
Abstract
We report a case of clinically significant micronutrient deficiencies following biliary pancreatic diversion (BPD) surgery. Our patient was admitted to hospital six years after BPD surgery following a low impact humeral fracture complicated by postoperative wound infection. On presentation she complained of a widespread rash and loss of night vision. Laboratory testing confirmed hypoalbuminaemia, deficiencies of vitamins A, E and D and of the trace elements copper, zinc and selenium. Bone densitometry confirmed osteoporosis. The skin rash was thought to be due to zinc deficiency and improved with conservative measures and trace element replacement. Her night blindness resolved 48 hours after receiving high dose parenteral vitamin A. Six months later she was readmitted to our intensive care unit with wound dehiscence at her fracture site and clinical features of sepsis and encephalopathy. This case highlights the importance of devising treatment and follow-up guidance prior to surgery and multidisciplinary team involvement including the patient so that long-term metabolic complications are avoided.
Introduction
Obesity is an increasing problem within healthcare services and 23–27% of the British population are now classified as obese. The demand for bariatric surgery is also increasing, with 8024 inpatient procedures performed within the National Health Service (NHS) in England in 2012–2013. 1
Bariatric surgery comprises of various techniques used to establish and maintain weight loss in morbidly obese individuals through either restricting intake of food, altering hunger and satiety, malabsorption or a combination of these mechanisms. 2 Commonly used techniques in the UK include laparoscopic gastric banding, Roux-en-Y gastric bypass (RYGB) and the gastric sleeve procedure. 3 Biliary pancreatic diversion (BPD) removes up to 70% of the distal stomach and bypasses the majority of the small intestine allowing for approximately just 50 cm of distal jejunum as a ‘common limb’ for mixture of ingested food and digestive intestinal enzymes. 4 BPD patients are at particular risk of nutritional complications and this technique is now less commonly used in clinical practice. 3 The ongoing prospective controlled Swedish Obese Subjects study has provided strong evidence that bariatric surgery is effective at achieving significant weight loss and reductions in cardiovascular disease risk, type 2 diabetes mellitus, hypertriglyceridaemia, cancer and overall mortality. 5
Case report
We report the case of a female bariatric patient in her late 40 s who had a BPD performed several years previously. Prior to surgery her weight was 205 kg, body mass index (BMI) 76 kg/m2 and she suffered from hypertension, type 2 diabetes mellitus and hyperlipidaemia. Her co-morbidities resolved following surgery. She was maintained on oral nutritional supplements consisting of a twice daily multivitamin and mineral preparation and varying doses of calcium and vitamin D (dose range: 500–1500 mg calcium and 200–600 units vitamin D). Follow-up and expert monitoring were limited due to non-clinical reasons.
Micronutrient and other biochemical measurements following biliary pancreatic diversion surgery.
