
Abstract
Objective
Serum and synovial fluid (SF) chemokine ligand 2 (CCL2)/monocyte chemoattractant protein 1 (MCP-1) concentrations have been identified to be increased in osteoarthritis (OA) patients. The scope of this study was to examine CCL2 concentrations in serum and SF of knee OA patients and to explore their association with patient-reported symptomatic severity.
Method
One hundred and sixty-one knee OA patients and 138 healthy controls were enrolled into the study from our hospital. We collected Western Ontario and McMaster Universities Arthritis Index (WOMAC) scores from OA patients and measured CCL2 concentrations in serum and SF using enzyme-linked immunosorbent assay method, and correlation between WOMAC scores and CCL2 concentrations were analysed.
Results
CCL2 concentrations in SF instead of serum were independently and positively associated with self-reported greater pain (r = 0.460, P < 0.001) and physical disability (r = 0.561, P < 0.001) in OA patients.
Conclusion
CCL2 in SF might serve as a novel and reliable biomarker for assessing symptomatic severity of OA.
Introduction
Osteoarthritis (OA) is the most frequent chronic joint disease characterized by slow progressive degeneration of articular cartilage, subchondral bone alteration, secondary synovial inflammation and marked osteophyte formation. 1 The knee is the most commonly affected joint, and knee OA is a leading cause of disability in the elderly population.2,3 It is expected that the morbidity of OA would increase by 40% by 2025 through the continued aging of the population and the obesity epidemic trend. 4 The increased number of people suffering from knee OA in recent years impelled the need for accurate diagnosis of early OA. Recently, non-invasive biomarkers represent a potential non-radiographical alternative to detect early OA and to assess disease severity.
Chemokines are a family of small proteins that guide cell migration into sites of inflammation. On the basis of conserved cysteine motifs, chemokines are divided into C, CC, CXC and CX3C groups. 5 Previous studies have demonstrated that chemokines are associated with various arthritis including knee OA.6,7 Chemokine ligand 2 (CCL2), the ligand of C-C chemokine receptor-2 (CCR2), is chemotactic for monocyte/macrophages and activated T cells.8,9 Increased concentrations of CCL2 are detected in the blood, synovial fluid (SF) and synovial tissue in patients suffering from OA. 10 Injection of CCL2 into rabbit joints cause marked macrophage migration into the affected joint, 11 and treatment with CCL2 antagonist prior to disease onset in arthritis mouse model could prevent the onset of arthritis. 12 Studies have also shown CCL2 could induce pain-related behaviours in rodents.13–15 Since CCL2 is present in the osteoarthritic joint, it may serve as potential pain mediator in OA. Besides, recent studies have demonstrated that CCL2 increases vascular cell adhesion molecule 1 (VCAM-1) expression in human OA synovial fibroblasts via a cascade of signalling pathways, and CCL2-induced VCAM-1 expression promoted monocyte adhesion to human OA synovial fibroblasts. 16 These data suggest that CCL2 may play crucial roles during OA pathogenesis and progression or may even be important in OA symptomatology. However, there have been no studies illustrating the relationship between serum and SF concentrations of CCL2 and the symptomatic severity of OA. Therefore, the current study was designed to assess whether serum or SF concentrations of CCL2 are correlated with the symptomatic severity of the disease.
Materials and methods
Study subjects
One hundred and sixty-one knee OA patients undergoing diagnostic or therapeutic knee hyaluronic acid injection in the Dong Ying People’s Hospital from February 2012 to January 2014 were enrolled in this study. Knee OA were diagnosed according to the American College of Rheumatology. 17 One hundred and thirty-eight sex- and age-matched healthy volunteers receiving regular physical examination in outpatients from our hospital were enrolled as controls. Participants were excluded from the study if they had systemic inflammatory or autoimmune disease, post-traumatic OA, history of knee joint infection, diabetes, gout, malignant disease or other factors causing inflammation of knee joint. All the volunteers had no clinical and radiological manifestations of OA. Written informed consent was obtained from all participants. The research programme was approved by our hospital.
