
Abstract
Background
Plasma betaine concentrations and urinary betaine excretions have high test-retest reliability. Abnormal betaine excretion is common in diabetes. We aimed to confirm the individuality of plasma betaine and urinary betaine excretion in an overweight population with type 2 diabetes and compare this with the individuality of other osmolytes, one-carbon metabolites and trimethylamine-N-oxide (TMAO), thus assessing their potential usefulness as disease markers.
Methods
Urine and plasma were collected from overweight subjects with type 2 diabetes at four time points over a two-year period. We measured the concentrations of the osmolytes: betaine, glycerophosphorylcholine (GPC) and taurine, as well as TMAO, and the one-carbon metabolites, N,N-dimethylglycine (DMG) and free choline. Samples were measured using tandem mass spectrometry (LC-MS/MS).
Results
Betaine showed a high degree of individuality (or test-retest reliability) in the plasma (index of individuality = 0.52) and urine (index of individuality = 0.45). Betaine in the plasma had positive and negative log-normal reference change values (RCVs) of 54% and −35%, respectively. The other osmolytes, taurine and GPC were more variable in the plasma of individuals compared to the urine. DMG and choline showed high individuality in the plasma and urine. TMAO was highly variable in the plasma and urine (log-normal RCVs ranging from 403% to −80% in plasma).
Conclusions
Betaine is highly individual in overweight people with diabetes. Betaine, its metabolite DMG, and precursor choline showed more reliability than the osmolytes, GPC and taurine. The low reliability of TMAO suggests that a single TMAO measurement has low diagnostic value.
Keywords
Introduction
Betaine (N,N,N-trimethylglycine, glycine betaine, TMG) is an important osmolyte which is also involved in one-carbon metabolism as a major source of methyl groups in mammals. 1 Betaine can be obtained from the diet 2 or produced in the body by oxidation of choline. Choline is predominantly present in the diet and the body in the form of phosphatidylcholine. 3 Urinary betaine excretion is often elevated in diabetes and renal failure.4,5 Plasma betaine concentrations and urinary betaine excretions can predict secondary cardiovascular events in people with established vascular disease, 6 and the plasma concentration of dimethylglycine, the product of betaine metabolism, is an especially strong prognostic marker.6,7 These predictions are stronger for patients with diabetes. It is therefore important to know how much value can be attached to single measurements of these metabolites. Reference change values (RCVs) are useful to show a change over successive measurements that cannot be attributed to either analytical imprecision or biological variation. Betaine has been shown to have a high reliability in the plasma and urine of healthy young males over the period of a day, and over eight weeks. 8 A high reliability (or individuality) of urine betaine excretion has been reported in subjects with stable angina over a few years, 5 and plasma betaine concentrations were found to be consistent in a small sample of normal subjects over a similar time. 9 It is not known if the high reliability which has been observed for betaine is related to its role in one-carbon metabolism, or its role as an osmolyte.
The objective of this study was to investigate the individuality (using the index of individuality) and test-retest reliability (using the coefficient of reliability) of plasma and urine betaine concentrations in a group of overweight people with type 2 diabetes over a two-year period and compare these data with some related compounds. The other one-carbon metabolites, N,N-dimethylglycine (DMG) and choline were measured. Trimethylamine-N-oxide (TMAO) is another methylamine which has been associated with cardiovascular risk. 10 Wang et al. 11 showed that high plasma and choline concentrations were associated with a higher risk of major adverse cardiac events when plasma TMAO is also elevated. We therefore included TMAO in this study to investigate the usefulness of a single measurement as a diagnostic marker in type 2 diabetes. Since betaine is an important osmolyte, we also investigated the test-retest reliability of two other osmolytes, taurine and glycerophosphorylcholine (GPC).
Methods
Study design
Characteristics of the study population.
