
Abstract
Background
Acromegaly is characterized by excess growth hormone and insulin-like growth factor-1 concentrations. There is conflicting evidence as to whether acromegaly is associated with an increased risk of atherosclerosis. Apelin is an adipose tissue-derived peptide that may be associated with hyperinsulinemia. Fetuin-A is a hepatocyte produced plasma glycoprotein that has an important role as a calcification inhibitor. The aim of this study was to examine apelin, fetuin-A, and procalcitonin concentrations and to assess their relationship with carotid intima medial thickness (cIMT) in subjects with acromegaly.
Methods
Apelin, fetuin-A, and procalcitonin serum concentrations were measured in 37 (20 inactive and 17 active) subjects with acromegaly and 30 control subjects, along with carotid intima medial thickness.
Results
The concentrations of apelin, fetuin-A, and procalcitonin were increased in subjects with acromegaly. There were significant correlations between apelin, fetuin-A, and procalcitonin in subjects with acromegaly. Carotid intima medial thickness values were similar between control subjects and subjects with acromegaly.
Conclusions
Carotid intima medial thickness was not increased in subjects with acromegaly. It is possible that the increased apelin and fetuin-A concentrations observed play a protective role against the development of atherosclerosis in subjects with acromegaly.
Introduction
Acromegaly is an uncommon chronic disorder characterized by classical clinical features caused by excess growth hormone (GH) and consequent raised concentrations of insulin-like growth factor-1 (IGF-1). This condition may be associated with increased morbidity and mortality, considered to be mainly due to cardio-cerebrovascular disease (although the latter is unclear). 1 In most cases, acromegaly is caused by a pituitary somatotroph adenoma that secretes excess GH, which leads to insulin resistance, glucose intolerance, and increased prevalence rates of atherosclerosis and cardiovascular mortality.1,2 The presence of early atherosclerotic changes may be assessed by measuring carotid intima medial thickness (cIMT) with carotid Doppler ultrasonography (USG).3–5
Apelin and the APJ (apelin) receptor are expressed in a wide variety of tissues, including heart, brain, kidneys, and lungs.6–9 Apelin is a peptide growth factor that exhibits high affinity binding with the APJ receptor, which has high sequence homology with the angiotensin II type 1 receptor, but does not bind angiotensin II.10,11 Procalcitonin and fetuin-A are proteins that are mainly secreted by the liver.12,13 Procalcitonin secretion is closely related to inflammatory mediator concentrations, 12 while fetuin-A inhibits arterial calcium deposition in vitro. 13 Clinical studies have demonstrated that circulating fetuin-A concentrations are positively associated with fat accumulation in the liver, insulin resistance, and metabolic syndrome.14–16
Data on accelerated atherosclerosis and increased cardiovascular risk in acromegaly are somewhat conflicting and have been based for the most part on retrospective case series reports.17,18 The aim of this study was to examine apelin, procalcitonin, and fetuin-A concentrations and assess their relationship with cIMT in subjects with acromegaly.
Material and methods
This study was approved by the institutional ethics and research committee of Pamukkale University. Informed consent was obtained from all participants. Measurements were performed in 37 acromegalic patients (20 male and 17 female) and 30 healthy controls (15 male and 15 female). The mean ages of the patient and controls were similar (51.5 y ± 10.5 and 46.4 ± 6.9, respectively, P > 0.05).
Height and weight were measured with participants wearing light clothes and no shoes, and body mass index (BMI) was calculated as weight (kg)/height (m) 2 . Systolic and diastolic blood pressures were measured twice in the seated position after 5 min of rest.
Serum insulin, thyroid stimulating hormone (TSH), GH, and IGF-I concentrations were measured by chemiluminescent assay (Immulite 2000, Siemens AG, Erlangen, Germany). Serum concentrations of glucose, triglyceride, HDL-cholesterol, and LDL-cholesterol were measured on a Beckman-Coulter LX-20 analyzer (Beckman-Coulter Inc., Brea, CA, USA), with reagents supplied by the manufacturer.