Laboratory methods
Venous blood samples collected from all participants were centrifuged, and serum was stored immediately at −80℃ until analysis. SF samples were collected from the affected knee of the patients with OA before first hyaluronic acid injection. The specimen was then centrifuged to remove cells and joint debris and stored at −80℃ for further measurement. The serum and SF samples were analysed for CCL2 using commercially available enzyme-linked immunosorbent assay (ELISA; R&D Systems Inc., Minneapolis, MN, USA). Two samples of low and high serum and SF concentration were measured six times in a row to calculate the intra-assay coefficient of variation (CV); then two samples of low and high concentrations of serum and SF samples measured were assayed two times a day for three days to calculate inter-assay coefficients of variation. The intra-assay CV and inter-assay CV of the ELISA kits were <5% and <10%, respectively. The recovery of spiked standard in serum was 98%. All the samples were routinely analysed by ELISA in triplicate, and the results were averaged.
Definition of disease severity
The symptomatic severity of the disease was assessed using the Western Ontario and McMaster University Osteoarthritis Index (WOMAC) score. 18 The index comprised three items: pain, stiffness and physical function. The subscales were scored in the range of 0–4 point, where 0 indicates no pain, no stiffness or no difficulty with physical function, and higher scores represent more serious pain, greater stiffness or poorer function. This scale is very broadly used, and the reliability and validity have been well established in OA population. 19 The radiographic severity of OA was classified according to the Kellgren–Lawrence (K–L) grading scale assessed by our experienced radiologist. 20
