
Abstract
Background
Previous studies showed high frequency of duplicate errors of lactate dehydrogenase (LDH) measurement in primary lithium-heparin blood tubes. We hence evaluated imprecision of LDH testing and frequency of replicate errors in primary serum samples centrifuged at two different speeds.
Methods
Serum samples were collected from 15 healthy subjects and centrifuged at either 1300 g or 2000 g. Serum LDH was then measured on Beckman Coulter AU5800 using the International Federation of Clinical Chemistry-recommended procedure. Complete blood cell count of top layer of serum supernatant was also performed using Advia 2120. Imprecision was calculated as coefficient of variation of 10 replicates of each serum tube, whereas the frequency of replicate errors was compared to the desirable specifications for imprecision.
Results
Mean LDH values were slightly but significantly higher in serum samples centrifuged at 2000 g rather than 1300 g, whereas blood cell counts were similar. The mean imprecision of LDH was more than double in samples centrifuged at 2000 g than in those centrifuged at 1300 g (8% versus 3%). The percentage of replicate measurements exceeding the desirable specifications was more than threefold higher in samples centrifuged at 2000 g than in those centrifuged at 1300 g (30% versus 9%; P < .001).
Conclusions
The lower frequency of replicated errors in LDH measurement observed using serum samples centrifuged according to manufacturer’s instruction suggests that assay precision in serum is better if samples are centrifuged at 1300 g rather than 2000 g when the International Federation of Clinical Chemistry-recommended procedure is used.
Introduction
Lactate dehydrogenase (LDH; EC 1.1.1.27) is a prevalently cytoplasmic enzyme, which catalyses the reversible conversion of pyruvate to lactate under anaerobic conditions. Due to the widespread localization in human tissues, the activity of this enzyme considerably increases in blood after cell damage attributable to a large number of pathological conditions, including cardiac and liver injury, haematological disturbances, and cancer. 1
Interestingly, previous studies described a considerably high frequency of duplicate errors (from 19 to 35%) with the International Federation of Clinical Chemistry (IFCC)-recommended method for LDH in primary lithium-heparin blood tubes, a phenomenon that was partially attributed to the presence of cellular aggregates in the top layer of plasma.2–4 Therefore, we planned another investigation aimed to establish the imprecision of LDH testing and frequency of replicate errors in primary serum samples separated with conventional and higher centrifugation force.
Materials and methods
The study population consisted in 15 healthy subjects (8 women and 7 men; mean age 44 ± 11 years) recruited among the laboratory personnel, who needed blood collection for routine testing. Three venous blood specimens were collected at fasting from each subject in primary serum blood tubes (13 × 100 mm × 6.0 mL BD Vacutainer® Plus plastic serum tube with spray dried clot activator; Becton Dickinson Italia SpA, Milan, Italy). The first tube was collected and always discharged, another blood tube was subjected to conventional centrifugation according to manufacturer’s instruction (1300 g for 10 min at room temperature), whereas the remaining tube was centrifuged at higher speed (i.e. 2000 g for 10 min at room temperature). From subjects 1 to 7, the secondly drawn tube was centrifuged at 1300 g and the thirdly drawn tube at 2000 g, whereas the sequence was inverted from subjects 8 to 15 (i.e. second tube centrifuged at 2000 g and third tube centrifuged at 1300 g, respectively). The primary blood tubes were then loaded in a Beckman Coulter AU5800 (Beckman Coulter Inc., Brea, CA, USA), where LDH was measured in 10 consecutive replicates per each tube using the IFCC-recommended procedure. 5 Briefly, lactate and NAD are converted to pyruvate and NADH catalysed by LDH. The rate of absorbance change at 340 nm is directly proportional to LDH activity (reference range in adults; 140–371 U/L; total imprecision: 1.8–2.2%). After clinical chemistry testing was completed, a blood cell count of the top layer of serum supernatant was performed using Advia 2120 (Siemens Healthcare Diagnostics, Tarrytown NY, USA). According to manufacturer’s specifications, the limits of quantification are 0.01 × 1012/L for red blood cells, 0.02 × 109/L for white blood cells (WBC) and 5.0 × 109/L for platelets (PLT), respectively. All measurements were completed within 3 h from sample collection.