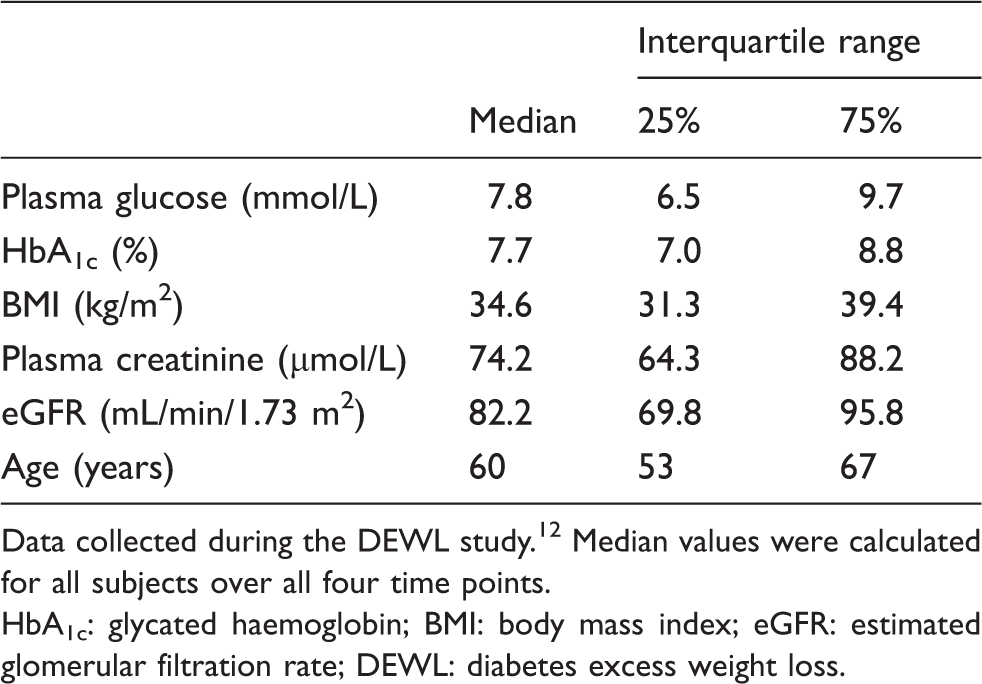
Data collected during the DEWL study. 12 Median values were calculated for all subjects over all four time points.
HbA1c: glycated haemoglobin; BMI: body mass index; eGFR: estimated glomerular filtration rate; DEWL: diabetes excess weight loss.
Reagents and chemicals
Glycine betaine (HCl), DMG (HCl), choline (iodide), GPC (cadmium chloride complex), TMAO (dihydrate) and taurine were obtained from Sigma (St Louis, MO, USA). N,N,N-Trimethyl-D9-glycine (HCl) (D9-betaine) and choline-trimethyl-D9 (chloride) were obtained from Isotec (Miamisburg, OH, USA), D9-TMAO was obtained from Cambridge Isotope Laboratories (Andover, MA, USA) and N,N-dimethyl-D3-glycine (HCl) and 2-aminoethane-D4-sulfonic acid (deuterated taurine) were obtained from CDN isotopes (Pointe-Claire, Quebec, Canada). Ammonium formate and formic acid were purchased from Sigma-Aldrich (St Louis, MO, USA). High-performance liquid chromatography (HPLC)-grade acetonitrile was obtained from Mallinckrodt (Paris, KY, USA), and methanol was obtained from Merck (Darmstadt, Germany).
Sample analysis
Mass transitions and voltages used in the mass spectrometry methods.