Statistical analysis
Statistical analysis was implemented utilizing the statistical package for social sciences (SPSS) software, version 21.0 for Windows. The data are expressed as mean ± SD or median (interquartile range). Data normality was analysed using Kolmogorov–Smirnov test. Demographic data between patients and controls were compared by Chi-square tests, unpaired Student’s t-tests or Mann–Whitney U test, as depends. The Spearman rank correlation coefficient and multivariate linear regression analyses were performed to assess the correlation between CCL2 concentrations and WOMAC scores and K–L grading system. Statistical significance was defined as P < 0.05.
Results
Baseline characteristics
Baseline characteristics.
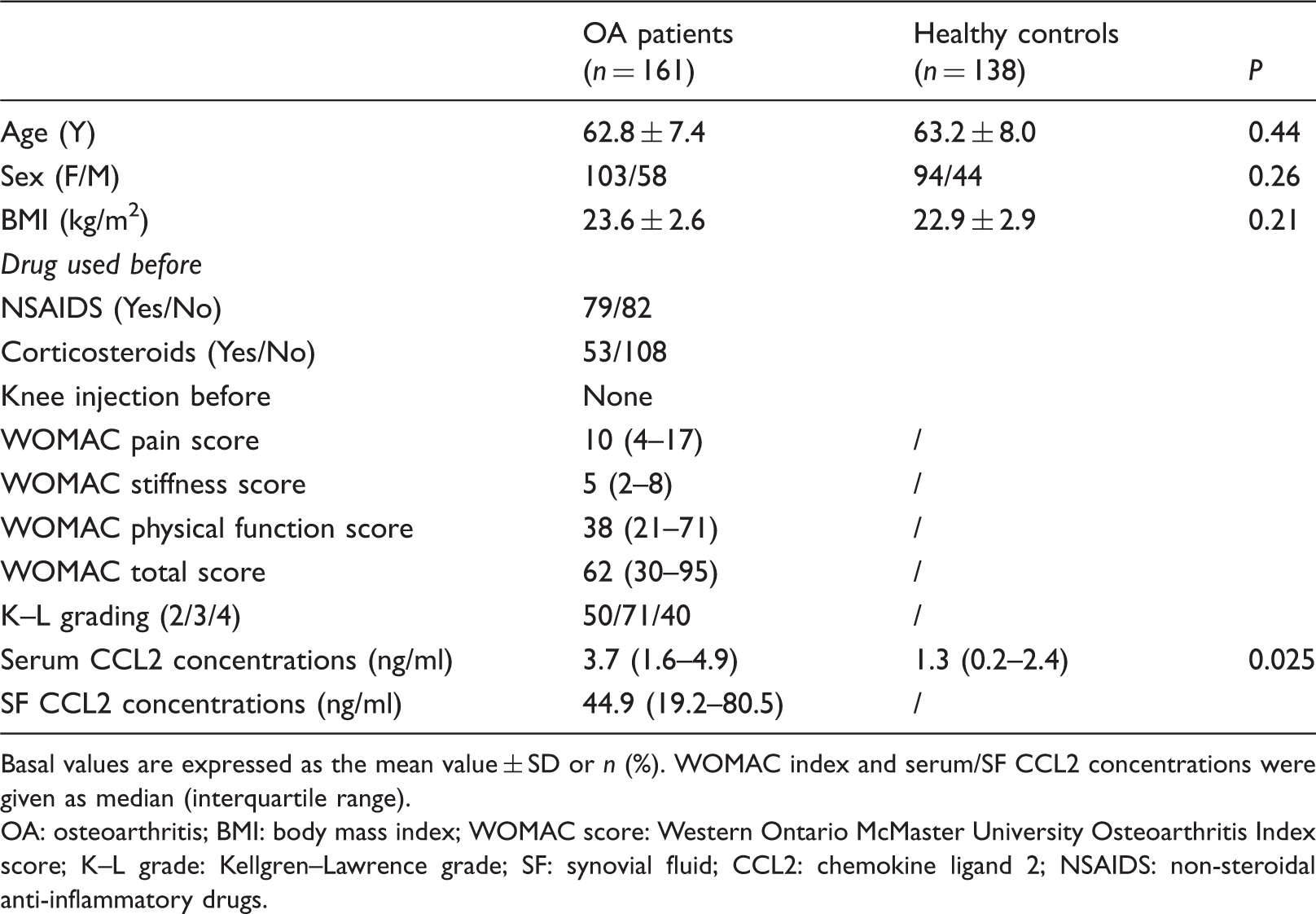