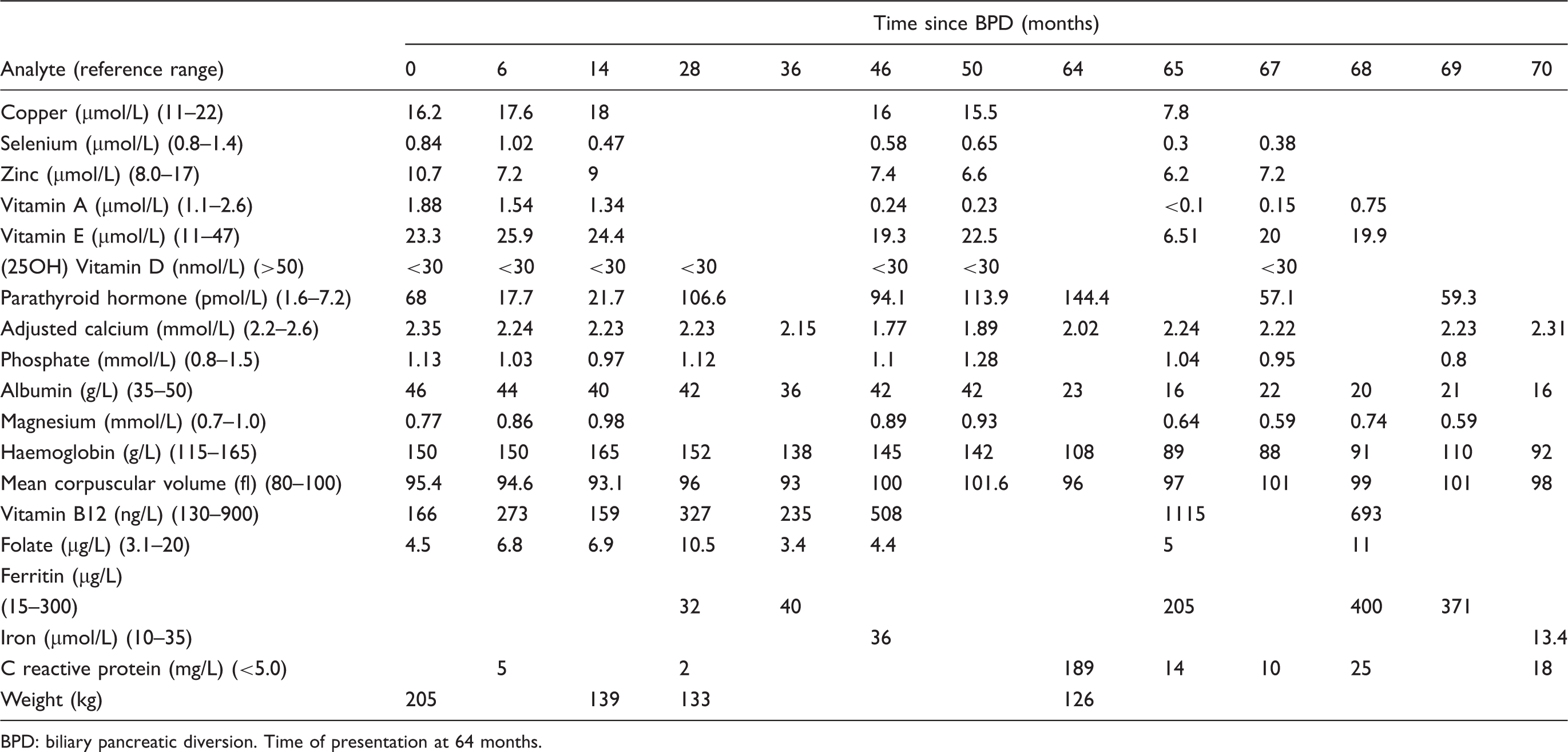
BPD: biliary pancreatic diversion. Time of presentation at 64 months.
She received 100,000 units of intramuscular vitamin A and 300,000 units of intramuscular vitamin D and her night blindness improved within 48 hours. The rash, thought to be secondary to zinc deficiency responded to conservative management and trace element supplementation. Following successful treatment of her wound infection she was discharged from hospital. A high dose outpatient vitamin and mineral replacement regimen was implemented including a 3-month course of 20,000 units oral vitamin D, a calcium and vitamin D preparation thrice daily, multivitamin and nutrient supplementation four times daily and an infusion of intravenous trace elements. Six months later she re-presented to hospital with wound dehiscence at the fracture repair site and features of sepsis and encephalopathy. She died on the intensive care unit, despite aggressive treatment.
Methods
25(OH) vitamin D was measured with a liquid chromatography-tandem mass spectrometry method (Waters Ltd., Elstree, UK). Vitamins A (retinol) and E (tocopherol) were measured using a high-performance liquid chromatography technique (Agilent Corporation, Santa Clara, CA, USA). Trace elements were assayed using inductively coupled plasma mass spectrometry (Agilent). All other routine chemistry and haematology analyses were carried out on automated platforms (Abbott Architect [Abbott Diagnostics, Maidenhead, UK] Hobira Pentra [Hobira Medical, Montpellier, France] respectively).
