
Abstract
We present two cases of spuriously high cerebrospinal fluid glucose concentration with approximately normal blood glucose concentrations. The cause of these abnormal findings was the use of inappropriate collection tubes during the pre-analytical phase. Whilst no patient harm was identified following this error, significant time and effort were expended by both laboratory and clinical staff to explain the cause of these findings.
Keywords
Introduction
Cerebrospinal fluid (CSF) analysis plays an important role in the diagnosis of many infectious and non-infectious medical conditions.1,2
CSF samples must be delivered to the laboratory immediately and should be analysed within 1 h of collection. Routine assessment of CSF includes determination of protein, glucose and lactate concentrations. Red and white blood cell counts, microscopic examination and culture should also be performed. In addition, specific antigen and antibody testing for infectious agents may sometimes be requested. Other tests may be useful depending on the presumptive diagnosis.2,3
CSF is an ultrafiltrate of plasma, and CSF glucose concentration is regulated through facilitated transportation across the blood–brain barrier, with CSF glucose concentrations being proportional to plasma concentrations.4,5 The normal CSF glucose concentration is approximately 50–60% of the blood glucose concentration, ranging from 2.2 to 3.9 mmol/L. 6 Because of this relationship, it is often appropriate to interpret CSF and plasma glucose concentrations simultaneously. CSF glucose concentration, especially low glucose concentrations (representing a CSF/blood glucose ratio lower than 0.4) and increased lactate concentrations are useful in the diagnosis of neurological inflammatory diseases (especially bacterial or fungal meningitis), metastases and disorders with increased CSF cell count. 2
In contrast to a low CSF glucose concentration, the finding of a high CSF glucose concentration has no specific diagnostic significance. High CSF glucose concentration may be observed in patients with high plasma glucose concentrations, such as patients with diabetes. However, even in these conditions, CSF glucose concentrations are not exceptionally increased compared to normal CSF glucose concentrations. In patients with higher plasma glucose, a decreased CSF/blood ratio can be present due to saturation of glucose transport through the haematoencephalic barrier.4,5 However, systemic hyperglycaemia was not present in our cases. Finally, rare cases of extreme glucose concentration due to central line migration into the epidural space or peri-vertebral veins have been reported.7,8
Case 1
Cerebrospinal fluid biochemistry assessment, case 1.
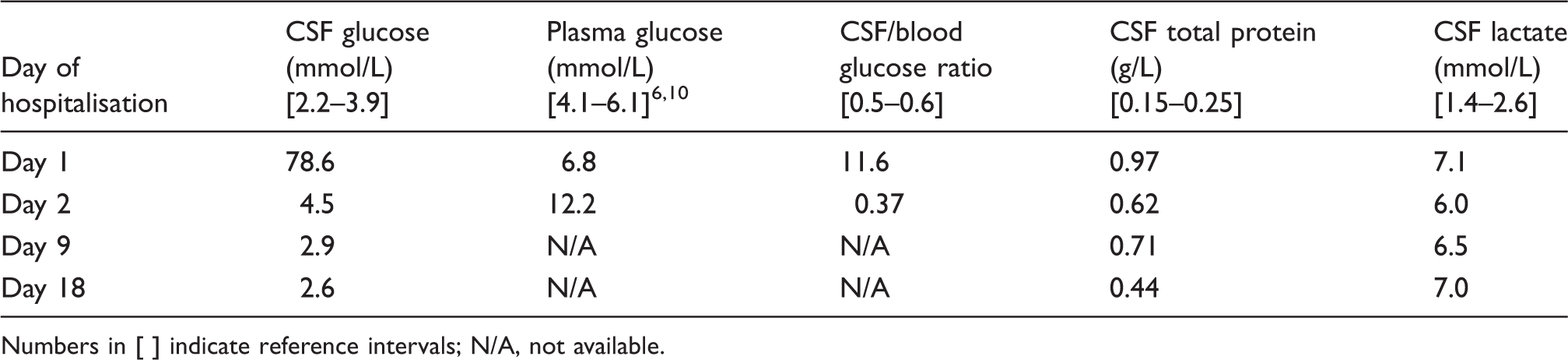
Numbers in [ ] indicate reference intervals; N/A, not available.