Basal values are expressed as the mean value ± SD or n (%). WOMAC index and serum/SF CCL2 concentrations were given as median (interquartile range).
OA: osteoarthritis; BMI: body mass index; WOMAC score: Western Ontario McMaster University Osteoarthritis Index score; K–L grade: Kellgren–Lawrence grade; SF: synovial fluid; CCL2: chemokine ligand 2; NSAIDS: non-steroidal anti-inflammatory drugs.
Association of CCL2 concentrations with WOMAC scores and K–L grades
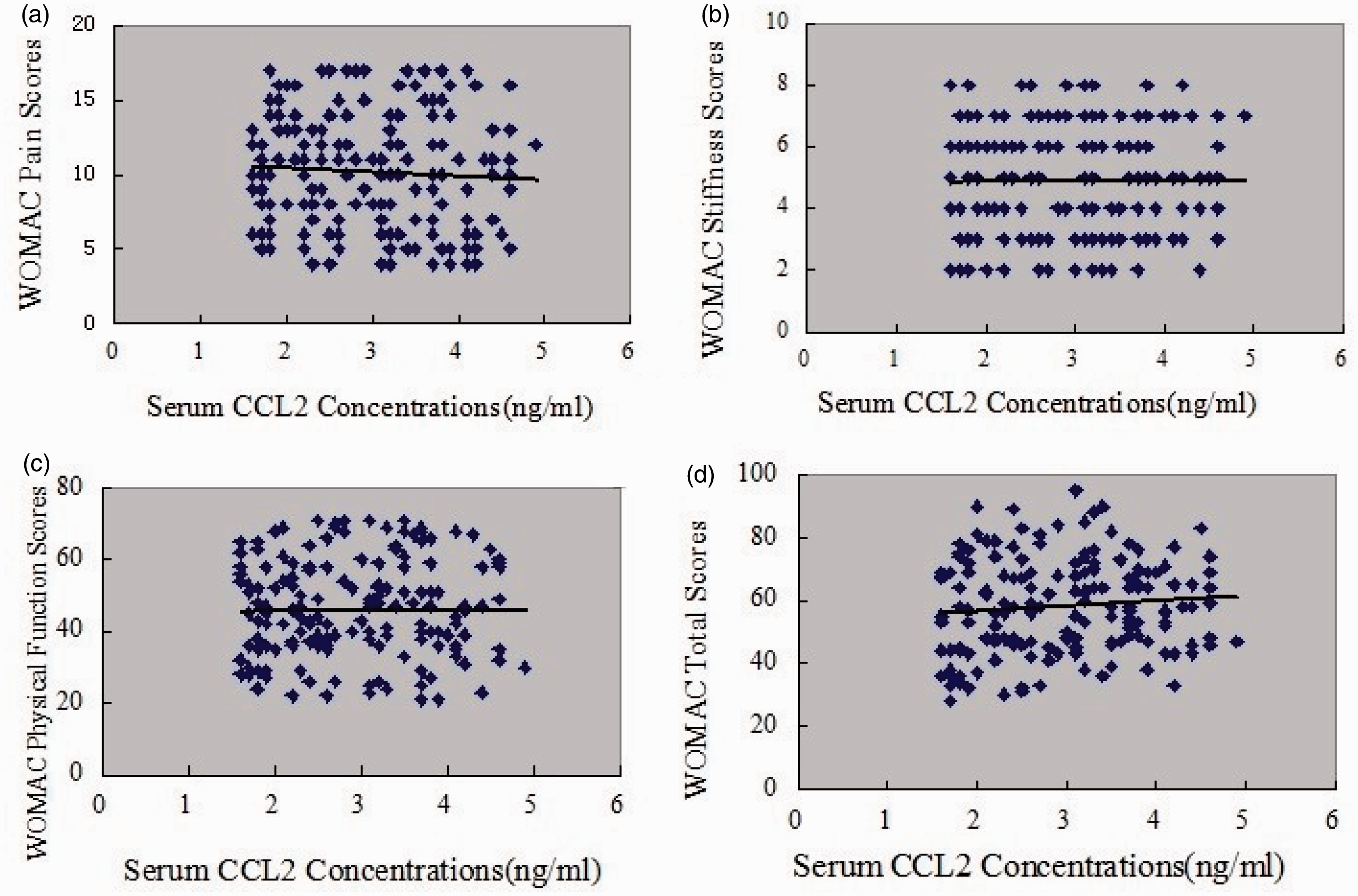
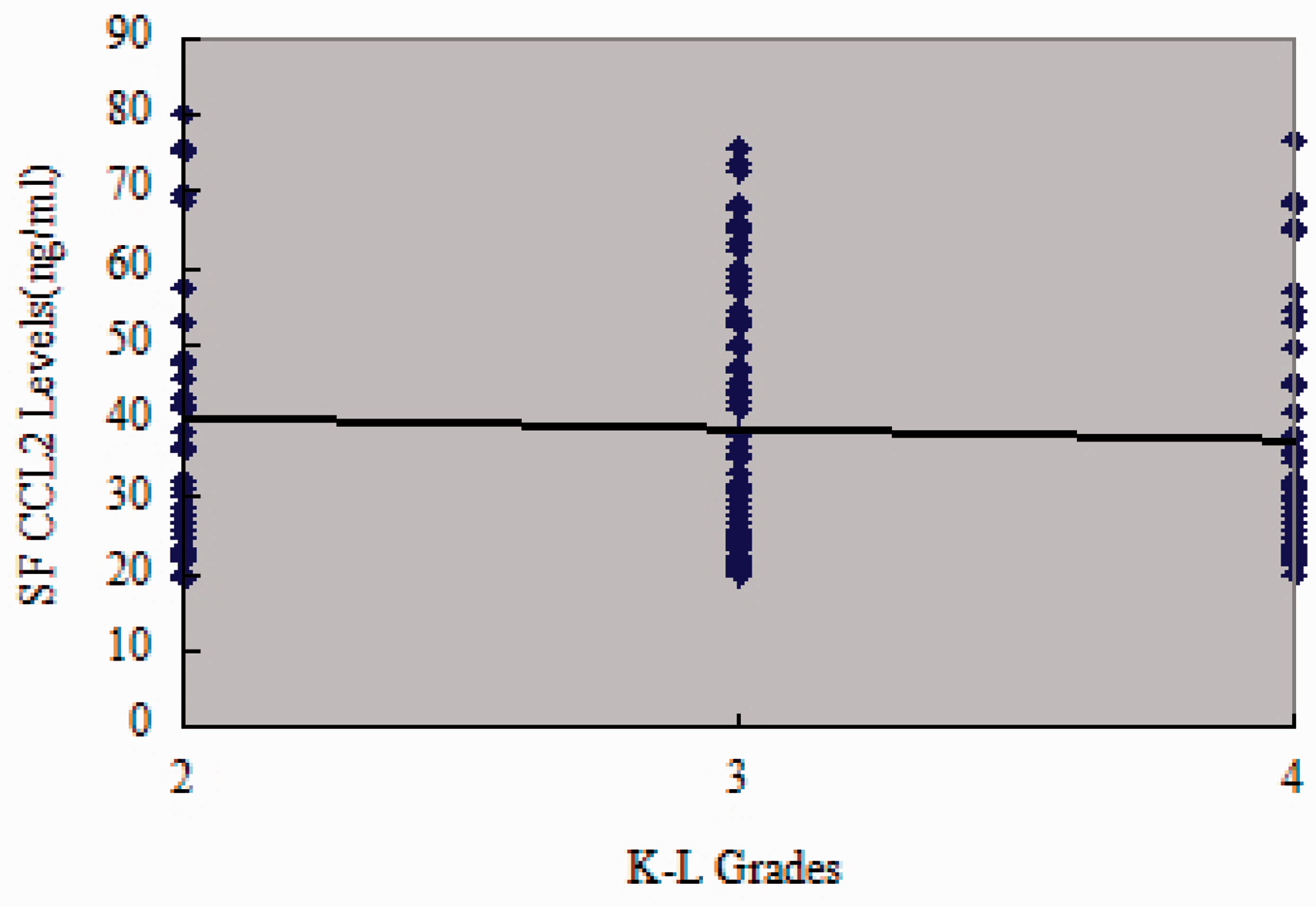
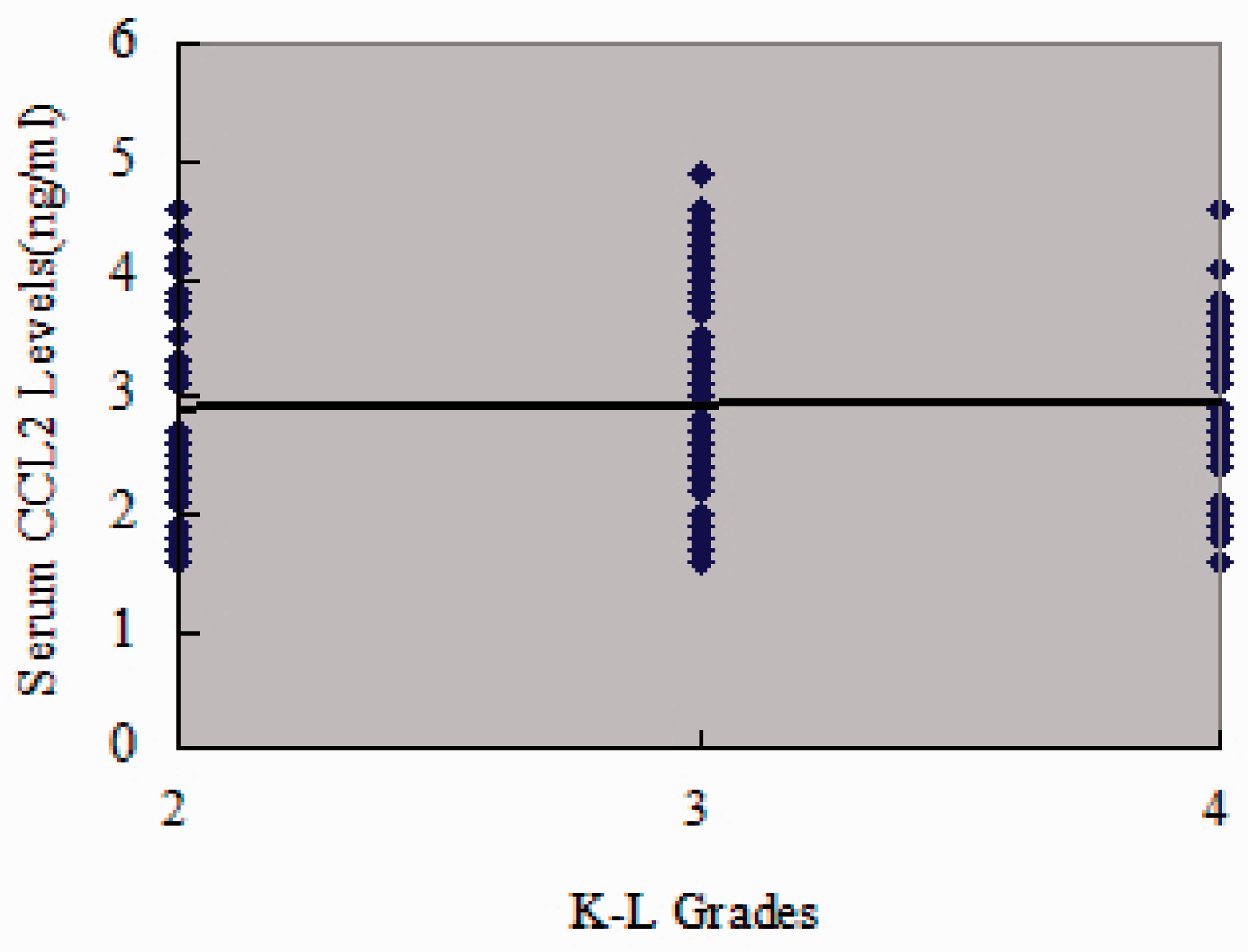
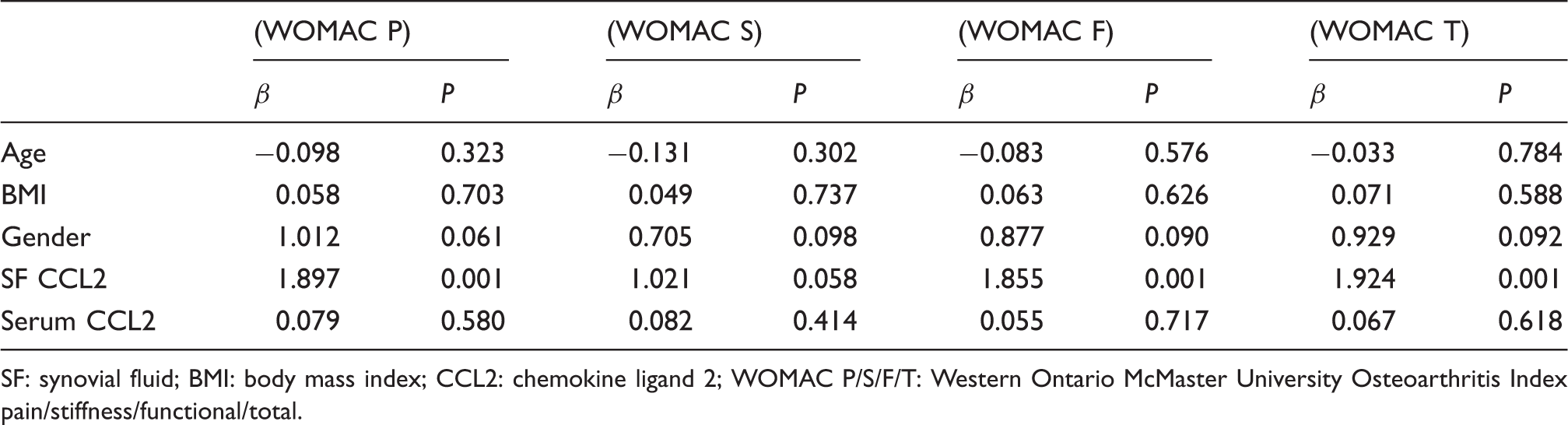
As illustrated in Figure 1, CCL2 concentrations in SF were positively correlated with WOMAC pain (r = 0.460, P < 0.001) (Figure 1(a)), WOMAC function scores (r = 0.561, P < 0.001) (Figure 1(c)) and WOMAC total scores (r = 0.443, P < 0.001) (Figure 1(d)) However, association with WOMAC stiffness scores did not reach statistical significance (r = 0.145, P = 0.067) (Figure 1(b)). The correlation between SF CCL2 concentrations and WOMAC scores was further analysed by multinomial logistic regression. Multiple regression analysis demonstrated that the association between SF CCL2 concentrations and WOMAC scores was still significant after adjusting for other confounding factors (Table 2). CCL2 concentrations in serum had no significant correlation with all WOMAC index, including pain scores (r = −0.065) (Figure 2(a)), WOMAC stiffness scores (Figure 2(b)) (r = −0.003), WOMAC function scores (Figure 2(c)) (r = 0.002) and WOMAC total scores (Figure 2(d)) (r = 0.062) (all P > 0.05) in OA patients. Nevertheless, both SF and serum CCL2 concentrations were not significantly correlated with K–L grades (Figures 3 and 4).
