
Abstract
Background
Laboratory services in the UK have witnessed an annual increase in requesting activity often with no associated increase in budget. This study evaluated the impact of different demand management strategies on biochemistry test requesting activity from a tertiary Intensive Care Unit (ICU) at a UK teaching hospital.
Method
We conducted an observational longitudinal study in which biochemistry requesting activity from the ICU was gathered over five separate six-month periods between 2009 and 2013. During this time, two different strategies aimed at reducing inappropriate biochemistry requesting were in use and the effects of the two strategies were compared.
Results
Implementation of minimum re-testing intervals (MRIs) resulted in an overall 22.7% reduction in total requesting activity in the first year with minor change in clinical workload. In the second year, a 13.3% rise in requesting activity was seen but this was against a background of a 14.6% increase in ICU workload. Removal of the MRIs rules associated with the introduction of an ICU test testing schedule resulted in a 13.4% reduction in total requesting activity in the first year. ICU workload during this year was 1.8% lower than the previous year. In the final year, requesting activity was almost unchanged but ICU workload grew by 6.8%.
Conclusion
Implementation of MRIs reduced biochemistry test requesting activity on the ICU. Introduction of an agreed test schedule and removal of the MRIs, however, produced a further reduction in ICU requesting activity. Variation in ICU workload does not account for all the observed changes.
Introduction
There is published evidence that up to 25% of all laboratory tests are perceived as inappropriate.1,2 Despite this, most laboratories continue to witness an 8–10% increase in workload year on year, often without a matching increase in budget. 3 There is a need to find measures to reduce unnecessary testing while maintaining quality of care. There have been many reported strategies to manage increasing demand by reducing inappropriate or unnecessary testing. These include changing request card design,4,5 introducing minimum re-testing intervals (MRIs), education, audit and feedback, computerised physician order entry systems with real time decision support 6 and funding/financial models. 7 A quality report in Australia 7 looked into many of these strategies and although all appear to have the capacity to deliver success, there was no consensus on the best strategy for broader adoption in the long term, with sustainability remaining particularly problematic. The consensus opinion has been generally supportive of the MRIs approach,8,9 though a multi-faceted approach is ideal. 10 The rationale for implementation of MRIs is based on the properties of the test, biological half-life, treatment and monitoring requirements, established guidance and the particular clinical situation. The Association of Clinical Biochemistry and Laboratory Medicine has recently published national guidance on MRIs with evidence-based recommendation 11 and others have devised a laboratory tool-kit to aid the development of demand management strategies. 10
The University Hospital of Wales (UHW) is a teaching hospital with over 1000 beds, with an average daily bed occupancy of 86.8% in 2011–2012. 12 The adult Intensive Care Unit (ICU) comprises of 33 beds split according to need between level 2 (high dependency) and level 3 (intensive care) beds with a bed occupancy in excess of 95% and approximately 1300 admissions per year.
In January 2010, UHW Medical Biochemistry department implemented MRIs rules across all disciplines including ICU. Requests that breach the set MRIs [72 h for liver (LFT) and bone profiles and 24 h for C-reactive protein (CRP)] are only processed without direct contact if the request is justified by the clinical team. Prior to 2010, standard practice for the ICU was to request renal profile (urea/electrolytes), LFT, bone profile, CRP and magnesium (Mg) on all patients on a daily basis. Data for the four years preceding this study period demonstrated an annual increase in biochemistry requests of between 5 and 14%.
In 2012, ICU consultants decided that the use of MRIs in an ICU setting was not helpful and proposed switching to a standard testing schedule. A full profile [urea/electrolytes (urea, creatinine, sodium and potassium), bone profile (calcium, albumin, alkaline phosphatase, total protein and calculated globulin), LFT (total protein, albumin, bilirubin, alanine aminotransferase, alkaline phosphatase), calcium, albumin, magnesium, phosphate, CRP, full blood count and coagulation screen] was done three days a week (Monday, Wednesday and Friday), with urea/electrolytes being the only biochemistry test performed on the other four days. Any additional biochemistry tests felt to be clinically required could be requested by the duty ICU consultant. The new requesting guidelines were agreed between the Medical Biochemistry department and senior ICU staff. An educational programme was undertaken for the trainee medical and nursing staff and the new testing schedule was introduced in February 2012. To facilitate the requesting of the correct tests for the day of the week, a standard test request ‘ICU Profile’ was introduced.
Aim
The aim of this study was to assess retrospectively the impact and sustainability of two demand management strategies on the biochemistry test requesting activity of the Intensive Care unit at the University Hospital of Wales.
Method
Data on ICU requesting activity were gathered for the period between 1 March to 31 August each of the years 2009 to 2013 inclusive. The six-month period in 2009, when no demand management interventions were applied, is provided for comparison. The MRIs were introduced in 2010 and requesting activity was gathered for the same six-month period in 2010 and 2011. The standard ICU testing schedule was implemented in 2012; data were gathered for the same six-month periods in 2012 and 2013. As the implementation dates for the two interventions were not the same each year, a six-month period post intervention was chosen for comparison.
Results
Total number of biochemistry sets, ICU workload and year on year percentage change (%) in the different six-month periods.