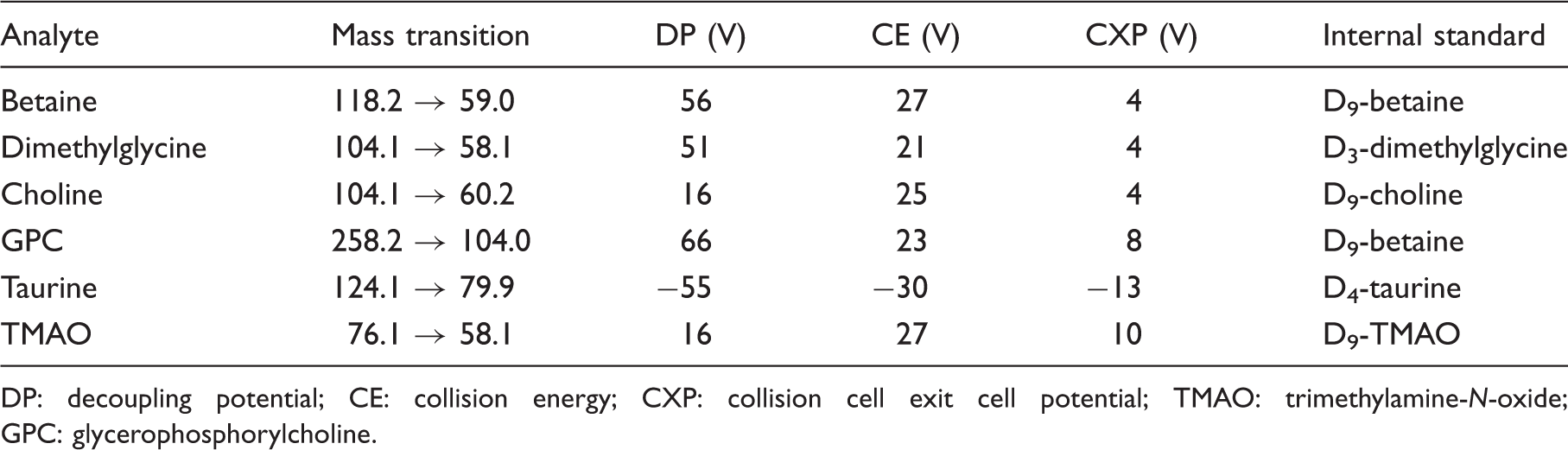
DP: decoupling potential; CE: collision energy; CXP: collision cell exit cell potential; TMAO: trimethylamine-N-oxide; GPC: glycerophosphorylcholine.
Taurine was separated isocratically using an XBridge amide column (100 × 2.1 mm, 3.5 µm, Waters, USA). The mobile phase contained 20% water and 80% acetonitrile, the flow rate was of 0.3 mL/min, the injection volume was 10 µL and the oven temperature was 40℃. Taurine was measured in negative ion mode.
Urine creatinine was measured during the DEWL study on routine analysers at three locations in New Zealand using the Jaffè method. eGFR was calculated using the abbreviated modification of diet in renal disease (MDRD) equation. 17
Statistical analysis
Statistical analyses were performed using SigmaPlot (Version 11.2). Differences between the subjects were investigated for the analytes in the urine and plasma using one-way repeated measures analysis of variance. Mann–Whitney rank sum tests were used to test for differences in metabolite concentrations between the dietary treatments, and between the genders. A P value <0.05 was considered to be statistically significant. The within-individual variation over the four time points was also investigated. The index of individuality was also calculated for each compound, where a lower number represents higher individuality of the data. The index of individuality was calculated as the ratio of within-subject coefficient of variation (CVi) to between-subject coefficient of variation (CVg). CVi was calculated using the formula CVi = (CVt2–CVa2)½, where CVt is the total imprecision and CVa is the analytical imprecision.
The test-retest reliability of the results was also determined by calculating the coefficient of reliability (Cronbach’s α) in order to compare the data with those from previous studies. Coefficient of reliability = (N / (N−1)) ((total variance − sum of individual variance) / total variance), where N is the number of subjects. Because of the non-normal distribution in urine, the coefficient of reliability was calculated for log-transformed data. A reliability coefficient close to 1 represents a high degree of test-test reliability, 18 whereas a coefficient of zero corresponds to random data (no consistency). A coefficient of reliability was calculated for each compound using only subjects where there was a complete set of four time points (baseline, 6 months, 12 months and 24 months).
Log-normal RCVs for a positive and negative change were calculated as described by Fraser 19 using the equation RCVpos = [exp(1.96 × 2½ × σ) − 1] × 100, and RCVneg = [exp(−1.96 × 2½ × σ) − 1] × 100, where σ is the log-normal distribution defined as σ = [ln(CVt2 + 1)]½, and CVt is the total imprecision. A Z-score of 1.96 was used to calculate RCVs, corresponding to P = 0.05, or a 95% chance that a change is significant.
Results
Quality control
The analytical coefficients of variation throughout the study were generally below 7% for betaine, DMG, choline, taurine and TMAO. However, GPC had a greater analytical CV of 21% in the plasma, which may be a consequence of lack of a suitable commercially available internal standard. The concentrations of GPC in the samples were also closer to the detection limits than the other analytes.