Association of SF CCL2 concentrations (ng/ml) with WOMAC (a) pain, (b) stiffness, (c) physical function and (d) total scores in OA patients. Association of serum CCL2 concentrations (ng/ml) with WOMAC (a) pain, (b) stiffness, (c) physical function and (d) total scores in OA patients. Association of SF CCL2 concentrations (ng/ml) with K–L grades. Association of serum CCL2 concentrations (ng/ml) with K–L grades. Multivariate linear regression. SF: synovial fluid; BMI: body mass index; CCL2: chemokine ligand 2; WOMAC P/S/F/T: Western Ontario McMaster University Osteoarthritis Index pain/stiffness/functional/total.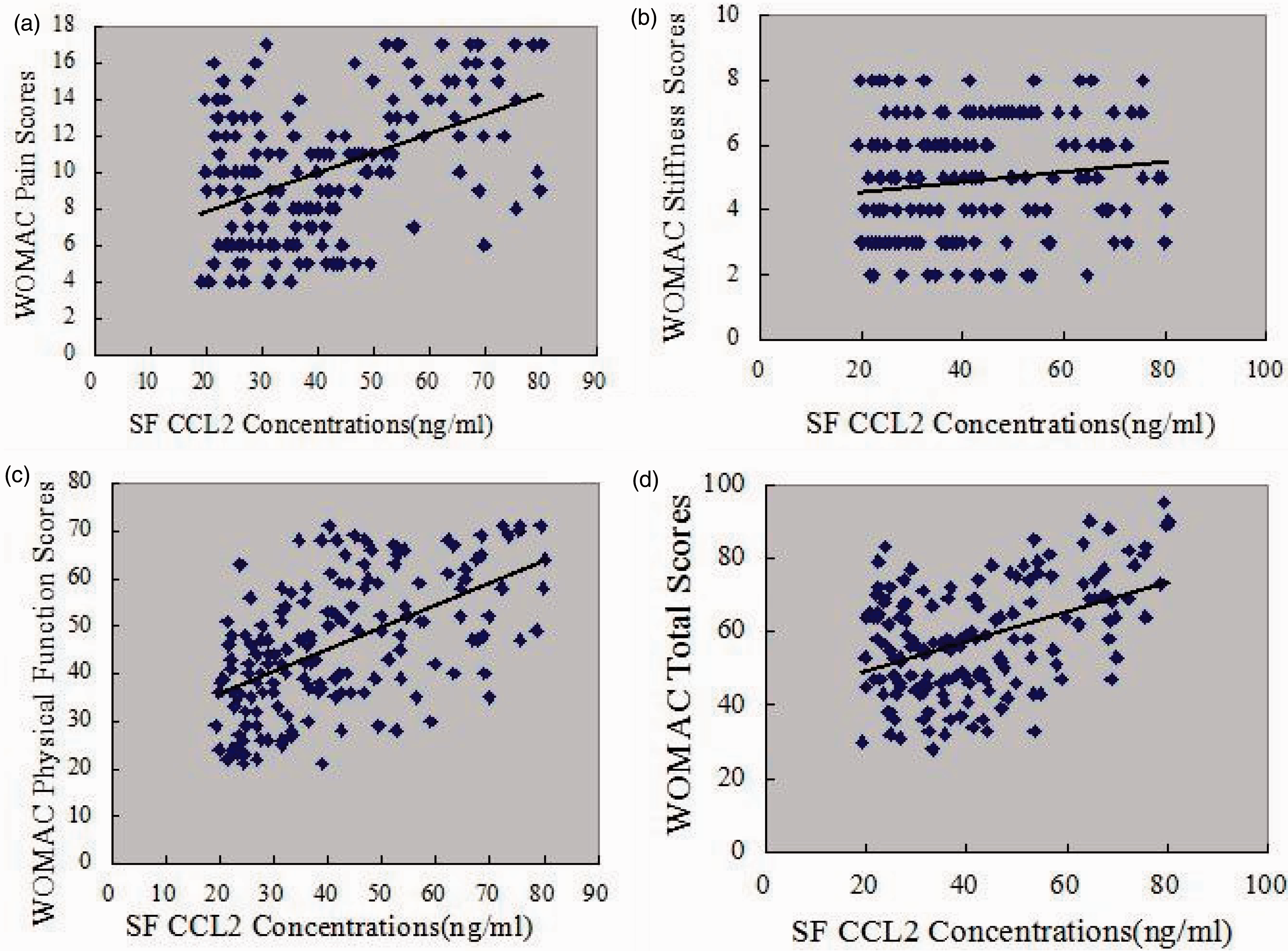
Discussion
The current research explored the correlation between serum or SF CCL2 concentrations and self-reported symptomatic severity in patients with primary knee OA. We demonstrated for the first time that SF but not serum CCL2 concentrations were positively associated with greater pain and physical disability in knee OA patients. These results indicated that CCL2 may serve as a new potential SF biomarker for reflecting the symptomatic severity in knee OA patients.
