
Abstract
Background
Use of a hospital pneumatic tube system may be associated with measurement errors.
Methods
A venous blood sample was collected from 79 patients into a pair of lithium heparin tubes; one tube was sent to the laboratory by porter and the other was sent via the pneumatic tube system. Plasma lactate dehydrogenase concentrations were then assayed.
Results
Lactate dehydrogenase concentrations were overestimated (median bias: 18.8%) when evacuated vacuum lithium heparin tubes were sent by pneumatic tube system. This bias was reduced by bubble-wrapping the standard lithium heparin tube or using Monovette lithium heparin tubes in aspiration mode (median bias: +8.7% and −0.3%, respectively).
Conclusions
Cushioning and aspiration-mode sampling may limit pneumatic tube system-associated overestimation of lactate dehydrogenase concentrations.
Introduction
Pneumatic tube systems (PTSs) are widely used to transport samples rapidly and cost-effectively from hospital wards to the central laboratory. However, PTS transportation of blood specimens is known to be associated with aberrant assay results for plasma lactate dehydrogenase (LD), due to the mechanical disruption of blood cells. This bias is particularly problematical for leukaemic patients with fragile leukocyte membranes 1 but is not absent in subjects with normal blood cells. 2 The PTS’s effects increase with transportation speed, rapid acceleration and deceleration when changing in direction, transportation distance and a lack of cushioning.3,4 Cell membrane damage and lysis can also be influenced by the type of sample and the choice of phlebotomy site and/or method. 1 However, susceptibility to PTS-induced cell lysis varies significantly from one individual to another. 2 The results of the present study suggest that PTS interference with LD assays can be reduced through gentle aspiration of the blood into the tube and (to a lesser extent) use of adequate cushioning.
Methods
Sample collection
A venous blood sample was collected from each of 79 patients in a nursery unit by filling two 4-mL Vacutainer lithium heparin (LH) plastic tubes (Becton Dickinson, USA; diameter: 13 mm; length: 75 mm; reference: 368884) in vacuum mode (our standard procedure). Samples were collected by phlebotomists using a standard needle (diameter: 0.8 mm; length: 38 mm). About 15 min after phlebotomy, one of the Vacutainer LH tubes was sent to the central lab by porter; this was considered to be the reference sample. The other tubes were sent to the central lab via the PTS (Swisslog, Switzerland). For 28 of the 79 patients, a 4-mL S-Monovette LH plastic tube (Sarstedt, Germany; diameter: 13 mm; length: 75 mm; reference: 04.1920.100) was filled in aspiration mode during the above-mentioned venipuncture (S-Monovette systems can be used in either vacuum or aspiration mode). The tubes were filled to capacity. For 31 of the remaining 51 patients, a third Vacutainer LH tube was filled during the venipuncture mentioned above but then wrapped in cushioned, bubble-wrap packaging.
The PTS
Each sample was first inserted in a disposable plastic bag. The latter was placed in a second plastic bag with parachutes, which was introduced into the one-way PTS from the nursery unit using a soft-start technique (i.e. initial aspiration, followed by midway airflow reversal and thus propulsion). The 1100-m transmission path included several tight turns, but the maximum transmission speed was limited to 6 m/s. The PTS was fitted with a soft landing capability, i.e. (i) the cessation of active propulsion prior to arrival and (ii) cushioning at the point of receipt in the central laboratory. The transportation time (whether by porter or by PTS) was less than 10 min.
Laboratory analyses
Upon receipt by the laboratory, samples were promptly centrifuged (10 min at 2465 g) in the same batch. The plasma LD concentrations were measured within 30 min on a Cobas 8000 analyzer (Roche Diagnostics, USA).
Statistical analysis
Statistical analyses were performed with JMP 9 software (SAS Institute, Cary, NC, USA). A paired t-test was used to compare the results for PTS- and porter-delivered samples. The threshold for statistical significance was set to P < 0.05. Values exceeding the total allowable error (TEa) of 11.4% were considered to be medically significant. 5
Results
Plasma LD assay results for samples collected in LH tubes and then sent to the central lab via a PTS.