Effect of diet
No significant differences (P < 0.05) in the concentrations of betaine, DMG, choline, taurine, GPC or TMAO were observed between the diet treatments for both plasma and urine.
Gender differences
There were significant differences observed between the genders. Males had significantly higher (P < 0.01) plasma betaine, DMG and choline. Plasma concentrations of TMAO, GPC and acetylcarnitine were not significantly different between the genders. There were no significant gender differences detected for any metabolites in the urine.
Individuality
The test-retest reliability and individuality in plasma.
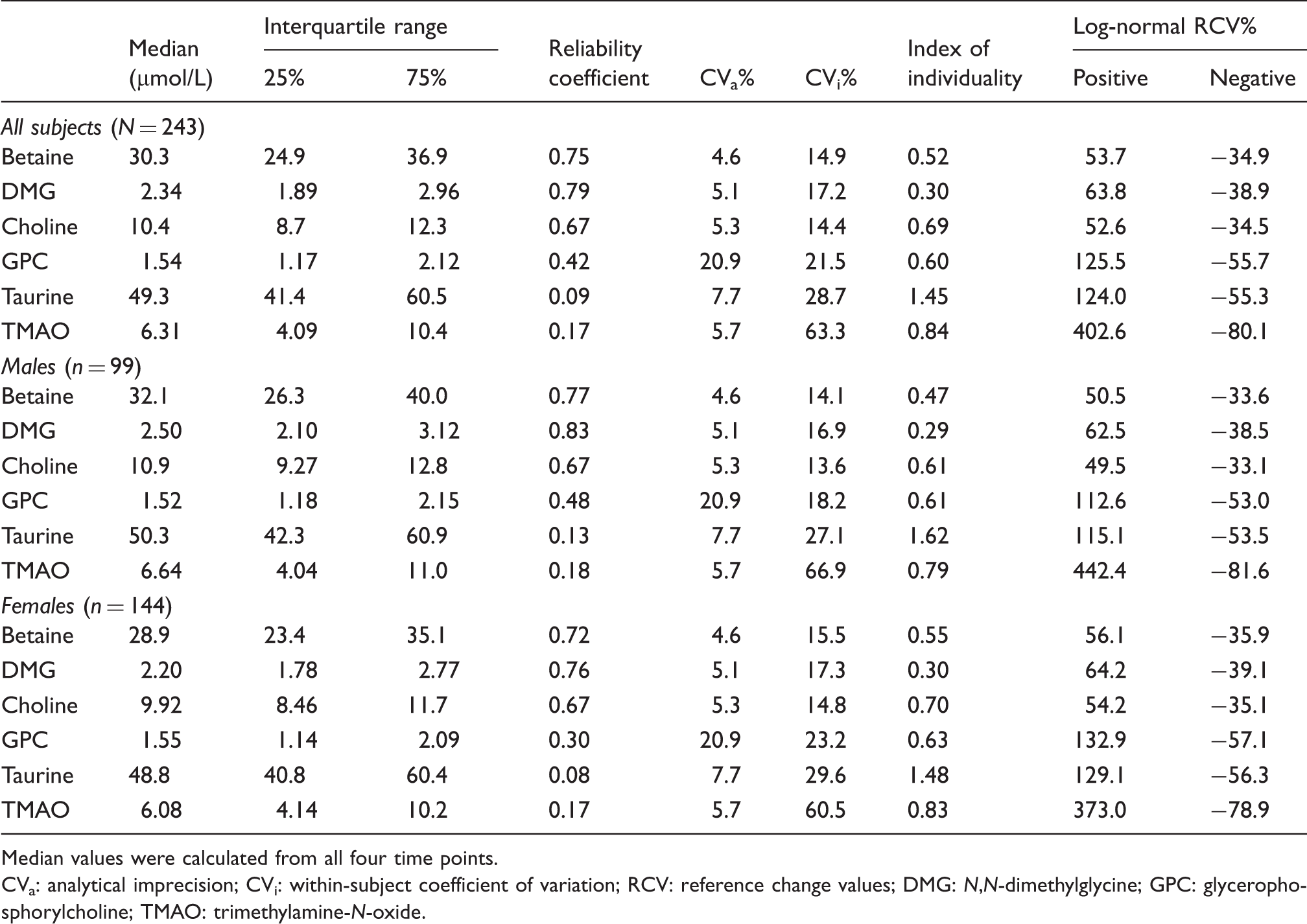
Median values were calculated from all four time points.