The discovery of reliable OA biomarkers provides useful diagnosis by reflecting disease-relevant condition and predicting the disease progression. In addition, novel biomarkers could help in identifying potential targets for therapeutic interventions and thus facilitate therapeutic decision making. From another perspective, the concept provided by OA-related biomarker studies represents a paradigm shift in the ways of diagnosis and intervention of OA. Studies have shown that the inflammatory element is an integral component of OA at both its early and advanced stages. 21 Forceful evidence demonstrated that chronic inflammation played a great pathophysiological role in the production and maintenance of pain in OA patients. 22 A series of cell cytokines or proinflammatory mediators have been detected in knee OA patients.21–25 Chemokines are a family of small and secreted proteins that play pleiotropic roles in inflammation-related pathological diseases. Chemokines perform in many physiological and pathological process, including those acting in the inflammation process of articular cartilage. 21 Among these, the chemokine CCL2/monocyte chemoattractant protein 1 (MCP-1), which is best known for its chemotactic functions, is mainly expressed by immune cells in various inflammatory activities.26,27 CCL2 has been explored with its presence and underlying engagement in the process of OA by several studies. It has been demonstrated that increased concentrations of CCL2 are detected in the blood, SF and synovial tissue in OA patients. 10 This is in consistent with our results. CCL2 has been proven to cause pain in animal models or articular inflammation in several animal studies.11–15 One recent study showed that CCR2/CCL2 plays a key role in balancing the bone remodelling process. 28 All these factors indicate CCL2 may act in pathogenesis or progression of OA. However, further studies should be conducted to clarify the molecular or signal pathways which CCL2 activation may exert in the pathophysiology of OA.
The main finding of the present study was that SF CCL2/MCP-1 concentrations positively correlated with WOMAC pain ratings, WOMAC function scores and total WOMAC scores. This association was still significant after adjusting for potential confounders in multivariate linear regression analysis. We also explored the correlation between SF and serum CCL2 concentrations with K–L grading system and found no significant difference in the current study, which indicates that CCL2 concentrations involved in radiographic changes in knee OA patients were not related to symptomatic severity. In multivariate linear regression analysis, we found BMI and gender were both not associated with symptoms; these may be attributed to the racial diversity, small sample size for males and single-centre study. But anyway, these results indicate that CCL2 in SF may represent a new potential biochemical marker for reflecting the severity of pain and act as a pain mediator in knee OA patients. Our findings may also provide new specific therapeutically targets for relieving pain and related symptoms.
The limitations of our research should be taken into account when discussing our results. First, the current study was cross-sectional among Chinese people with a relatively small sample size, which impaired the statistical power for evaluating the prognostic value of CCL2 in OA patients. Therefore, further multicentre and multisample studies are needed with larger scale. Second, although the WOMAC score is widely applied to assess symptomatic severity in knee OA patients, the use of WOMAC score seems always subjective and may be subject to interferences from some confounding factors. Third, we could not obtain SF samples from healthy controls for ethical concerns, and in fact, the SF volume in healthy individuals is tiny which is difficult to collect. These might lead to some bias. Fourth, we only examined serum and SF CCL2 concentrations, and additional studies on the investigation of other inflammatory cytokines like C-reactive protein, IL-1 may provide more valuable information on the disease progression role of CCL2 signalling pathways in OA-related symptoms to further confirm CCL2 uniqueness. Last, we did not assess whether the hyaluronic acid injection had an effect on the serum and SF concentrations of CCL2 in knee OA patients. Therefore, we would miss a potential mechanism of hyaluronic acid, and this is worthy of further investigation. Collectively, CCL2 concentrations in SF but not serum were positively correlated with the symptomatic severity of knee OA. CCL2 concentrations in SF may serve as a new biomarker together with the classic ways for evaluating the risk and severity of knee OA.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
This study was approved by the ethics committee of Dong Ying People’s Hospital (No. 2012DYPH006).
Guarantor
LL.
Contributorship
LL reviewed literature and proposed the study. LL and JB were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. LL wrote the first draft of the manuscript. Both authors reviewed and edited the manuscript and approved the final version of the manuscript.