.497) or HDL cholesterol (P = 0.157).
Brachial artery FMD measures the vasodilator response of endothelium to increased blood flow.40,41 Mean FMD% decreased in CVID patients compared with controls and the difference was statistically significant between both groups (P < 0.001). But, FMD% did not show any relation with chitotriosidase activity (P = 0.298) and hs-CRP (P = 0.468), but had relation with SAA (P = 0.012). Three patients with high SAA values had decreased FMD%.
In CVID patients, heart diastolic functional deficiency, which is characterized with a decline in performance of one or both ventricles during diastole, increased cIMT, decreased brachial artery FMD% and chitotyrosidase enzyme activity elevation may be accepted for findings for early atherosclerosis. In general, our seven patients with increased cIMT and decreased FMD% needed more careful follow-up for future cardiovascular events. Chitotriosidase activity (P = 0.932), cMIT (P = 0.475) and FMD% (P = 0.807) did not show any significant elevation in patients older than 18 years. But, triglyceride elevation (P = 0.031) and HDL-cholesterol depletion (P = 0.006) were significant. This study will give more explanation for diagnostic usage if comparative echocardiographic measures and chitotriosidase enzyme results are repeated after a few years.
CVID patients were under regular immunoglobulin replacement therapy. So, atherosclerotic changes and endothelial dysfunction may be overlooked. Ucar et al. 6 speculated that the immunomodulatory effect of regular IVIg treatment in CVID patients might supress IgG-dependent inflammation and thus protect endothelial cells from excessive cytokine exposure.
High plasma chitotriosidase activity in CVID patients demonstrated in vivo the presence of activated macrophages in such subjects indicating ongoing inflammation. On the other hand, echocardiographic early atherosclerosis findings in seven patients were noteworthy, though only two of them had high enzyme concentrations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work has been approved by local ethics committee of Ege University (approval number: 15-12/4, date: 20.01.16).
Guarantor
EA.
Contributorship
EA, NK designed the study and prepared the study protocol. EA obtained literature data. NK selected the patients and performed clinical follow‐up. EL performed echocardiographic evaluation. EA and ES performed laboratory evaluation and analysed the data. EA, NK prepared the first draft of the manuscript. All the authors have accepted responsibility for the entire content of this submitted manuscript and approved submission.