CVa: analytical imprecision; CVi: within-subject coefficient of variation; RCV: reference change values; DMG: N,N-dimethylglycine; GPC: glycerophosphorylcholine; TMAO: trimethylamine-N-oxide.
The test-retest reliability and individuality in urine.
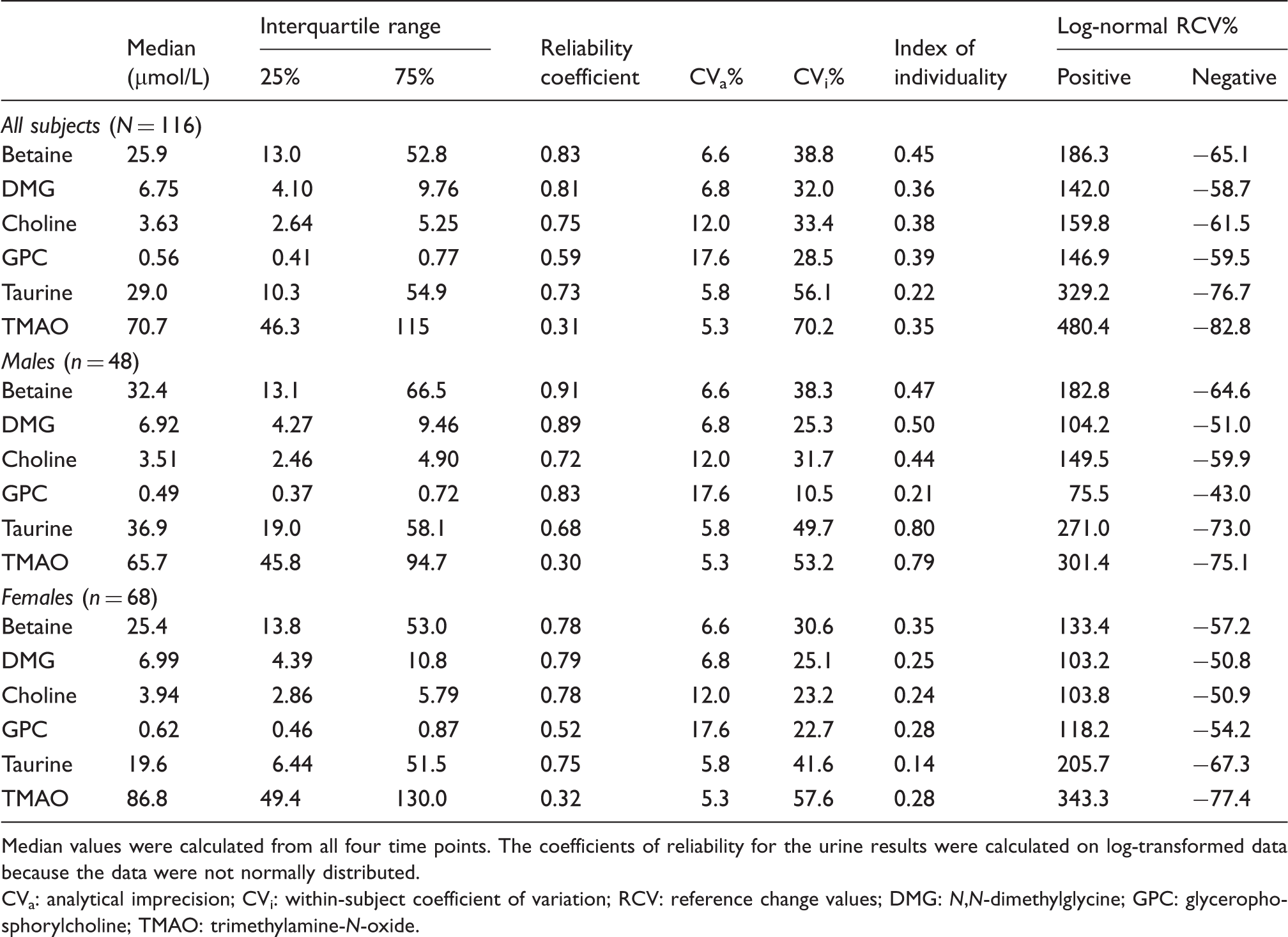
Median values were calculated from all four time points. The coefficients of reliability for the urine results were calculated on log-transformed data because the data were not normally distributed.