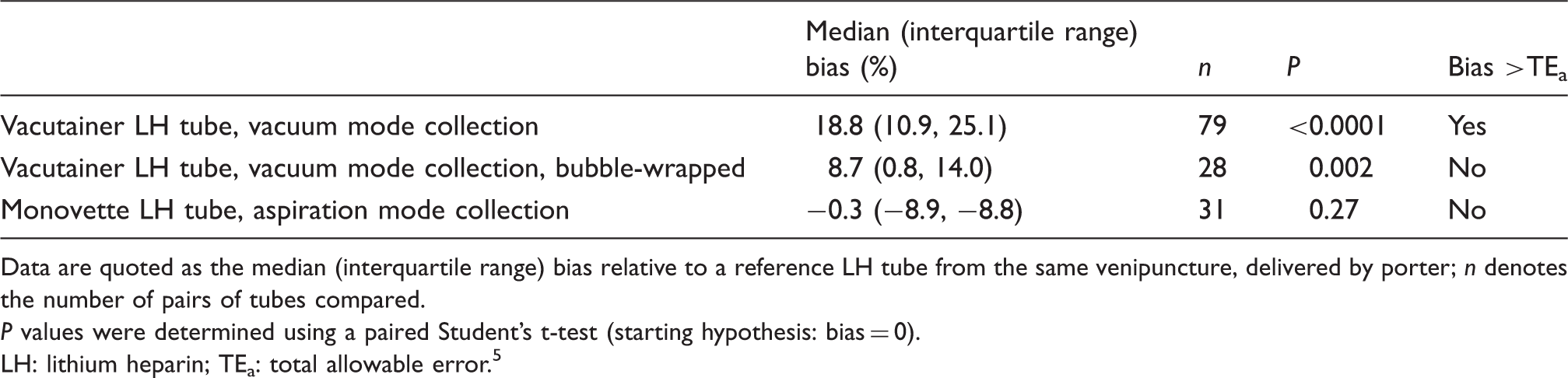
Data are quoted as the median (interquartile range) bias relative to a reference LH tube from the same venipuncture, delivered by porter; n denotes the number of pairs of tubes compared.
P values were determined using a paired Student’s t-test (starting hypothesis: bias = 0).
LH: lithium heparin; TEa: total allowable error. 5
Discussion
A health care establishment should always establish whether medically significant errors might result from use of its PTS.3,4 Here, we confirmed the medically significant overestimation of plasma LD assay results when samples were collected in standard, evacuated LH tubes and transported via a PTS. Our investigation was prompted by falsely elevated LD results (undetected when considering the haemolysis index) that had led to inaccurate diagnostic tests for lymphoma in several patients. Interestingly, we found that lithium heparin containers used in aspiration mode (such as the S-Monovette) can abolish the PTS-related overestimation of LD concentrations. Lippi et al. 6 have already emphasized the beneficial effect of manual, slow, gentle blood aspiration of plain serum into S-Monovette tubes on the accuracy of LD assays, relative to vacuum mode collection. We hypothesize that significant sheer stress during blood drawing can weaken blood cells and contribute to haemolysis during PTS transport. Conversely, lower stress during aspiration collection may help to prevent spurious haemolysis during both venipuncture and PTS transport. Furthermore, we speculate that the absence of head space in the S-Monovette container (allowing thorough filling, as in a syringe) limits the damaging motion of blood cells during transport. Alternatively, the placement of bubble-wrap around blood collection tubes can reduce the PTS-related overestimation of LD concentrations; our results confirm Kavsak et al.’s 4 report on the benefits of using cushioning (such as foam liner in the tube) and a soft landing system at the end destination. We found that bubble-pack with large bubbles is preferable, since our results with small-bubble wrapping were disappointing (data not shown).
In summary, more accurate LD assay values can be obtained by gentle aspiration of the blood into the tube and (to a lesser extent) cushioning the tube during transport. The substantial dispersion of LD values observed for all sampling/transportation modes might be due to interindividual variability; hence, interindividual differences in susceptibility to haemolysis should always be taken into account. 2
Footnotes
Acknowledgements
We thank Catherine Ribot and Aurelie Chuin for their excellent technical assistance. We thank Dr David Fraser for helpful comments on the manuscript’s English.
Declaration of conflicting interests
All the authors declare no conflicts of interest with respect to this work.
Funding
This work is funded by the CHRU de Lille.
Ethical approval
Not required.
Guarantor
ISV.
Contributorship
Each author has made substantial contributions to (i) conception and design, acquisition of data or analysis and interpretation of data; and/or (ii) drafting the article or revising it critically for important intellectual content. All the authors have approved the submitted manuscript.