Case 2
A 73-year-old man with primary cutaneous large B-cell lymphoma (PCLBCL), leg type, presented with confusion at the Department of Haemato-Oncology at the University Hospital in Pilsen. Enhanced CT of the brain showed no obvious lesions. Initial CSF examination was performed, and May-Grünwald-Giemsa-stained smears showed atypical mononuclear cells (mononuclear cell count 142/µL with absence of polymorphonuclear cells). FACS examination revealed central nervous system infiltration with PCLBCL. Biochemical analysis revealed concentrations of glucose of 1.2 mmol/L, total protein of 1.8 g/L and lactate of 7.6 mmol/L. Repeated lumbar punctures with intra-thecal cytostatic therapy were performed. The response to the therapy was good, CSF element counts gradually decreased and biochemical analysis results on day 13 were almost within the physiological range. However, a high CSF glucose concentration of 54.0 mmol/L was measured on day 20. As described in case 1, CSF glucose concentrations were measured repeatedly using the AU 5800 Clinical Chemistry System (Beckman Coulter, Lismeehan, O’Callaghan’s Mills, Co. Clare, Ireland) and Biosen S Line (EKG diagnostics, Barleben, Germany). Plasma glucose concentration was measured in a sample drawn within 1 h of CSF puncture, with a result of 6.0 mmol/L. The lumbar puncture was not repeated, the condition of the patient improved and the patient was discharged within one month of admission.
Discussion
The findings of such high CSF glucose concentrations in these two patients were both unexpected and improbable and led us to look for the presence of a pre-analytical or analytical error. Investigation revealed that both patients had been treated in the same department and that at the time of lumbar puncture, no intravenous infusions were being undertaken. In both cases, samples for CSF examination were delivered in sterile tubes without additives as recommended. However, we ascertained that CSF samples collected for FACS examination are routinely stored in tubes with 0.2 mL of stabilising solution TransFix/EDTA (Cytomark, Caltag Medsystems Ltd, Buckingham, UK). No information regarding the composition of this stabilising solution is available. We had contacted the Company’s technical support with this issue, but they did not provide an explanation. However, the Company advises against measuring glucose in CSF that has been collected or stored in these tubes, even though this caveat is not contained within any product information leaflet. The information that is provided clearly states that the containers’ intended use is in the stabilisation of CSF leukocytes for subsequent cytometric analysis. We undertook a search for reports relating to glucose-containing tubes used for CSF collection, but we were unable to find any. Nevertheless, we suspected that CSF from these two patients had been contaminated by a solution containing a high concentration of glucose. A tube containing undiluted stabilising solution was subsequently obtained and analysed. Because a high glucose concentration in the stabilising solution was presumed, a small volume of stabilising solution was diluted using distilled water (0.05 mL of stabilising solution was diluted using 5.0 mL of distilled water). The glucose concentration was tested using two analysers, which utilised the same principle of glucose determination outlined above. On average, the glucose concentration in the stabilising solution was 2031.5 mmol/L. In addition, to exclude the possibility of analytical error, the stabilising solution was analysed using a gas chromatography (GC)/mass spectrometry method (Agilent 6890N Network GC System, 5973 Network Mass Selective Detector, CA, USA) as described previously. 11 The glucose concentration was determined to be 1989.9 mmol/L.
The most likely explanation for the exceptionally high glucose concentration observed in these CSF samples is that they were collected into tubes containing stabilising solution with a high glucose concentration. Once contaminated, they may then have been transferred to sterile tubes (with no additives) for biochemical and cytological analyses. These findings illustrate the importance of users complying with laboratory guidance for sample collection and storage. Failure to comply with such guidance can have a significant adverse impact on the analytical phase. In these two cases, fortunately, no adverse incidents arose due to the error, although significant time and effort were spent by healthcare professionals to explain the findings. In conclusion, CSF samples from wards using special tubes for FACS analysis can potentially be contaminated with glucose and should therefore not be used for CSF glucose analysis.
Footnotes
Declaration of conflicting interests
None declared.
Funding
Supported by the Ministry of Health, Czech Republic – Conceptual Development of Research Organisation (University Hospital in Pilsen – FNPl, 00669806).
Ethical approval
Not applicable.
Guarantor
JR.
Contributions
PB wrote manuscript and is responsible for concept and design, data collection and interpretation of data. DR was involved in concept and design, data collection and interpretation of data. JR was involved in concept, design and interpretation. LV is co-responsible for the analysis and data collection. TP is co-responsible for the analysis. All authors reviewed and approved the final version of the manuscript.