CVa: analytical imprecision; CVi: within-subject coefficient of variation; RCV: reference change values; DMG: N,N-dimethylglycine; GPC: glycerophosphorylcholine; TMAO: trimethylamine-N-oxide.
The results show that there is a high degree of reliability for betaine (coefficient of reliability (coefficient) = 0.75) and DMG (coefficient = 0.79) in the plasma. Of all the analytes investigated, betaine (coefficient = 0.83) and DMG (coefficient = 0.81) concentrations showed the highest degree of reliability in the urine.
While betaine showed a high level of individuality in the plasma and urine, the other osmolytes were more variable. GPC had a moderate degree of reliability in the plasma (coefficient = 0.42) and urine (coefficient = 0.59). Taurine was much more variable in the plasma (coefficient = 0.09) than in the urine (coefficient = 0.73).
Choline concentrations showed a moderate reliability in the plasma (coefficient = 0.67) and in the urine (coefficient = 0.75). TMAO had a low reliability in both the plasma (coefficient = 0.17) and the urine (coefficient = 0.31).
The indices of individuality show similar trends for the metabolites. A smaller number for the index of individuality indicates low within-individual variability (high individuality). Plasma taurine had a particularly high index, representing a low individuality. GPC and TMAO in the plasma also had high indices of individuality of 0.60 and 0.84, respectively.
The RCVs were much lower in the plasma than the urine for all analytes. A change in plasma betaine concentration of +51% (or −34%) in males and +56% (or −36%) in females can be considered significant (P < 0.05). A change in plasma DMG concentrations of +64% (−39%) is significant (P < 0.05). However, a change in plasma TMAO of +403% (or −80%) and a change of plasma taurine of +124% (or −55%) is required to be significant (P = 0.05). Larger log-normal RCV ranges were observed for urine metabolite excretions compared to the plasma. For example, urine betaine had a positive log-normal RCV of 186 and a negative log-normal RCV value of −65 over both genders. TMAO had the highest RCVs in the urine of +480% (or −83%) over both genders.
Discussion
Effect of diet
No significant differences in metabolite concentrations were observed between the high protein and high carbohydrate diets, which is surprising considering the high betaine content of many high carbohydrate foods, such as wheat-based cereal products. 2 However, this observation is likely to be at least partially a result of deviations the DEWL study participants may have made from their prescribed diets. 12