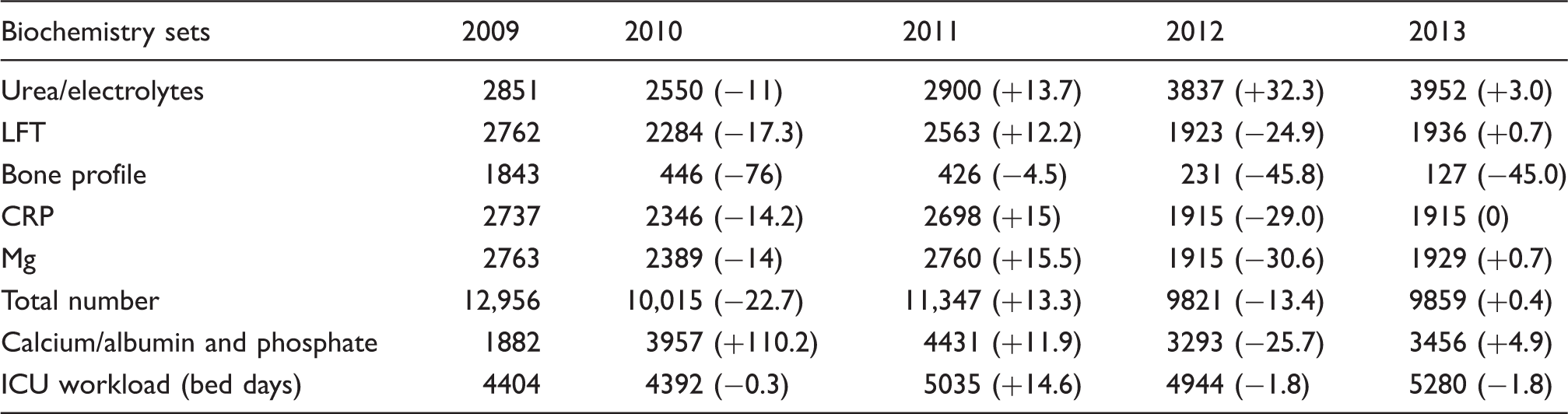
Following implementation of the ICU testing schedule in 2012, requesting activity reduced by 13.4% compared to the previous year in association with a reduction in ICU workload of 1.8%. In the final year of the study (the second year of the ICU testing schedule), requesting activity increased by less than 5% but with an increase in ICU workload by 6.8%.
Discussion
MRIs have been broadly recommended as a demand management tool which can be implemented easily and reliably within laboratory systems. The data presented here support in part the value of this approach in controlling requesting activity. In the UHW ICU, the implementation of MRI led to a marked reduction in requesting activity initially but this was not sustained in the following year possibly due to a rise in ICU workload.
The implementation of ICU testing schedule was undertaken along with continuous education and evaluation by both ICU and biochemistry staff. This was associated with 13.4% reduction in requesting activity compared to the previous year. Some but not all of this change may be attributed to a 1.8% reduction in ICU workload over the same time period. In the final year of the study (the second year of the testing schedule), requesting activity was unchanged despite an increase in ICU workload by 6.8%.
Bone profile requests showed a continuous reduction across the study period. Nevertheless, both calcium and phosphate requests had shown an increase in requesting which was marked during the period of MRI implementation. Clinicians suggest this may have been an attempt by clinical staff to circumvent the bone profile MRIs. The ICU testing schedule did not seek to target urea/electrolytes requesting as daily testing was felt to be clinically indicated and in fact urea/electrolytes requesting increased over the observation period (Table 1).
One limitation of the study was the absence of a second ‘control’ period between the two interventions. Given the positive impact of the MRIs, a second control period would have been a retrograde step that would most likely have increased testing and associated costs. It should be noted that ICU workload has varied over the study period with both increases and decreases and against this background a second ‘control’ period would not necessarily have provided useful information. There were no major re-configurations of the clinical service during the study period to account for the observed variation in workload. These changes most likely represent the effects of the H1N1 influenza pandemic along with the general annual increase in ICU workload which is currently estimated at 4–5% per year.
We have not presented the results of the reduction in serum glucose and routine urine testing during the intervention period. Point of care testing for glucose was introduced during the study period and this probably led to reduction in laboratory glucose measurement seen. Data from the point of care testing are not held centrally and cannot therefore be obtained retrospectively and analysed. Urine testing was never addressed by either the MRIs or the blood test schedule, but nevertheless showed a marked reduction in requesting activity. We believe that the ‘cultural’ change introduced by ITU testing schedule was largely responsible for this reduction.
Conclusion
Both MRIs and ICU testing schedule interventions reduced biochemistry requesting activity on our tertiary ICU when workload was taken into account. The introduction of the ICU testing schedule produced further gains over those already achieved by the MRIs intervention and therefore appears to have been more effective in our ICU. We believe that this is due largely to the collaborative approach taken. Any intervention aimed at reducing inappropriate requesting is more likely to be successful if it engages the clinical teams and results in a mutually agreed approach.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Not applicable.
Guarantor
SZ.
Contributorship
SZ and HR were involved in implementation of demand management strategies. Data were analysed and the first draft was written by ST. Further changes and significant contributions were made by all authors, and the final draft was agreed by all authors.