Discussion
Obesity is associated with reduced concentrations of 25(OH) vitamin D.4,6 Malabsorptive procedures, especially BPD are particularly restrictive of fat-soluble vitamin uptake and calcium deficiency is also observed. 7 Together these are associated with a subsequent risk of fracture. Although our patient was maintained on various calcium and vitamin D supplements following surgery, long-term compliance and doses taken were variable.
Vitamin A deficiency has been observed in up to 70% of patients following BPD surgery although ophthalmic symptoms are often not immediately recognized.8,9 Parenteral replacement is quick and effective in treating visual disturbance as was evident in our patient.
Thiamine deficiency has been described in up to 49% of RYGB patients. Symptomatic deficiency and development of Wernicke’s encephalopathy has been recognized following all weight loss procedures and can manifest as an early and acute complication. 4 Current recommendations are for routine replacement in all patients and to have a low threshold for intravenous replacement if patients become unwell. 10 Encephalopathy in some patients has been proposed to be secondary to multiple micronutrient deficiencies. 11 In our patient we surmised that the aetiology of the encephalopathy was metabolic and she was treated with intravenous thiamine replacement. She also received treatment for hepatic and septic causes.
Copper and zinc deficiency is recognized in patients with obesity and following bariatric surgery.12,13 Copper is particularly important for iron absorption and can cause anaemia, leukopaenia and rarely pancytopaenia. 13 Other manifestations are neurological, which can be mistaken for more commonly observed vitamin B12 deficient symptoms. Obesity-induced inflammation can give falsely reassuring results. 6 Low concentrations of zinc are associated with diarrhoea, emotional disorders, weight loss, infection, dermatitis, hair loss, poor wound healing and blunted taste.2,6 Supplementation of zinc needs to be considered in conjunction with copper replacement due to its interference with copper absorption. 6
In the context of inflammation laboratory measurements of 25(OH) vitamin D, serum retinol, zinc and selenium can be low due to an acute phase response. 14 This may not reflect true deficiency and may confound results. In our patient the clinical features correlated with the laboratory findings.
Conclusion
Obese patients are at risk of developing severe micronutrient deficiency following bariatric surgery, in particular with malabsorptive procedures such as BPD. Inflammation produces confounding results in several serum markers, and this needs to be considered when interpreting results to prevent unnecessary treatment. Bariatric surgery is an effective intervention for morbidly obese individuals; however, this does not come without risk. It is therefore imperative to ensure patients and clinicians are educated on the potential nutritional harm of the procedures and that those continuing care for these patients are well informed on how to monitor for and treat any nutritional complications encountered.
There is global recognition of the importance of monitoring nutrient status in these patients. The extent of micronutrient testing varies amongst guidelines and surgical procedures.10,15,16 European guidelines recommend annual monitoring following RYGB and measurement at 1, 4, 12 months and then annually thereafter for BPD. Suggested serum nutritional markers include vitamin B12, 25(OH) vitamin D, parathyroid hormone, ferritin, calcium and albumin; trace elements however are not mentioned. Daily supplementation is necessary and it has been advised that parenteral replacement be considered if deficiency develops. 17 The National Institute for Health and Care Excellence advises that patients undergoing bariatric surgery should be committed to long-term follow-up and have regular dietetic input including micronutrient monitoring. 18 Emphasis in guidance is placed upon multidisciplinary follow-up and individual assessment.
Most deficiencies are preventable and treatable with high dose supplementation and complications such as low-impact fractures or encephalopathy should alert clinicians to consider further nutritional investigations or treatment. With increased awareness of the potential nutritional consequences of bariatric surgery, life-threatening complications may be avoided.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
None.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
It was not possible to obtain informed consent from the patient or next of kin in this report. The journal has taken the decision to publish this case in the public interest.
Guarantor
DD.
Contributorship
HW wrote the first draft of the manuscript. Subsequent manuscripts were reviewed, edited and approved by DD.