Acromegaly subjects with GH≤1 μg/L and IGF-1 concentrations within the healthy population reference ranges appropriate for age and sex were classified as “inactive,” and patients with GH>1 μg/L, and higher IGF-1 concentrations, were classified as having “active” acromegaly. Insulin resistance was calculated according to the homeostasis model assessment (HOMA) method, using the following formula: (fasting plasma insulin [mIU/L × fasting plasma glucose (mmol/L)]/ 22.5. A HOMA-IR cutoff value >2.7 is considered to indicate insulin resistance.
Blood samples were obtained by venepuncture between 8:00 and 10:00 am after a 12 h fast. Plasma total cholesterol, triglycerides, HDL, LDL, TSH, GH, IGF-1, IGFBP3, insulin, and glucose concentrations were measured immediately. Serum samples for apelin, procalcitonin, and fetuin-A measurement were frozen at −80℃ until analysis (RayBio® Human Apelin kit, RayBiotech, Norcross, GA, USA; Booster® Human Fetuin-A kit, RayBiotech, Norcross, GA, USA; CUSABIO® Human Procalcitonin kit, CSB-E09502h, CUSABIO, Hubei, China) according to the manufacturers’ instructions. The intra-assay and inter-assay coefficients of variation (%CV) varied between 10–15% (apelin), 10–12% (fetuin-A), and <8–<10% for (procalcitonin).
B-mode USG of the left and right common and internal carotid arteries was performed with measurements made at least 15 min after resting in a supine position. After bilateral, longitudinal, and transverse examination of the carotid arteries, two sets of standardized images were obtained at 5-min intervals at two different points: one at the lateral angle of the carotid artery bulb and 20 mm proximal to the bifurcation. The common cIMT was calculated as the mean of the left and right measurements, and cIMT values >0.8 mm were considered as increased thickness.