Comparison of the DEWL study group with other studies
Comparison of DEWL data with other studies.
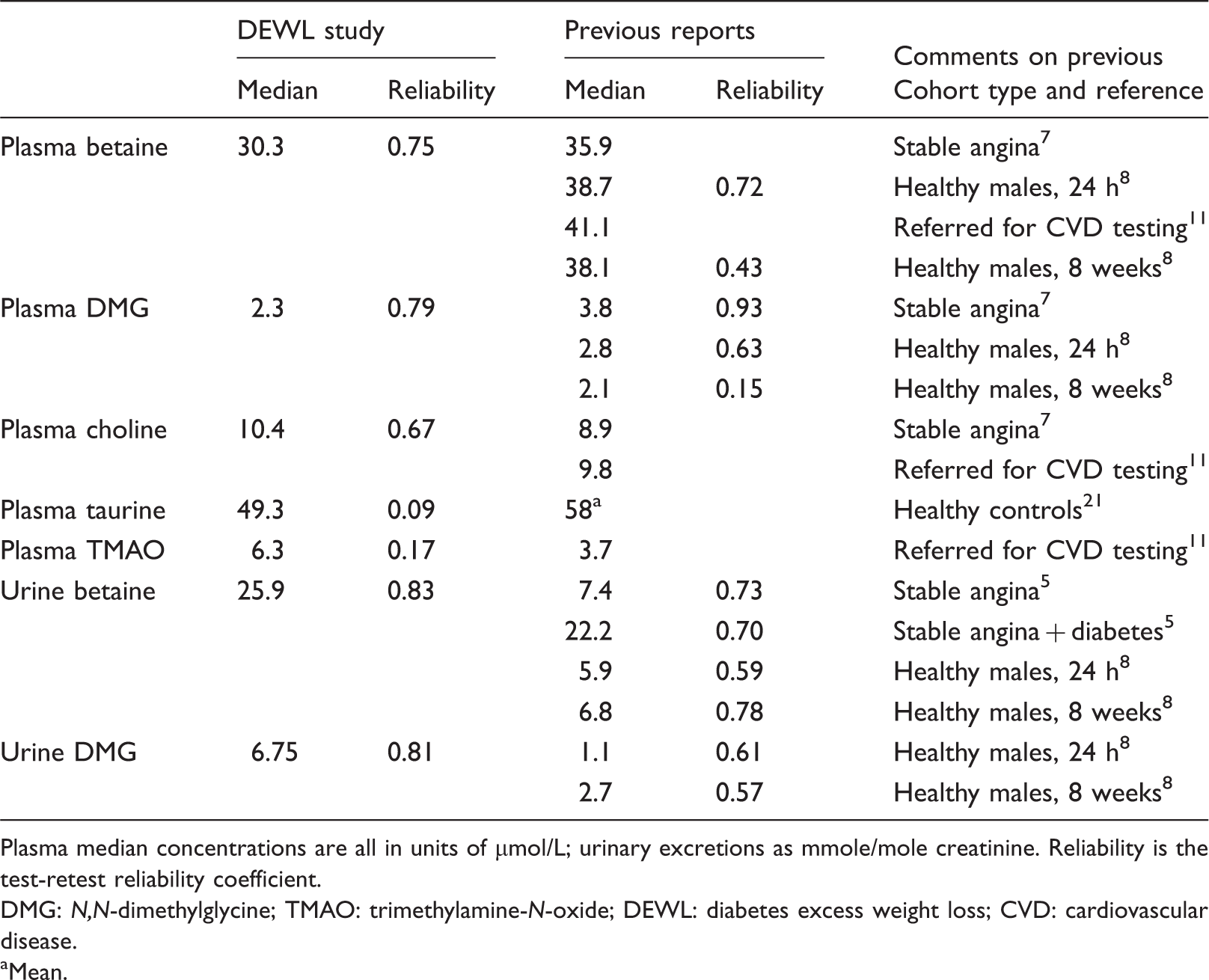
Plasma median concentrations are all in units of µmol/L; urinary excretions as mmole/mole creatinine. Reliability is the test-retest reliability coefficient.
DMG: N,N-dimethylglycine; TMAO: trimethylamine-N-oxide; DEWL: diabetes excess weight loss; CVD: cardiovascular disease.
Mean.
Plasma choline concentrations (overall median 10.4 µmol/L) in the overweight subjects with diabetes were consistent with data on the general population. 24 Cardiovascular events such as myocardial infarction have been associated with high plasma choline concentrations, though the event probably causes the elevation. Plasma choline concentrations ≥25 µmol/L have been reported to be predictive of major cardiac events. 24 The mean plasma taurine concentration of 53.5 µmol/L observed for the DEWL study samples is in good agreement with Laidlaw et al., 21 who published a mean value (±SD) of 58 ± 16 µmol/L in apparently healthy subjects. There are few reports published on the osmolyte GPC, especially in diabetes, so it is difficult to compare the results with other studies. However, the present study shows that the concentrations of GPC in plasma and urine of overweight people with diabetes are considerably lower than the other osmolytes, betaine and taurine. This could be expected because GPC is synthesised intracellularly in response to osmotic stress, rather than accumulated by active transport from the circulation. 25
Individuality
The results of the present study are consistent with the high coefficient of reliability of 0.73 which was reported for urine betaine concentrations by Schartum-Hansen et al. 5 in a population with coronary artery disease; the coefficient in the subgroup with diabetes was similar (0.70) despite a much higher median excretion in this group. 5 The present study found an even higher coefficient of reliability of 0.83 for urine betaine (0.91 in the males). The main difference in these populations is that the present study investigated people with diabetes who were overweight, whereas Schartum-Hansen et al. 5 investigated a larger group of cardiovascular patients that included a significant minority with diabetes. A high reliability of betaine in the plasma and urine was also reported by Lever et al.8,9 in healthy subjects. The coefficients observed for people with type 2 diabetes in the present study are generally consistent with those of Lever et al. 8 Urinary DMG excretion may have slightly lower individuality than betaine, and free choline lower still.