The analysis of values obtained in paired blood tubes was performed with paired Mann–Whitney test, Spearman’s correlation (for continuous variables) and Chi-square test with Yates’ correction (for categorical variables), using Analyse-it (Analyse-it Software Ltd, Leeds, UK). Imprecision was calculated as coefficient of variation of the 10 replicates in each tube. The frequency of LDH replicate errors was assessed by calculating the percentage of replicate measurements exceeding the desirable specifications for imprecision calculated from biologic variation (i.e. 4.3%). 6 All subjects provided a written consent for enrollment in the study, which was approved by the Institutional Review Board and carried out according to the Declaration of Helsinki.
Results
The mean concentration of LDH in the primary serum tubes centrifuged at 2000 g was slightly but significantly higher than that of paired specimens centrifuged at 1300 g (312 ± 59 versus 317 ± 59; P = .040). The median values of WBC (0.02 × 109/L, range 0.01–0.05 × 109/L versus 0.01 × 109/L, range 0.01–0.06 × 109/L; P = .055), red blood cells (always lower than 0.01 × 1012/L) and PLT (1 × 109/L, range 0–2 × 109/L versus 1 × 109/L, range 1–2 × 109/L; P = .094) counts were instead similar between serum specimens centrifuged at 1300 g or 2000 g, with a large number of values lower than the limits of quantification. The mean analytical imprecision of LDH measurements was more than double in samples centrifuged at 2000 g than in those centrifuged at 1300 g (i.e. 8% versus 3%) (Figure 1). Interestingly, the imprecision was higher in samples with lower LDH values, especially for those centrifuged at 2000 g. Although we cannot provide a definitive explanation for this finding, a similar trend has been previously observed by Herzum et al.
7
and has been at least in part attributed to the larger imprecision of the IFCC-recommended assay at lower LDH values.
Imprecision of 10 replicate measurements of lactate dehydrogenase (LDH) in primary serum samples centrifuged at either 1300 g (○) or 2000 g (⋄). The dotted line is drawn at the desirable specifications for imprecision calculated from biologic variation (i.e. 4.3%).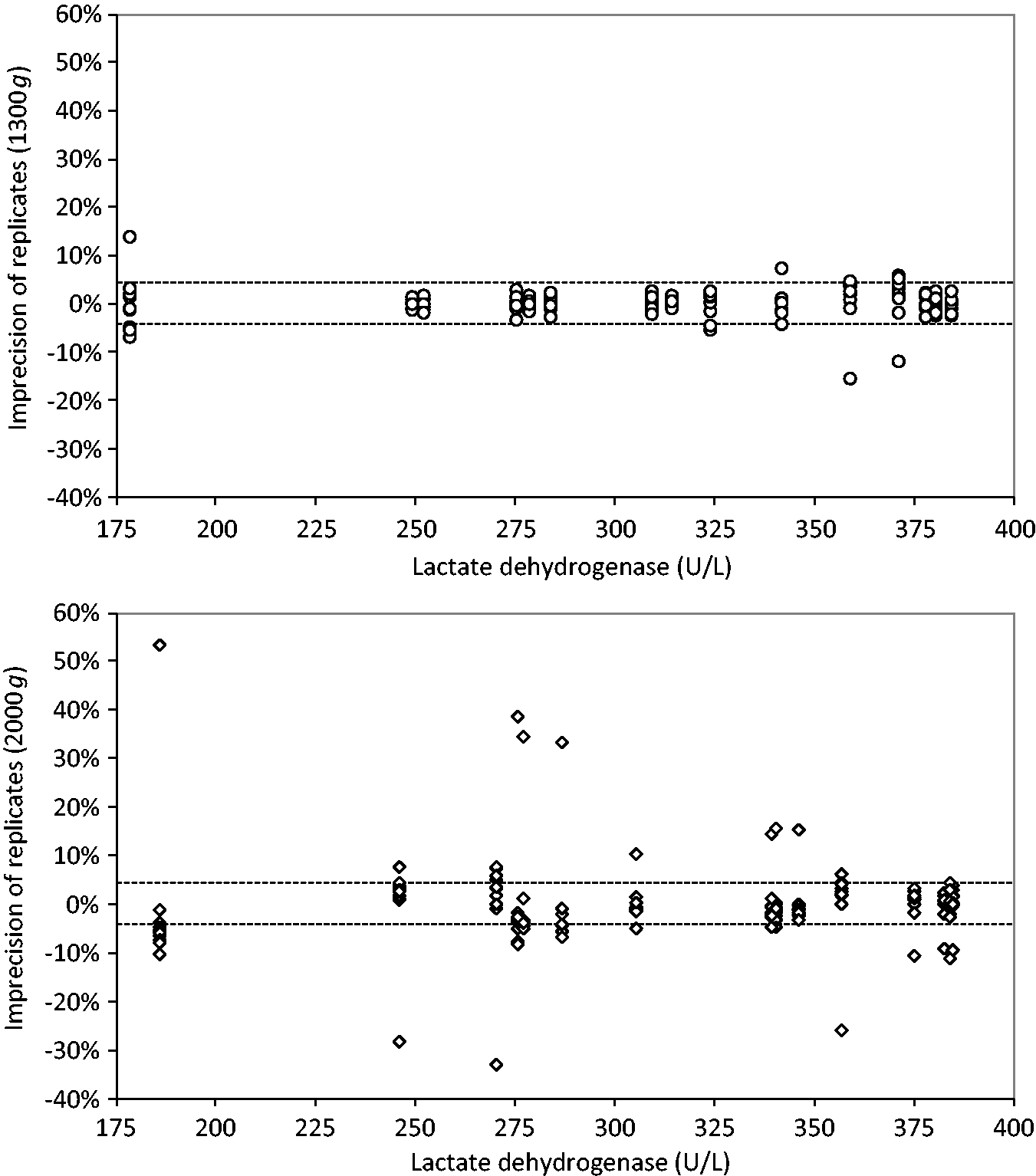
Even more importantly, the percentage of replicate measurements exceeding the desirable specifications for imprecision was more than threefold higher in samples centrifuged at 2000 g (45/150; 30%) than in those centrifuged at 1300 g (14/150; 9%; P < .001) (Figure 1). The rate of replicate measurements exceeding the 5.6% allowable difference between duplicates used by Bakker et al. was 6/150 (i.e. 4%) in serum samples separated at 1300 g, thus consistently lower than the frequency of duplicate errors reported in plasma samples. No significant relationship was found between analytical imprecision of LDH measurements and residual blood cells in serum (correlation between LDH and WBC: r = −0.154 and P = .582; correlation between LDH and platelets: r = −0.330 and P = .227).