Statistical analysis was done with SPSS (Statistical Package for Social Sciences) 13.0 software (SPSS Inc, Chicago, IL, USA). Discrete variables were expressed as counts (percentage) and interquartile ranges. In the statistical evaluations, one-way analysis of variance test was used to observe any differences between control group, active acromegaly, and inactive acromegaly subject groups. In the determination of different groups, Duncan multiple comparison method was used. The Bonferroni–Dunn procedure was used to compare mean values between the groups. In addition, logistic regression and Pearson’s correlation tests were used for association between parameters. All testing was two-tailed and p values less than 0.05 were considered to indicate statistical significance.
Results
Characteristics of subjects with inactive acromegaly, active acromegaly, and controls. Results given as median (interquartile range).
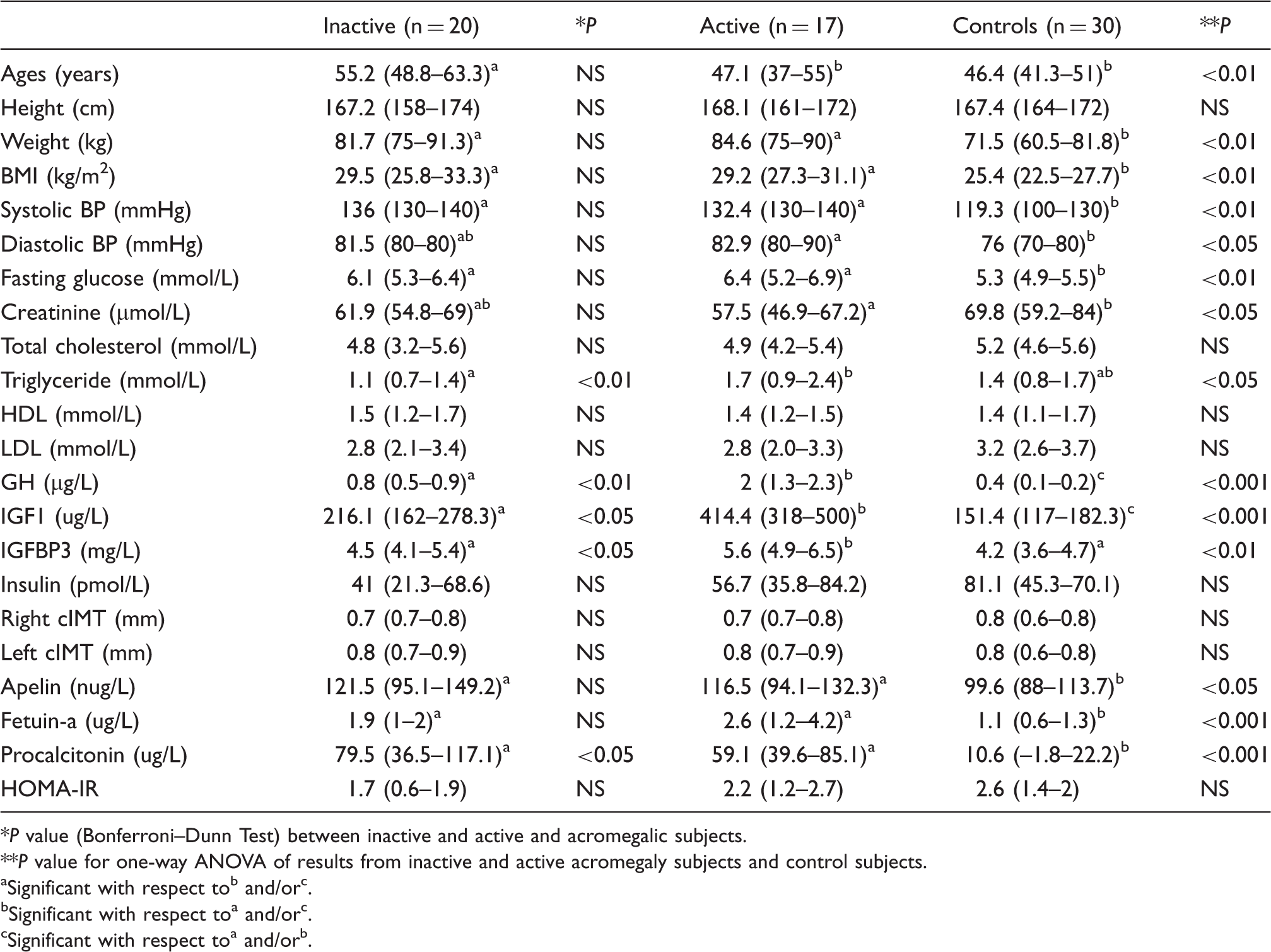
P value (Bonferroni–Dunn Test) between inactive and active and acromegalic subjects.
P value for one-way ANOVA of results from inactive and active acromegaly subjects and control subjects.
Significant with respect tob and/orc.
Significant with respect toa and/orc.
Significant with respect toa and/orb.
Correlations between apelin, fetuin-A, procalcitonin, GH, IGF-1 concentrations and BMI in subjects with acromegaly.