Plasma dimethylglycine is much more individual in this population than in a small group of healthy young males, 8 and these values can be expected to be population dependent. Svingen et al. 7 also reported a high coefficient of reliability (0.93) for plasma DMG in people with stable angina. Plasma DMG was also shown to be predictive of secondary cardiovascular events, 7 which is in agreement with the findings of Lever et al. 6 The predictive value of single measurements of plasma DMG is not just a reflection of its correlation with homocysteine, 7 and as noted before, it could be expected that changes in plasma DMG with time may be a useful additional tool in patient management, and this should be investigated.
The other osmolytes, GPC and taurine showed less test-test reliability in the plasma than betaine. The moderately high individuality and low RCVs suggest that plasma choline may be useful as an indicator of cardiovascular risk in this population. The high variability in plasma taurine (index of individuality = 1.45) observed here suggests that fluctuations in diabetic control and changes in the osmotic status in the body may be having an effect. However, taurine was more individual in the urine in this population (index of individuality = 0.22). Plasma GPC concentrations showed moderate individuality (index of individuality = 0.60) in this population.
The plasma TMAO concentrations were highly variable in this study group. Plasma TMAO has been promoted as a predictive marker of cardiovascular disease. 10 However, in the DEWL study group, both plasma concentrations and urinary excretion of TMAO are highly variable. TMAO concentrations are especially affected by the dietary intake of marine foods. TMAO is an osmolyte in many marine animals, but not a mammalian osmolyte, and is often a marker of eating fish. TMAO concentrations are also raised in people on high choline diets or taking lecithin, betaine or carnitine supplements. 26 Elevated plasma concentration TMAO has been previously proposed as a maker of renal disease.27,28 The high intraindividual variability for TMAO concentrations observed in this population may make it difficult to make clinical decisions on the basis of a single measurement.
A limitation on this study is that most subjects lost weight during it, 12 and the dietary changes may be expected to affect the handling of some metabolites. This makes the high level of consistencies reported here more remarkable, and we may have underestimated the individuality of some of those we studied. However, we have sought trends for changes with treatment and time and have found none that approach statistical significance.
Conclusions
The high test-retest reliability of betaine in this study group shows that the disruption of osmolytes by diabetes has little effect on within-individual reproducibility. This indicates that betaine concentrations are likely to be homeostatically controlled by one-carbon metabolism, even in diabetes. Betaine concentrations measured at any given time provide information about the betaine status of each individual. Other one-carbon metabolites (choline and DMG) also had high test-retest reliability in the urine and plasma. The other osmolytes: GPC and taurine were considerably more variable than betaine, meaning single measurements are likely to be of limited clinical use. The low individuality observed for plasma and urine TMAO in this study may cast some doubt on its value as a disease marker (at least in this population) despite evidence for its association with vascular disease,10,11 and may be related to the consumption of seafood.
Footnotes
Acknowledgements
The authors thank the DEWL study team for allowing the use of the DEWL study samples in the present study.
Declaration of conflicting interests
None declared.
Funding
The DEWL study was funded by the Health Research Council of New Zealand (06/337). The authors also acknowledge support from the National Heart Foundation of New Zealand and the Maurice and Phyllis Paykel Trust and made use of equipment funded by New Zealand Lottery Health Research.
Ethical approval
Ethical approval was obtained to measure betaine and related metabolites in the DEWL study samples from the Multi-region Ethics Committee of New Zealand (MEC/06/08/081).
Guarantor
SC.
Contributorship
JDK and HL were involved with designing and carrying out the DEWL study. JDK obtained ethical approval. CJM carried out measurements for betaine and related compounds on the study samples. CMF advised on the statistical analysis. All authors contributed to and edited the manuscript.