Discussion
Previous studies reported that the frequency of duplicate errors of LDH measurement can be as high as 20% in primary heparin-plasma tubes with separator, but could be even higher (i.e. 35%) in primary heparin-plasma tubes without separator.2–4 According to local routine conditions, our results suggest that the precision of LDH testing is limited in serum samples, especially when the primary blood tubes are centrifuged according to manufacturer’s recommendations (i.e. 1300 g). Although we are not allowed to directly compare our data with the results published by Bakker et al. (the article was published in 2006, and the authors used a higher centrifugation force, i.e., 3000 g), 4 we have found that the assay precision in serum is better if samples are centrifuged at 1300 g rather than 2000 g when the IFCC-recommended procedure is used. Interestingly, previous studies have observed better performance using serum compared with plasma, 8 thus supporting the IFCC recommendation that serum should be considered the preferred biological matrix for LDH assessment. 5 The inter-assay imprecision of 10 replicates of the primary serum samples centrifuged according to manufacturer’s instructions was globally low (<10% when compared to the desirable specifications for imprecision, decreasing to 4% when compared with the 5.6% allowable difference used by Bakker et al. 4 ). Interestingly, it has been previously reported that the high frequency of duplicate errors in heparin-plasma was not attributable to inappropriate sample preparation, since this problem was not eliminated by increasing the centrifugation speed. 1 Our results not only support this conclusion but also show that an increased centrifugation force generates slightly but significantly higher LDH values in serum and considerably enhances replicated errors. The former aspect may achieve clinical significance for values close to the upper limit of the reference range. It is also noteworthy that higher centrifugation forces are occasionally used in stat laboratories, to accelerate sample separation for urgent testing. According to our findings, it seems hence reasonable to discourage this practice in order to maintain an acceptable imprecision of LDH measurement in serum using the IFCC-recommended method.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The written informed consent was obtained from the subjects. The study was approved by Institutional Review Board of Academic Hospital of Parma.
Guarantor
GL.
Contributorship
GL was involved in study design, sample collection, data analysis and wrote the first draft of the manuscript. RB, MD and RA were involved in sample analysis and provided contribution in writing the manuscript. All authors reviewed, edited and approved the final draft of the manuscript.