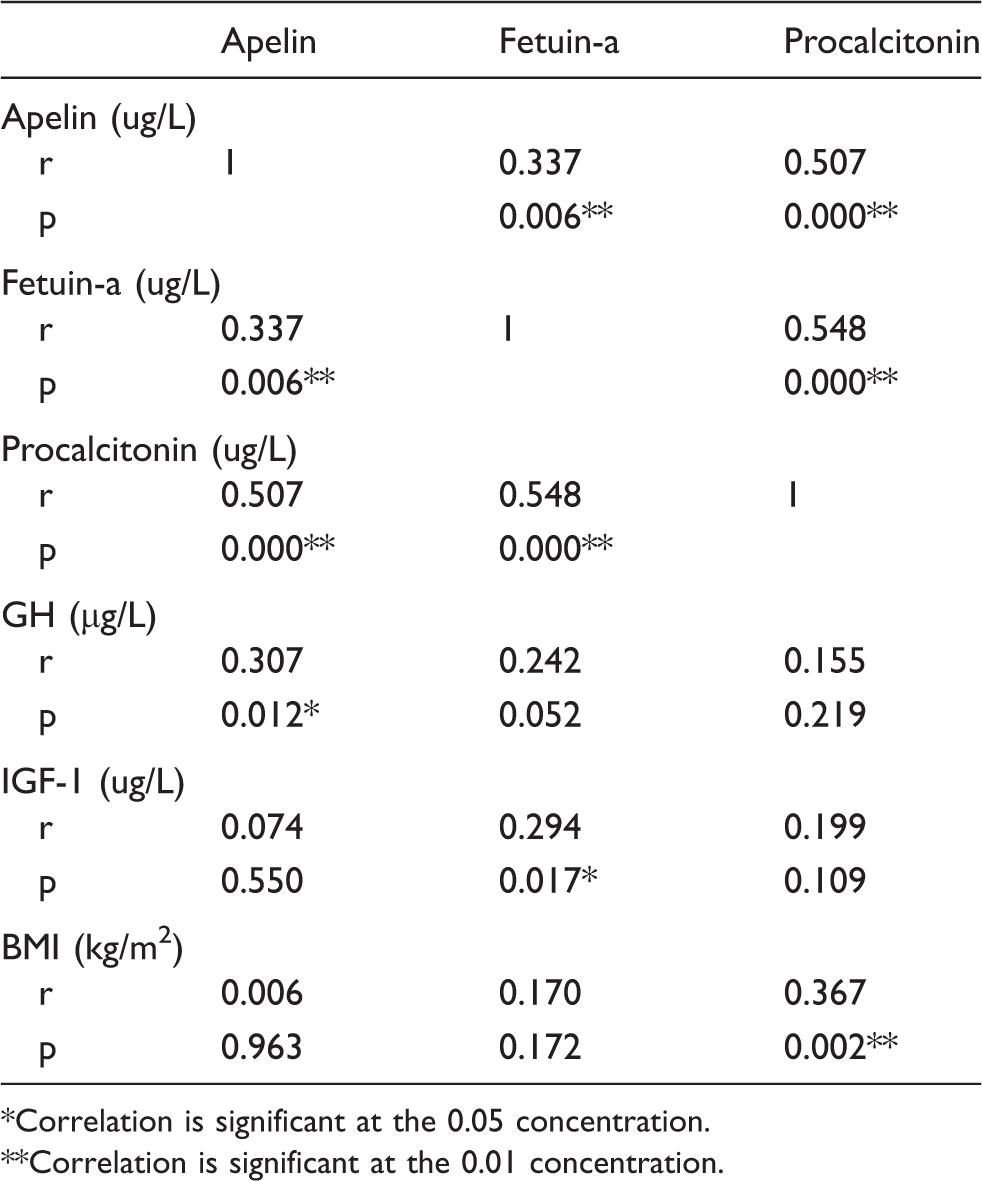
Correlation is significant at the 0.05 concentration.
Correlation is significant at the 0.01 concentration.
Discussion
The physiological importance of fetuin-A, procalcitonin, and apelin concentrations in acromegaly has been unclear. The present study found higher concentrations of fetuin-A, procalcitonin, and apelin in subjects with acromegaly but no increase in cIMT.
Acromegaly-related symptoms are usually associated with metabolic and cardiovascular complications, such as obesity, hypertriglyceridemia, diabetes mellitus, and hypertension, all of which may confer increased risk of atherosclerosis. Studies of acromegaly have reported differing findings regarding the relationship with atherosclerosis.19–21 Fetuin-A, a liver-derived inhibitor of calcification, has been inversely associated with arterial stiffness and cardiovascular morbidity and mortality. 22 Prospective studies have suggested that low serum fetuin-A concentrations may be a predictor of coronary artery disease incidence, severity, and related mortality.23–25 The cardioprotective role of fetuin-A has been supported by low circulating fetuin-A concentration as a negative predictor of acute coronary disease evolution. 25 Insulin resistance in acromegaly causes impaired glucose tolerance and type 2 diabetes in 60 and 25% of patients, respectively. 26 Studies performed in laboratory animals and humans suggested that fetuin-A induces insulin resistance,27–30 which supports the hypothesis that fetuin-A may also play a role in the pathophysiology of acromegaly. However, the relationship of fetuin-A to insulin resistance is still a subject of debate and the physiological importance of fetuin-A in acromegaly remains unclear. Our results show that although fetuin-A concentration was increased in subjects with acromegaly there was no correlation between fetuin-A concentration and insulin resistance or cIMT. This finding supports the suggestion that high serum fetuin-A concentration may have a protective effect against artherosclerosis. The putative protective action of fetuin-A may act through a direct antiatherogenic effect or through an anti-inflammatory action. To our knowledge, this is the first study for to examine serum fetuin-A concentrations in acromegaly. A limitation of our study is the relatively small number of subjects with acromegaly included and therefore the findings need to be confirmed in a larger study.
The functions of apelin and its receptor are not fully understood. Various studies have suggested that apelin is involved in body fluid homeostasis 31 and cardiovascular system regulation.32,33 It is well known that bone mineral disorders and the related vascular calcification plays an important role in the pathogenesis of cardiovascular disease. It has been proposed that apelin is protective against vascular calcification through inhibition of osteoblastic differentiation of vascular smooth muscle cells. 34 However, the role of the apelin–APJ system in cardiovascular function and its relationships to other neuroendocrine pathways remain unclear. 35 Apelin injection resulted in improved cardiac function and reduced cardiac loading in vivo. 36 Serum apelin concentrations were found to be lower in uremic patients with dilated cardiomyopathy. 37 Lower apelin concentrations in patients with both chronic kidney disease and heart disease than those with chronic kidney disease without heart disease have been reported.37,38 In the present study, we found higher apelin concentrations in subjects with acromegaly than in controls and a significant correlation with GH concentration in these subjects. There was no correlation with between apelin concentration and cIMT. One possible explanation for these associations is that high apelin concentrations may play a protective role against the development of atherosclerosis.
There is conflicting evidence as to whether subjects with acromegaly are at increased risk of accelerated atherosclerosis. Cannavo et al. 39 reported that 41% of subjects with acromegaly were at risk of coronary atherosclerosis and furthermore Ozkan et al. 40 found that procalcitonin can be used as a marker of premature atherosclerosis. In contrast, Bogazzi et al. 41 showed that coronary heart disease risk of in acromegaly was lower than that in subjects without acromegaly. Although our study confirms the finding of increased procalcitonin concentration there was no correlation with cIMT.
GH increases glucose production and inhibits hepatic gluconeogenesis, and excessive GH production leads to compensatory hyperinsulinemia. 42 In the present study, we noted statistically significant differences between subjects with acromegaly and controls for body weight, systolic and diastolic blood pressures, fasting glucose, and LDL concentrations (Table 1).
In conclusion, we found increased serum concentrations of fetuin-a, procalcitonin, and apelin in subjects with acromegaly and positive correlations between apelin and GH, fetuin-A and IGF-1, and procalcitonin and BMI. cIMT was not increased in the subjects with acromegaly despite having higher procalcitonin. We speculate that the higher concentrations of fetuin-A and apelin may play a protective role against cardiovascular disease in subjects with acromegaly.
Footnotes
Acknowledgement
The authors thank Scientific Projects Commission of the Pamukkale University for support.
Declaration of conflicting interests
None declared.
Funding
This study was supported by the Scientific Projects Commission of the Pamukkale University (Grant number: 2011-TPF-045).
Ethical approval
This study was approved by the institutional ethics and research committee of Pamukkale University (2011-034).
Guarantor
ST.
Contributorship
ST: Planning, evaluating, and writing
FA: Planning, evaluating
ST: Hematological observations
GFY: Planning
DH: Radiological analysis
CA: Hematological examinations